- Published by:
- Department of Families, Fairness and Housing
- Date:
- 19 Dec 2019
Evaluation of new community-based perpetrator interventions and case management trials
Executive summary
Introduction
The Royal Commission into Family Violence (the Royal Commission) found that existing interventions for perpetrators of family violence in Victoria were not sufficiently broad nor diverse. Apart from a small number of programs for some minority cohorts, there was limited diversity in interventions for perpetrators of family violence.
In response to Recommendation 87 of the Royal Commission, two trial programs were developed; perpetrator case management and seven community-based perpetrator intervention trials targeting specific cohorts (cohort trials).
This evaluation was led by Deloitte Access Economics, and undertaken with the Social Research Centre. The evaluation objectives were to determine whether the funded activities:
- were implemented according to plan
- achieved their stated objectives
- met the needs of the target cohort and victim/survivors to a greater extent than existing programs
- presented a more effective service response.
Justification and appropriateness
The Royal Commission identified that mainstream Men’s Behaviour Change Programs (MBCPs) are not easily accessible or are not relevant for a number of people who use violence. It also found that existing, group based MBCPs are, by their nature, not designed to work with participants individually, to provide a more intensive service where necessary.
The models employed by the cohort trials have been designed or adapted to address the specific needs of these different cohorts, often drawing on approaches used overseas as they address gaps in the mainstream service delivery models typically used in Australia.
Case management provides individualised and timely responses to perpetrators. It addresses and coordinates service delivery according to the complex needs of the perpetrator (e.g. alcohol and other drug (AOD) misuse, mental/physical health concerns, gambling or homelessness). Case management has now been funded on an ongoing basis.
In the request for submissions process for the cohort trials, no trials were funded specifically addressing mental health and AOD issues due to the lack of suitable submissions targeting these cohorts.
Lessons from practice
This evaluation has determined six key features that have been observed in the current practices of the providers delivering the new cohort trials and case management. These features align with evidence of specific approaches that better enable previously excluded or under-serviced groups to benefit from government funded perpetrator interventions, such as trauma-informed practices, integrated response models, and cultural healing:
- Creating trusting relationships between participants and facilitators, and among group members to encourage engagement and participation.
- Utilising both individual and group work in a complementary manner.
- Addressing accountability with a trauma informed approach to address the underlying factors contributing to violent behaviour.
- Facilitating a holistic, wrap-around approach to address contextual factors in a person’s life by connecting them to the broader service system.
- Allowing flexibility in approach for people with different levels of need and at varying stages of change.
- Providing support to people who experience violence via a family safety contact.
Approaches for specific cohorts
While there are overarching design features that contribute to good practice, there are also specific features of program design that are appropriate for particular cohorts.
For Aboriginal cohorts, cultural healing and connection to culture and country is necessary, so they are able to first address their own healing from past trauma and grief, in order to subsequently address their use of violence. Engagement with Elders, sufficient time to deliver and implement the programs, meaningful partnerships and Aboriginal self-determination in design and delivery are important.
There are some parallels for the LGBTI and women who use force cohorts in terms of enabling participants to heal from violence/trauma and the use of peer support.
The program for culturally and linguistically diverse (CALD) participants delivered the program in a culturally appropriate manner, including applying a cultural lens to mainstream materials, and having facilitators who belonged to the two cultural groups.
For people with cognitive impairment, the program is a more resource-intensive version of the MBCPs. This is because the small group size, slower pace, specialist workforce and closed group are important features contributing to participant engagement (but are also more resource intensive). Using prompts and visuals has also been beneficial.
Early client achievements
Some early client achievements as a result of participating in the cohort trials and case management have been identified. Due to the short amount of time that has passed since the commencement of the programs, these findings are not definitive, however they demonstrate positive signs at this point in time.
- Providers of cohort trials and case management reported that participants have been demonstrating high levels of engagement compared with their experience facilitating mainstream programs.
- Some participants reported increased understanding of what constitutes family violence, particularly non-physical forms of violence, and how their behaviour affected others.
- There were mixed findings regarding participants taking responsibility for their behaviour, however this is to be expected given the short-term nature of the programs compared to the long-term process of behaviour change.
- Participants acknowledged that they would need to continue to work on implementing strategies in order for them to become ‘learned behaviours’. Many reflected the need for continued support beyond the life of the program.
- The programs are contributing to a greater level of risk management of people who use violence, particularly those with complex needs. By engaging people who use violence who were previously not accessing services, these programs are ‘keeping them in view’, which enables providers to better identify and manage risk.
- People who experience violence reported that the support they received had helped them to feel less isolated, and a number indicated their feelings of safety had improved.
Implementation – workforce and process
The evaluation examined the activities and processes that were involved in establishing the cohort trials and case management, and made the following findings:
- Attracting staff with the appropriate skills and experience in working with people who use violence was a particular challenge for some cohort trial and case management providers. The initial 12 month funding allocation reportedly affected the ability of providers to recruit and retain the workforce.
- Referral pathways into programs from the community and justice settings needs to better understood and defined, as people who use violence traverse both systems.
- There are some challenges to effective service coordination across the sector, including a lack of capacity or willingness to work with people who use violence.
- Performance management of the programs needs to be strengthened, to ensure there is accountability and consistency for reporting on program outcomes.
Conclusion and future considerations
Overall, it has been established that the perpetrator cohort intervention trials and case management are addressing a service delivery gap for people using violence, and have contributed to delivering on Recommendation 87 of the Royal Commission. This evaluation report identifies several areas for ongoing improvement or enhancement, particularly as the programs transition from pilots to ongoing funding (case management) or providing services for an additional year (cohort trials). There are eight overarching improvement opportunities, and three that relate to cohort interventions.
- building the focus on the role of the family safety contact
- strengthening the referral pathway by raising awareness of the programs within the service system
- contributing to building workforce capability
- improving accountability, governance and reporting of the programs through FSV
- providing improved exit planning for case management participants
- providing clarity around funding
- adopting a systems approach by creating alignment with the justice perpetrator programs
- long-term research and evaluation
- tailoring implementation and reporting targets for Aboriginal cohorts (cohort specific)
- building capability within the mental health and AOD workforces to encourage the design of suitable programs for these cohorts (cohort specific)
- consider opportunities to scale the programs (cohort specific).
Deloitte Access Economics is Australia’s pre-eminent economics advisory practice and a member of Deloitte's global economics group. For more information, please visit our website: www.deloitte.com/au/deloitte-access-economics
Deloitte refers to one or more of Deloitte Touche Tohmatsu Limited (“DTTL”), its global network of member firms, and their related entities. DTTL (also referred to as “Deloitte Global”) and each of its member firms and their affiliated entities are legally separate and independent entities. DTTL does not provide services to clients. Please see www.deloitte.com/about to learn more.
Deloitte is a leading global provider of audit and assurance, consulting, financial advisory, risk advisory, tax and related services. Our network of member firms in more than 150 countries and territories serves four out of five Fortune Global 500®companies. Learn how Deloitte’s approximately 286,000 people make an impact that matters at www.deloitte.com.
Deloitte Asia Pacific
Deloitte Asia Pacific Limited is a company limited by guarantee and a member firm of DTTL. Members of Deloitte Asia Pacific Limited and their related entities provide services in Australia, Brunei Darussalam, Cambodia, East Timor, Federated States of Micronesia, Guam, Indonesia, Japan, Laos, Malaysia, Mongolia, Myanmar, New Zealand, Palau, Papua New Guinea, Singapore, Thailand, The Marshall Islands, The Northern Mariana Islands, The People’s Republic of China (incl. Hong Kong SAR and Macau SAR), The Philippines and Vietnam, in each of which operations are conducted by separate and independent legal entities.
Deloitte Australia
In Australia, the Deloitte Network member is the Australian partnership of Deloitte Touche Tohmatsu. As one of Australia’s leading professional services firms. Deloitte Touche Tohmatsu and its affiliates provide audit, tax, consulting, and financial advisory services through approximately 8000 people across the country. Focused on the creation of value and growth, and known as an employer of choice for innovative human resources programs, we are dedicated to helping our clients and our people excel. For more information, please visit our website at https://www2.deloitte.com/au/en.html.
Liability limited by a scheme approved under Professional Standards Legislation.
Member of Deloitte Asia Pacific Limited and the Deloitte Network.
© 2019 Deloitte Access Economics. Deloitte Touche Tohmatsu.
Introduction
1.1 Program purpose
Family Safety Victoria (FSV) has established two new trial programs for perpetrators of family violence, which address the needs of a more diverse range of perpetrators, and are better integrated into the wider response to family violence in Victoria.
1.1.1 Recommendation 87 of the Royal Commission into Family Violence
The Royal Commission into Family Violence (the Royal Commission) found that existing interventions for perpetrators of family violence were not sufficiently broad nor diverse. Apart from a small number of programs for men from culturally and linguistically diverse (CALD) background, Aboriginal men, and the Lesbian, Gay, Bisexual, Transgender, and Intersex (LGBTI) community, there was limited diversity in interventions for perpetrators of family violence. For example, the Royal Commission heard that people who misuse alcohol or other drugs, or have mental health issues, found it difficult to engage in these interventions[1]
Historically, the main intervention targeted at perpetrators in Victoria have been Men’s Behaviour Change Programs (MBCPs). MBCPs are designed to assist men to take accountability for their actions and to end their use of violence and other problematic behaviour in their relationships. They are intended to assist in facilitating the behavioural changes necessary to build healthy and respectful relationships. MBCPs include a family safety contact function, who works with the person who experiences violence to ensure they are connected to services as required and are kept safe and in sight. The Royal Commission found MBCPs to be inadequate in being able to provide tailored support to address individual needs and risks.
In March 2016 the Victorian Royal Commission released 227 recommendations to reform the state’s response to family violence. Recommendation 87 of the Commission suggests the Victorian Government “research, trial and evaluate interventions for perpetrators [within three years]”, including interventions that:
- provide individual case management where required
- deliver programs to perpetrators from diverse communities and to those with complex needs
- focus on helping perpetrators understand the effects of violence on their children and to become better fathers
- adopt practice models that build coordinated interventions, including cross-sector workforce development between the men’s behaviour change, mental health, drug and alcohol and forensic sectors” [2].
The Royal Commission found that the range of perpetrator interventions needed to be broader and better integrated within the scope of initiatives targeting family violence, creating a “web of accountability” to keep perpetrators in view and protect victims and families.
In response to this recommendation, FSV have developed two new programs; perpetrator case management and community-based perpetrator intervention trials (cohort trials).
1.1.2 Perpetrator case management
One of the new approaches to address the shortcomings of current programs is the implementation of a new case management model for perpetrators of family violence.
Case management provides individualised and timely responses to perpetrators. It addresses and coordinates service delivery according to the complex needs of the perpetrator (e.g. alcohol and drug misuse, mental/physical health concerns, gambling or homelessness). Besides ensuring perpetrators are in view of service providers and relevant authorities, case management aims to directly increase the safety of victims via a number of methods. This includes providing a platform to engage with victims through a Family safety contact, and identifying relevant information (shared under the Family Violence Information Sharing Scheme) to contribute to risk assessment and management for victim safety. Case management also helps involve the perpetrator in planning and decision making to encourage engagement with other social activities and universal services.
The approach to case management consists of developing strategies and skills to stop the perpetrator’s use of violence, as well as increasing their motivation for change. Perpetrators under case management are assisted in:
- recognising abusive patterns and tactics
- seeing the relevance in their engagement with support services and long-term behaviour change, and
- taking responsibility for their violence through their engagement with support services such as MBCP [3].
Funding provides for an average of 20 hours per participant.
Case management was targeted at perpetrators who:
- have been removed from the home and require practical support;
- are deemed unsuitable for MBCPs. This could be due to:
- English not being a primary language
- having complex needs (mental health, alcohol and other drug issues (AOD), homelessness, cognitive impairment and acquired brain injury) and require support, or
- being at risk from other perpetrators.
- are attending a MBCP and require additional support to stay engaged, including those at risk to themselves, or
- require additional support after the conclusion of a MBCP [4].
Referrals to case management occur primarily through existing intake services and Orange Door locations. This includes police referrals, the Men’s Referral Service, and informal referrals (such as Child Protection, family services, or other pathways).
The providers by area are listed in Table 1.1 below. Further detail on each provider by area, is shown in Table 1.1.
Table 1.1: Providers by DHHS area
|
DHHS Area |
Provider |
|
Bayside Peninsula |
|
|
Southern Melbourne |
|
|
North Eastern Melbourne |
|
|
Western Melbourne |
|
|
Hume Moreland |
|
|
Brimbank Melton |
|
|
Outer Eastern Melbourne |
|
|
Inner Gippsland |
|
|
Inner Eastern Melbourne |
|
|
Barwon |
|
|
Loddon |
|
|
Central Highlands |
|
|
Goulburn |
|
|
Wimmera South West |
|
|
Mallee |
|
|
Ovens Murray |
|
|
Outer Gippsland |
|
*Aboriginal Community Organisation or mainstream provider delivering dedicated Aboriginal targets
1.1.3 Cohort trials
FSV is providing funding to trial new community-based cohort trials. Under the new program design, the scope of perpetrator interventions has increased in order to target more diverse perpetrator cohorts who were not being adequately serviced by the mainstream system.
The scope of the cohort trials has been structured as follows:
- two targeted to men with cognitive impairment
- two targeted to Aboriginal (or non-Aboriginal) fathers in Aboriginal families
- one targeted to women who use force
- one targeted to cis women (heterosexual, bisexual and lesbian), transgender and gender diverse people who use violence, and
- one targeted to migrants/refugees from Hazara (Afghani) and South Asian communities.
Further detail on each trial, including the approach and location, is shown in Table 1.2.
Table 1.2: New perpetrator cohort trials
|
Agency (lead and partner) |
Target of trial |
Approach |
Coverage of the trial |
|
Bethany Community Support |
Men with cognitive impairment |
MBCP |
Barwon |
|
Drummond Street |
cis women (heterosexual, bisexual and lesbian), transgender and gender diverse people who use violence |
Mix of one-to-one and group responses |
North East Melbourne |
|
Anglicare and VACCA |
Aboriginal and non-Aboriginal fathers |
Cultural healing approaches |
Bayside Peninsula |
|
Baptcare and Berry st |
Women who use force, including Aboriginal women |
Therapeutic group setting |
Central Highlands |
|
Peninsula Health |
Men with cognitive impairment and/ or learning disabilities |
Group and one-on-one interventions |
Bayside Peninsula |
|
Bendigo and District Aboriginal Co-operative |
Aboriginal fathers and non-Aboriginal fathers with Aboriginal families. |
Healing and re-storying/reflective practices in the bush setting |
Loddon |
|
InTouch Multicultural Centre Against Family Violence |
Newly arrived migrants and refugees from the Hazara (Afghani) and South Asian communities Introduction in 2019-20 of programs for African and younger men (18-20 years) |
In-language, culturally informed interventions |
Southern Melbourne |
Source: Family Safety Victoria (2018a)
Evaluation approach
2.1 Evaluation – purpose, role and scope
This evaluation is a requirement of Recommendation 87 of the Royal Commission. The evaluation findings are intended to inform and improve policy and drive system improvement, making it more responsive to the needs of our diverse Victorian community.
The evaluation was conducted by Deloitte Access Economics, with support for the qualitative research with people who experience and use violence undertaken by the Social Research Centre.
The evaluation objectives were to determine whether the funded activities:
- were implemented according to plan
- achieved their stated objectives
- met the needs of the target cohort and victim/survivors to a greater extent than existing programs
- presented a more effective service response. [1]
- the evaluation will also assist to inform future funding decisions, and therefore aligns with the lapsing program guidelines as stipulated by the Department of Treasury and Finance.
The evaluation commenced in September 2018, with the first data collection phase (process) occurring in April – June 2019, and the second data collection phase (outcome) occurring in August – October 2019. Prior to the data collection, there was an extensive period of evaluation planning, including the process of gaining ethics approval from the Australian National University Human Research Ethics Committee (ANU HREC). Evaluation of the MBCP group work element was not in scope of this evaluation.
The evaluation involved two phases:
- Interim (process) evaluation – reviewed implementation of the funded trials. This part of the evaluation considered whether the trials are being delivered at the standard and volume outlined in the service agreement, and whether they are acceptable and accessible to their target cohorts. It also considered whether the programs are achieving their desired short-term outcomes.
- End of program (impact) evaluation – assessed the extent to which the funded trials met the needs of the target cohorts and achieved their desired outcomes.
In order to inform the evaluation and key lines of enquiry, a series of evaluation questions were developed. These included both process and outcome evaluation questions. The evaluation questions considered the appropriateness, effectiveness and efficiency of the initiatives.
Table 2.1 categorises the process evaluation questions under one of the three evaluation domains (appropriateness, effectiveness, efficiency). Questions were developed based on those outlined in the Request for Proposal, the Department of Treasury and Finance’s Lapsing Program Evaluation guidelines, and advice from Deloitte Access Economics. The questions were further refined following a workshop with a selection of service providers of the trial programs held in November 2018. Questions taken from the Mandatory Requirements for Lapsing Program Evaluation document are italicised. This evaluation is not a Lapsing Program Evaluation, but does incorporate the Department of Treasury and Finance’s Lapsing Program Evaluation questions.
Table 2.1: Evaluation questions
| Evaluation domains | Evaluation questions |
|---|---|
| Process Evaluation Questions | |
| Appropriateness/Justification |
What is the evidence of continued need for the initiatives and role for government in delivering the initiatives? (P1) Have the initiatives been implemented as designed? (P2) How are the initiatives innovative and contributing to best practice? (P3) |
| Effectiveness |
Are there early positive signs of change that might be attributable to the initiatives? (P4) To what extent are the outputs being realised? (P5) Have people who use violence and people who experience violence responded positively to the program, including enrolment, attendance/retention and satisfaction? (P6) What are the barriers and enablers to effective referral of participants? (P7) What governance and partnership arrangements been established to support the implementation of the initiatives and are these appropriate? (P8) Do the program workforces have a clear idea of their roles and responsibilities? (P9) What components of the model are perceived to be the most valuable? (P10) What improvements to the service model could be made to enhance its impact? (P11) Have there been any unintended consequences, and if so, what have these been? (P12) |
| Efficiency | Has the department demonstrated efficiency in relation to the establishment and implementation of the programs? (P13) |
| Impact Evaluation Questions | |
| Appropriateness/Justification |
Are the programs responding to the identified need/problem? (I1) What are the design considerations of the program to support scalability? (I2) |
| Effectiveness |
Have the program inputs, activities and outputs led to the desired change mapped out in the program logic? (I3) To what extent have people who use violence and people who experience violence responded positively to the program, including enrolment, attendance/retention and satisfaction? (I4) What are the drivers for effective participant engagement in the programs? Does this differ according to the different cohorts? (I5) What is the impact of the program on victims/survivors’ perceptions of safety? (I6) What are the barriers and facilitators to the programs being integrated into the broader service system? (I7) What impact have the programs had on the management of risk associated with this cohort? (I8) What impact have the programs had on referral pathways and information transfer between community services and relevant authorities? (I9) What impact have the programs had on the confidence, knowledge and skill of the case management and service delivery workforces in supporting the target cohort in the community? (I10) Are key stakeholders, including the program workforces, supportive of the model? (I11) What would be the impact of ceasing the programs (for example, service impact, jobs, community) and what strategies have been identified to minimise negative impacts? (I12) |
| Efficiency |
Have the programs been delivered within its scope, budget, expected timeframe, and in line with appropriate governance and risk management practices? (I13) Does the initial funding allocated reflect the true cost required to deliver the programs? (I14) |
2.2 Indicators of program effectiveness
To address each of the evaluation questions, a series of performance indicators were identified. These are presented in Appendix A. In addition to mapping each performance indicator to an evaluation question, the measure and data source(s) required to measure each indicator is provided.
Evaluation findings are strengthened through multiple sources of evidence (i.e., triangulation and validation of results). As such, for each evaluation question, multiple performance indicators from various data sources have been collected to provide a broad range of perspectives. Where practical, both quantitative and qualitative data was used.
2.3 Ethics approval
Ethics approval for the evaluation was granted by the HREC, through three separate ethics applications:
- a low risk application, for data collection with providers, referral organisations, peak bodies and government employees.
- a high risk application, for data collection involving people who use and experience violence.
- an application for data collection involving Aboriginal and Torres Strait Islander participants.
Gaining approval from the ANU HREC necessitated extensive consultation with Aboriginal stakeholders, including the Dhelk Dja Priority 5 sub-working group, who reviewed the evaluation approach and subsequent reports [2].
2.4 Data Collection
The data collection involved a mix of primary and secondary data collection, as summarised below. Further detail is provided in Appendix B.
2.4.1 Primary data sources
Primary data sources included both qualitative interviews and a data collection tool, as described below:
- Stakeholder interviews – consultations with non-clients, including individual providers, FSV and DHHS representatives, coordination and referral staff, and advisory and peak bodies.
- Client interviews – a total of 87 interviews were conducted with program participants, including both face-to-face and telephone. The sampling and recruitment approach is outlined in Appendix C.
- Service provider data collection tool – to address gaps in data availability from the Integrated Reports and Information System (IRIS) system, the data management system used by FSV/DHHS for family violence programs, data was sought directly from service providers through a data collection tool. For each program participant and victim survivor, the tool included demographic, referral and outcome information.
The limitations related to this data are discussed in Section 2.5. An evaluation readiness tool was developed to understand the data being collected by all providers to inform the preferred approach for recruiting people who use violence and people who experience violence for primary data collection, and to identify any planned or current evaluation activity being undertaken by providers.
2.4.2 Secondary data sources
There were two secondary sources of data used to inform the analysis in this report. This included:
- FSV/DHHS data – including program and provider details, e.g. program duration, anticipated caseloads, recruitment approach, internal evaluation details, brokerage data, and governance terms of reference; deidentified participant information from the DHHS IRIS case management system, and other documentation provided by service providers, such as grant applications, acquittal reports, etc.
- Literature scan – a literature scan focused on best practices in case management and interventions for perpetrators of family violence was conducted.
2.5 Limitations of the research
Limitations pertaining to sample size and composition, participant eligibility criteria, and provider data collection and analysis were encountered throughout the evaluation data collection approach. Findings presented in this report should be considered in the context of these limitations.
2.5.1 Sample size and composition
Firstly, the findings should be interpreted in the context of the overall sample composition. People who have experienced violence were difficult to engage in the research, with only 18 participants interviewed (compared to 69 people who have used violence). This presents difficulties when corroborating the feedback from people who have used violence with those who have experienced violence. This is an important limitation, as people who have experienced violence are considered to have a more objective point of view, particularly as it relates to observing any outcomes.
The qualitative research is not intended to provide a representative overview of the population, and thus, findings should not be generalised.
2.5.2 Participant eligibility and identification
Participant recruitment was guided by a set of criteria designed to uphold the safety of participants and researchers, while also ensuring minimal disruption to participant engagement in services. This reduced the pool of eligible participants to participate in the qualitative research. For example, one criteria was that people who used violence were only eligible to participate if the affected family member was engaged by a family safety contact or specialist family violence service, in order to manage any potential risk that could arise from the interviews. This criteria greatly reduced the number of available participants. This may explain the lower number of people experiencing violence participating in the interviews compared to people who use violence.
The recruitment of participants via service providers is an important mechanism for reducing and mitigating risk. In particular, it ensures couples are not both interviewed, and that service providers can ensure the safety of the person experiencing violence. It does however, introduce the potential for a biased sample. For example, providers may only have forwarded participants who they thought would reflect positively on the service, or perhaps participants who were more engaged in the service would be more likely to volunteer for the research. This potential risk was mitigated by the approaches adopted by the Social Research Centre, including provision of a ‘recruitment pack’ to providers and regular check-ins with providers regarding the process. These mitigation strategies were approved by the Human Research Ethics Committee.
2.5.3 Data collection tool
There are limitations with the data received from providers via the data collection tool. Of the providers who submitted the data collection tool, many had substantial gaps in content. This was not unexpected, as the tool was a new instrument, and providers were implementing the mechanisms for data collection activity at an organisational level. Some of these limitations were rectified between phase one (data provided to the evaluators in July 2019) and phase two (data provided to the evaluators in September 2019). Additional training was provided, to emphasise the need to complete all fields (rather than leave blanks) and how to interpret particular fields such as referrals. Despite some improvement between phase one and phase two, there were still significant gaps in the data, and further work is needed to ensure data is consistently recorded by providers moving forward.
These gaps do, however, make the data unsuitable for drawing robust conclusions on program outcomes at this point in time, or being able to make any substantiated claims or comparisons at a cohort level. Particularly for the data collected on participant outcomes, there are significant gaps in exit data and equivalent data for people who experience violence, with which to make valid comparisons against the entry level data.
2.5.4 Time frame
It is recognised that changing behaviour can be a long and complex process, that can require multiple interventions. This evaluation collected data about people who used violence who had received one of the interventions within 12 months of the evaluation commencing. As a result, the evaluation was not able to capture any long-term or longitudinal data to determine the effectiveness of the programs over a longer timeframe.
[1] Request for Quote - Evaluation of new community-based perpetrator interventions and case management trials, Department of Health and Human Services
[2] While an important process, these additional activities meant that interviews with Aboriginal participants were delayed during the process phase of the evaluation. The additional consultation required to gain ethics approval for culturally diverse clients resulted in similar restrictions. As a result, these cohorts received one round of interviews over an extended period of time.
Justification & appropriateness
Key findings
- The Royal Commission provides evidence for the need for perpetrator interventions targeting specific cohorts. It identified that mainstream MBCPs are not easily accessible or are not relevant for a number of people who use violence. It also found that existing, group based MBCPs are, by their nature, not designed to work with participants individually, to provide a more intensive service where necessary.
- Currently, there is very limited knowledge of how to address certain cohorts in the context of perpetrator intervention programs.
- Responses to perpetrators need to address individual risk factors contributing to violent behaviours, such as past experiences of trauma, alcohol and drug misuse, and mental illness.
- The models employed by the pilot programs have been designed or adapted to address the specific needs of these cohorts.
- A specific program for people with mental health and AOD issues is not currently being provided, despite this being an identified need. Since the programs were established, FSV has been involved in capacity building activities in order to strengthen this response across the sector.
Perpetrator intervention programs are a common response for addressing the behaviours associated with family violence, and to bring perpetrators into view. These programs offer a preventative approach to behaviour change, alongside other more punitive responses such as intervention orders or criminal justice responses[1] . These programs are designed to treat the underlying beliefs, assumptions, or thought patterns that drive or facilitate the use of violence against their partner and/or children.
MBCPs have been developed and in use since the 1980s, in Australia and internationally, however service gaps still exist as they are either significantly less effective for certain cohorts, or minority cohorts are excluded from participation in MBCPs altogether. The Royal Commission found that interventions needed to respond to perpetrators and promote behaviour change vary. Some individuals require support through a behaviour change program, while others require tailored and intensive assistance [2]. This literature scan discusses the types of perpetrator intervention models that exist currently, their limitations, and how the new cohort trials and case management are designed to better treat certain cohorts of perpetrators.
3.1 The identified problem
The Royal Commission highlighted the importance of “bringing perpetrators into view and assisting them to change behaviours” for reducing family violence. The Royal Commission found that the response to perpetrators was under-developed, despite initiatives that aimed to maintain surveillance of high-risk perpetrators. Further, it cited analysis that recidivism from a small number of perpetrators account for a comparatively large share of family violence[3]. While it highlighted there were programs for perpetrators, there existed significant service gaps.
The Royal Commission heard that mainstream MBCPs are unsuitable for a number of perpetrators because they are (a) not easily accessible, e.g. there are language or cognitive barriers, or (b) they are not relevant, e.g. they do not address differences in cultural context, gender or sexuality. The Royal Commission also found that existing, group based MBCPs are, by their nature, not designed to work with participants individually, to provide a more intensive service where necessary. Additionally, a lack of understanding of family violence within these diverse communities can mean that individuals do not actively seek help, or when they do, providers are not equipped to respond effectively. Reasons for this include:
- the need to comply with minimum standards that mean course content is not suitable for certain people due to language, cultural, religious or sexuality reasons
- there is a lack of qualified staff trained in working with these cohorts of men
- there is limited capacity to provide a more intensive service where necessary.
As outlined in the Royal Commission final report, while there may be common risk factors for family violence, perpetrators are a diverse group. In addition to the barriers above, there are also specific needs and experiences relevant to different groups which impact on their ability to access and engage in mainstream MBCPs. Section 3.1.1 outlines the target populations which were identified by the Royal Commission as being typically excluded from mainstream programs, and the specific barriers they face.
3.1.1 The needs of specific cohorts
Given the limitations in the current service approach, it is important to understand the context of certain minority groups, as identified by the Royal Commission, which should inform program design.
3.1.1.1 Aboriginal and Torres Strait Islander people [4] who use violence
Aboriginal culture and identity has existed and survived for more than 60,000 years in spite of the impact of colonisation and tide of history. Within the State of Victoria, Aboriginal cultures and communities are not homogeneous but diverse entities, each with rich and varied histories and cultural heritage.
However, since colonisation, Aboriginal people have experienced violence by non-Aboriginal people, particularly during the early settlement period between the 1830s and 1900s. This violence has been both physical, structural and institutional. In addition to many documented instances of frontier violence, it includes but is not limited to dispossession of land and children, exclusionary policies, prohibition to practicing culture and language, removal from their ancestral country, relocation to missions and genocide. A greater proportion of Aboriginal people are impacted by the Stolen Generation in Victoria relative to other jurisdictions [5]. Such violence has led to the accumulation of intergenerational trauma, which impacts experiences of family violence within Aboriginal communities [6].
Family violence is defined by the Victorian Indigenous Family Violence Task Force[7] as:
an issue focused around a wide range of physical, emotional, sexual, social, spiritual, cultural, psychological and economic abuses that occur within families, intimate relationships, extended families, kinship networks and communities. It extends to one-on-one fighting, abuse of Indigenous community workers as well as self-harm, injury and suicide.
This definition of family violence is used in Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families, released in November 2018. This is an Aboriginal-led Victorian Agreement that commits signatories to work together to ensure Aboriginal people, families and communities are living free and safe from family violence. Dhelk Dja recognises that family violence is not part of Aboriginal culture or ever was before settlement occured. Family violence against Aboriginal people can be perpetrated by Aboriginal and non-Aboriginal people.
In the case of programs for Aboriginal men, there are different causes of family violence in these communities, which stem from the impact of colonisation, and the loss of culture, connection to Country and kinship relations[8]. Responses to family violence for Aboriginal people and families need to be Aboriginal-led, take a holistic approach (emotional, spiritual, and cultural wellbeing), and understand cultural and historical dynamics. It is important for non-Aboriginal organisations to involve Aboriginal organisations in service design and delivery.
The Royal Commission highlighted the lack of culturally safe, holistic and therapeutic interventions for Aboriginal and Torres Strait Islander men. VACSAL’s submission to the Royal Commission noted that nine out of 10 Aboriginal men who access mainstream behaviour change programs delivered by non-Aboriginal providers say they are not appropriate for Aboriginal men [9].
3.1.1.2 Culturally and linguistically diverse communities
Research and evidence from practice has showed that current (mainstream) programs do not adequately address the nature and causes of intimate partner violence perpetrated by men from culturally and ligusitically diverse backgrounds. In general, MBCPs are largely based on western notions of family and family life [10]. Additionally, for men lacking proficiency in the language the program is offered, understanding of the content is often limited, and therefore participation will not be meaningful. Evidence presented to the Royal Commission found that of 35 MBCPs, only two were delivered in languages other than English [11].
In addition to the language barriers, there is a lack of culturally appropriate practice within existing service models. While there are a very small number of culturally specific programs, most programs do not draw on the cultural norms and beliefs of men from CALD backgrounds. Of those that do, there are often long waitlists, and many participants have to travel long distances to attend the programs. Additionally, there are a limited number of facilitators trained to work with people who use violence from culturally diverse backgrounds [12].
3.1.1.3 Lesbian, gay, bisexual, transgender and intersex people
Mainstream perpetrator interventions models, such as Duluth or Cognitive Behavioural Therapy (CBT) approaches typically do not consider the specific needs or unique circumstances of LGBTI couples [13]. Research suggests LGBTI people experience unique stressors that accompanies being part of a sexual minority population [14]. These can be internal stressors, such as internalised homophobia, or external, such as actual experiences of violence, discrimination and isolation.
The focus of mainstream MBCPs has typically been focused on responding to male violence against women. This reflects the gendered and binary nature of family violence, but excludes affected LGBTI people. No to Violence conducted a study in 2015 which showed that male same sex intimate partner violence is significantly under-reported, and there are cases where generalist services may minimise violence between two people of the same gender[15]. The Royal Commission also found that there are circumstances where it can be unsafe for LGBTI people to attend these programs, as other members of the group may be homophobic or transphobic/biphobic and they exclude women.
3.1.1.4 Women who use force
Examination of literature regarding MBCPs shows that the overwhelming focus of these programs is on men, as the name suggests, as men account for the significant proportion of people who use violence. However, there are a cohort of women who use force in intimate relationships, often as a form of resistance against other adult family members. Although there are women who are predominant aggressors in domestic violence situations, researchers agree that most women who use force in their intimate relationships are victims who self-defended or retaliated [16]. At the time of the Royal Commission, there were limited suitable services in Victoria to provide an intervention for this group of women to address their violent behaviour.
3.1.1.5 People in rural, regional and remote communities
The Royal Commission heard that there are limited perpetrator intervention programs for people in rural, regional, or remote areas. Where these programs do exist, there are lengthy waitlists, and sometimes people access non-specialised counsellors as an alternative.
3.1.1.6 People with disabilities who use violence
People with disabilities, such as intellectual disabilities or acquired brain injuries, often struggle to comprehend course content, have limited capacity to engage in a group context, or are screened out of mainstream MBCPs altogether.
There is very limited practice guidance to support engagement with people with a cognitive impairment in MBCPs or other perpetrator interventions. A report undertaken by the Commonwealth Department of Social Services to scope innovative perpetrator intervention practices in Australia found that there is very little available for this cohort. The report states:
FDV [Family and Domestic Violence] perpetrators with cognitive impairments – mild intellectual disability, moderate intellectual disability, ABI and foetal alcohol syndrome – appear to be poorly served by existing interventions. It is reasonable to expect they would have specific needs; but no jurisdiction seems to have policy or documented pathways to indicate where and how interventions might take place [17] .
3.1.1.7 Older people who use violence
Whilst there are no barriers to the referrals or access of older men in mainstream MBCPs, they may have difficulty engaging with the content due to health issues, e.g. dementia, and other behavioural or cognitive issues.
The dynamics of elder abuse may also differ from other instances of family violence, due to the presence of both gendered and ageist attitudes. This may require alternative approaches to changing attitudes and behaviours.
3.1.1.8 People with complex needs, including mental health and AOD issues
In their submission to the Royal Commission, the Centre for Forensic Behavioural Science at Swinburne University included the following statement[18]:
“Intervention programs need to be responsive to the complex needs of the wide variety of family violence offenders. In particular, we must improve provision of specialist interventions to those with complex and serious mental, personality, and substance use disorders. There is a clear need for better integration and communication between mental health services, drug and alcohol services, and offence-specific program providers”.
The most common risk factors put to the Royal Commission which described people who use violence with complex needs were mental illness and AOD abuse. The Royal Commission heard that the mental health and AOD sectors remain disconnected from family violence services, and people with these conditions are less likely to engage with services or follow up on referrals. Additionally, when someone has a mental illness or AOD issues, they are unlikely to be able to engage in other services until these problems are addressed[19]. The Royal Commission also heard that there is a lack of capacity among current program facilitators to adequately identify and address mental health and AOD issues, which includes a lack of resources across the sector to provide individualised, tailored responses [20].
3.1.2 The proposed response
The Royal Commission recommended that perpetrator interventions targeted at these specific cohorts be established, as an alternative to mainstream MBCPs. The generalist response has been described as inflexible and outdated, and not keeping pace with best practice [21].
Programs offering cohort specific, culturally sensitive approaoches were suggested, as generalist programs may be perceived as alienating or irrelevent to the circumstances of specific cultural groups [22]. Additionally, responses to perpetrators needed to address individual risk factors contributing to violent behaviours, such as past experiences of trauma, alcohol and drug misuse, and mental illness.
Recommendation 87 of the Royal Commission stated:
The Victorian Government, subject to advice from the recommended expert advisory committee and relevant ANROWS (Australia’s National Organisation for Women’s Safety) research, trial and evaluate interventions for perpetrators that:
- provide individual case management where required
- deliver programs to perpetrators from diverse communities and to those with complex needs
- focus on helping perpetrators understand the effects of violence on their children and to become better fathers
- adopt practice models that build coordinated interventions, including cross-sector workforce development between the men’s behaviour change, mental health, drug and alcohol and forensic sectors.
3.2 Existing frameworks for perpetrator intervention
Most men’s behaviour change programs share common theoretical frameworks which underpin the treatment approaches. The most dominant theoretical model is known as the Duluth model, followed by cognitive behavioural therapy. These approaches are designed to address the underlying issues and causes of violent behaviour. However, it should be noted that few MBCPs only apply a single theoretical model to their approach. Most program providers blend two or more models within their program design.
3.2.1 The Duluth model
The Duluth model uses a feminist analysis of partner violence. Designed to educate and raise awareness, under this model intimate partner violence is treated as a response to the patriarchal nature of social arrangements [23]. Treatment of the perpetrator is based on coordinated strategies grounded in the experience of the victim, as opposed to the program being based solely on a criminal justice response.
The Duluth model incorporates the following approaches:
- highlighting perpetrator accountability by taking the blame off the victim
- prioritising the victim ‘voice’ and experiences in the creation of policies
- actively working to change societal conditions that support men’s use of control over women
- incorporating behaviour-change opportunities within court-ordered mechanisms
- collaborating across criminal, civil and community agencies to improve the community’s response to family violence [24]
Central to this approach is the Power and Control Wheel, which emphasises that abuse and violence is linked to male power and control, and the accompanying aspects, or ‘spokes’ of this wheel [25] include:
- minimising
- denying
- blaming
- using intimidation
- emotional abuse
- isolation
- children
- male privilege
- economic abuse
- threats.
This framework recognises that males use other means, in addition to physical acts of violence, to maintain control. Different methods are applied within the model to explore how men use controlling behaviour in relation to different themes. That men tend to view themselves as the victim, and that violence is used to regain power, status or respect (often from other areas of their lives), is also highlighted.
Another related model commonly used in Australia is the Risks Needs and Responsivity (RNR) model. This model takes a more individualised approach. Factors such as individual criminal history, learning style, and actuarial risk and instability factors are considered in addition to the socio-political factors emphasised in the Duluth model [26].
The Duluth model’s success has been attributed to inter-agency cooperation, and the fact that the model is developed from women’s own experiences of violence (incorporated within the spokes of the power and control wheel).
There has been some criticism directed at the Duluth model for being a “one-size-fits-all” approach, as it focuses on structural factors - gender based power relations - as the primary cause of domestic violence[27]. Dutton and Corvo [28] denounce the model as an ideologically narrow model of intervention, calling it a “radical form of feminism”. They also criticise the Duluth model for not being therapeutic, shaming clients, and showing no effective outcomes, and call for more attention to women’s violence. Gondolf [29] rejects this perspective, claiming that this narrative is misleading and can damage important progress in the field of perpetrator intervention. Gondolf highlights a multi-site, longitudinal evaluation of a Duluth-based ‘batterer intervention’, which demonstrated a clear de-escalation of abuse overtime, with 80 per cent of the men not being violent towards their partners in the previous year, at 30 months from program intake. The results also demonstrated positive impressions of change from the women’s perspective. This evaluation considered the ‘holistic’ intervention – from the arrest, court mandated referrals, supervision, and the program itself – which demonstrated that the criminal justice intervention, combined with the behaviour-change program, is not detrimental to a majority of men.
3.2.2 Cognitive behavioural therapy (CBT)
CBT, the most common psychotherapeutic approach, is another major approach to treating perpetrators. CBT is based on the identification and correction of mental processes that grant offenders the permission to commit violence, generally in a cyclical process. Men who perpetrate violence often consider themselves victims, blaming their partner for their own violence. The goal of CBT is to interrupt this process, helping the man to identify the preceding physical signs, thoughts and feelings by which he grants himself permission to commit violence [30].
There may also be certain beliefs or thought patterns about their partner, or women in general, at the core of their behaviour that CBT explores. Vignettes, role playing, discussions, practising alternative behaviour, and teaching and rehearsing new skills are all used in the delivery of programs that incorporate CBT[31].
CBT is more of an additional as opposed to a stand-alone approach, given that the ability to apply these skills in the particular context (their relationships) is needed. The combination of feminist analysis with CBT is often used; with 68% of states in the USA taking this approach, while only 5% of states use CBT but do not incorporate power and control [32].
3.2.3 The transtheoretical model (TTM) and the stages of change
The TTM is based on the concept that people go through stages of change before they are able to successfully achieve and maintain behaviour. These sequences of change move from precontemplation to contemplation, preparation, action, and maintenance. Within this model, it is not uncommon for individuals to move forward and backwards across the stages as they undergo treatment, rather than change occurring within a linear fashion. The TTM helps to explain the lack of progress made by men in the early stages of participation in MBCPs, as they are in the precontemplation stage and may be unwilling to acknowledge their use of violence within intimate relationships.
A number of studies have demonstrated the value of applying a TTM framework to treatment of violence in intimate relationships [33]. Results show that an intervention will be more effective in changing behaviour when a man’s treatment readiness is high. When a person is at the early stages of change, they tend to downplay their behaviour and report less signs of anger, which is consistent with denial and minimisation, rather than acceptance of violent actions [34]. A study by Levesque, Gelles and Velicer[35] found that there were varying stages of readiness within a sample of 292 men participating in a domestic violence counselling group. Twenty-four per cent of men were in the precontemplative stage, 63% in the contemplative/preparation stage, and only 13% in the action stage. These results explained why there can be varying levels of engagement and progress shown by men within the same treatment group.
Motivational interviewing (MI) is a counselling strategy aligned to the TTM model, which assists clients to increase their readiness for change. During MI, clients are assisted to identify their stage within the TTM framework, and then work through how this will influence their behaviour change process. The key features of MI counselling include use of empathy, avoidance of argumentation, and support for self-efficacy. Results assessing the impacts of this approach show that men in the later stages of change were able to recognise that there were aspects of their lives that required the need for treatment, however those in the earlier stages of change were not consistently recognising that they needed to make changes to aspects of their lives [36]. Additionally, this was also an indicator of readiness for group therapy as opposed to individual treatment. This is a useful finding for understanding that individuals who are more accountable for their actions are more likely to engage in, and benefit from, the treatment process. It is therefore important to determine the stage of change prior to commencing treatment, in order to understand the potential causes, and variances, in individuals’ behaviour change.
3.2.4 Other models
Noting that the approach to perpetrator interventions can vary widely, there are a number of other models used around the world, which often draw on or, in some cases, underpin the frameworks listed above [37]. These include:
- Psychoeducational – This approach is based on the underlying theory that socio-political factors (entrenched gender inequality, patriarchal ideology) are the cause of family violence. The use of violence is viewed as deliberate and intentional, for the purpose of controlling and dominating women. These programs are typically well structured, however have been criticised for lacking empirical support, being ineffective at promoting self-engaged change, and being a one-size-fits-all approach that doesn’t theoretically account for violence in other situations (such as violence by women against men or those in same-sex relationships). The Duluth model falls within this category
- Psychotherapeutic - Viewing family violence as caused by personal dysfunction, these approaches stem from psychiatry and psychology, and use individualised programs. CBT is considered by some (but not all) to be a psychotherapeutic approach. Cognitive therapy, not to be confused with CBT, has a behavioural component and yet is different due to the relationship that develops between the therapist and the person who uses violence
- Family therapy and couples counselling - These interventions are used for particular types of perpetrators when typical group settings are considered inappropriate. While informed from different theoretical perspectives, these programs approach the issue of family violence as the result of a dysfunctional relationship. Given a majority of victims either stay with or return to the perpetrator, advocates of this approach argue this should be offered in order for the couple to work through their issues [38]. However, others argue that it places the victim in danger, and that it implies both parties are responsible for the violence.
Most approaches use some combination of psychoeducational and psychotherapeutic approaches. Many largely psychoeducational programs incorporate stress management, behaviour change and communication skill development. Further, as mentioned above, CBT is more typically used in conjunction with a gender-based power and control framework similar to the Duluth model.
- Matched interventions – Based on family violence having a number of causes, matched interventions are tailored to the perpetrator’s level of risk, criminogenic needs, and readiness to change. The intervention may be based on where the perpetrator falls according to a specific typology. For instance, family therapy is advocated by some as appropriate for couples with low-level, “situational violence”. The TTM of Change (discussed above) and motivational interviewing (MI) are two examples. While it has grown in popularity in Australia, evidence on the effectiveness of MI is inconclusive, as is its impact on retention rates.
3.3 Common treatment approaches
Keeping in mind the Duluth model (or a similar feminist analysis models) is dominant, research on MBCP approaches, while not always model specific, highlight the following common features of program delivery:
- Group sessions, one-on-one sessions, and a mix of both are used. One program identified (the New York Model for Batter Programs) only accepted court-mandated offenders, while most did not indicate this aspect of eligibility[39]
- Based on all the programs and jurisdictional standards reviewed, program length ranges from 6-40 sessions over 10-48 weeks [40]. However, programs of less than 20 weeks are often considered too short, as they do not take into account the time taken for participants to develop motivation for behaviour change
- While few details regarding intake and eligibility were identified, one program identified in the primary search had developed material specific for a particular cohort of offenders (Relationships Australia Victoria’s CALD MBCP)[41]
- A majority of states in the USA require an intake evaluation or assessment, in part to determine if other services (like AOD treatment) are also necessary. A review of police reports or other available court documents is also undertaken. Additionally, a review of previous contacts with health providers is also required by many states
- A large majority of programs (93% in the USA) include contact with the people experiencing violence [42]. This could include support, advocacy, counselling or appropriate referrals. For those that didn’t engage with victims, it is typically due to concerns for their safety[43].
In general, the highest risk (10-20%) offenders are not considered suitable for perpetrator intervention programs [44]. The most severe cases include individuals with high levels of psychopathy and a history of violence in other (than family violence) contexts. Issues that interfere with their ability to function in a group environment, such as substance abuse or mental health issues, may make an individual unsuitable until such issues are stabilised. In general, the content of these programs is the same whether you are a first time or repeat offender [45].
3.3.1 Measuring the success of MBCPs
There is limited evidence from the literature on perpetrator intervention program success factors and quality. Proving a clear evidence base for domestic violence perpetrator interventions has been “extremely difficult”, as noted by the ANROWs literature review [46].
A recent ANROWS review[47] identified that:
- formally articulating program logic models is beneficial (as they can guide evaluation), and MBCPs should be supported to do so
- strengthening safety and accountability planning can improve program quality
- engaging with victim survivors can improve program quality, and that this is currently an underfunded aspect of these programs.
Motivation is considered to be an important factor in program success. As mentioned above, program length is considered an important aspect of effectiveness, with 20 weeks being the minimum. Some men may take the first 12-15 weeks of a program to become motivated and ready to put in the work to change[48]. There are a number of other factors/predictors considered important, including having fewer contacts with the criminal justice system, and the absence of comorbid conditions (such as AOD or mental health).
A 2016 study[49] by researchers at Monash University considered program outcomes following MBCP participation over two years, for 300 participants across three states. The study found immediate and sustained falls in violent behaviour after program completion, with 65% of these men either violence free or almost violence free two years later. However, the study also noted a list of shortcomings of MBCPs, most of which fall under two categories:
- Inadequate service: Poor coordination between agencies, often no end-of-program assessment with referral to relevant supporting services, and limited length of program time.
- Too difficult to access: Long waiting times, and program unavailability in many areas.
Authors of a study by RMIT’s Centre for Innovative Justice (CIJ) [50], believe that while interventions in general act as ‘doorways to treatment’, they also pose risks. Some key risks that must be accounted for when referring people to MBCPs include whether a perpetrator may think a partner ‘dobbed him in’, and the agency’s ability to identify risks and collaborate with other agencies to address them.
Based on the existing evidence base, there is variable evidence that behaviour change programs have an impact on recidivism. One 2013 review of 30 studies found that about half of the interventions were more effective than a no-treatment control group [51]. The conclusion was more pessimistic if excluding studies with methodological flaws. Quantified outcome results for targeted cohort interventions (such as AOD, mental health, or CALD) were not identified. There is little evidence to support one type of intervention being more effective than another [52].
However, as noted by Project Mirabel in the UK [53], most existing literature on perpetrator programs is based on programs in the USA. Most men in these studies were court mandated, and not many of the programs offered support for victim/survivors. This makes translating these results for the Australian context difficult.
3.4 Treatment approaches for diverse cohorts – current evidence, and gaps in knowledge
It has already been mentioned that there is limited knowledge of how to address certain cohorts with complex needs in the context of perpetrator intervention programs. In many cases, these individuals are considered ineligible for perpetrator interventions, as their specific issues impact on their ability to be treated in a group environment. The Victorian MBCP minimum standards focus on how these factors impact on eligibility for the program while providing limited guidance on how to accommodate these cohorts[54]. As noted by the Royal Commission, for perpetrators ineligible to participate in perpetrator programs due to the complexity of their needs, “there is little else available to specifically address their family violence offending” [55].
The following sections outline evidence of current practices for tailoring support to the needs of specific populations when addressing family violence. Despite this, the current literature is very limited, and for some groups non-existent.
3.4.1 Aboriginal and Torres Strait Islander people who use violence
Programs for Aboriginal and Torres Strait Islander people should be developed with a strong cultural foundation [56]. This includes designing them in a way that acknowledges the causes (e.g. impact of colonisation, stolen generation, substance abuse, entrenched poverty, experiences of trauma) and experiences of family violence in Aboriginal communities, which are more about compensation for a lack of value and esteem rather than patriarchal power [57].
Studies have noted the importance of healing approaches, which includes a holistic model encompassing the social, emotional, spiritual and cultural wellbeing of participants [58]. The concept of a ‘perpetrator’ is not commonly understood when working with Aboriginal and Torres Strait Islander people who use violence, and therefore terminology should be focused on values and concepts that relate to the men’s circumstances, and the impact on the victim.
Additionally, it is vital that programs are developed and delivered with involvement from the local community. This will ensure that programs are designed to meet specific needs, with the local context in mind. For example, programs may be run at a local sporting club or on country, and include local Elders in the delivery of the program [59].
3.4.2 Culturally and linguistically diverse communities
To address the notion that the content of mainstream perpetrator programs are largely focussed on western concepts of family life, and often do not consider people who are not proficient in English, there has been an increasing emphasis on designing programs which are culturally specific. Typically, these programs are delivered in a group setting by a facilitator of the same cultural group, and the curriculum integrates cultural issues [60]. This format also provides social support to the men in addition to the focus on behviour change.
Programs specifically targeted at migrant or refugee men must recognise the experiences of trauma experienced by these men, and other risk factors contributing to their violent behaviour such as experiences of racism, social isolation, stress caused by immigration, and lack of access to other supports.
However it has been argued by some researchers that categorisation of people according to broad social groups may be ’reductionist’, by defining their identity in simplistic terms, and not recognising subtle cultural differences within larger population groups [61]. It is therefore important that people from specific cultural backgrounds should be given the option of both culturally specific or mainstream programs.
3.4.3 People with a disability
Intervention with this cohort requires sensitivity to the lack of able-bodied privilege that these perpetrators experience in many aspects of their lives. This includes experiences of marginalisation, lack of access to resources and opportunities, and disabling environments. Whilst these experiences do not excuse perpetration of violence, it is important to recognise how these individuals can be both perpetrators (of gender-based violence) and victims (of ableism) at the same time [62].
It is noted that for people with an intellectual disability or an acquired brain injury, there is less of a need to change the framework or the context via which family violence should be understood, but more about altering the mechanisms through which information is delivered. This may include adjustments such as the use of easy English materials, or taking more time to focus on specific aspects of course content [63].
3.4.4 LGBTI people who use violence
Due to the very few services for this cohort which exist in Australia, there is limited evidence regarding best practice approaches for people who use violence in LGBTI relationships. However a study conducted on intimate partner violence among sexual minority populations in the United States shows that there are a number of practice and policy implications for addressing the use of violence among this cohort [64]. This includes:
- removing other barriers leading to stress and a reduction in help-seeking, such as provision of housing or legal support
- understand the dual nature of victimisation and perpetration of violence commonly experienced by this cohort
- recognising the common negative social reactions that are often received by this cohort when accessing support
- use inclusive language, which does not address family violence as a heterosexual-only issue
- be aware of the issues faced by LGBTI people, without affiming stereotypes or stigmatising this population.
3.4.5 Women who use force
It is important to note that domestic abuse is gendered, and in its most dangerous form – coercive control – it is almost exclusively a crime perpetrated by men against women [65]. Women who use force in intimate relationships are almost always doing so in self-defence – a form of violence which has been labelled ’violent resistance’ [66]. A starc reminder of this fact is that when women kill their intimate partners, they are almost always killing a perpetrator. This was shown in a study undertaken by the NSW Domestic Violence Death Review, which found that 28 of 29 men killed by a female partner were violent perpetrators themselves [67]. Noting this context, the Royal Commission acknowledges that interventions for women who use force need to consider the environment in which the woman is using violence in an intimate relationship, and ’untangle’ the situations where this is in self-defence to her partner’s violence, where he is the primary agressor. It also noted the higher correlation between violence and other risk factors for this cohort, such as AOD and mental health issues, post-traumatic stress disorders, personality disorders, and a history of abuse[68].
The Royal Commission established four principles for developing programs for women who use violence, based on evidence from the United States:
- mainstream perpetrator programs are not sutiable for women who use violence, as these programs address coercive control which is not used by a majority of women
- interventions for women who use violence should address circumstances including persistent victimisation, self-defence and motivation for retaliation
- programs should consider the consequences that may result from refaining from violence, such as injury, feelings of being dominated, and the reactions of others
- interventions should acknowledge the unique and complex circumstances of individuals in this cohort [69].
3.4.6 People with complex needs
Given the prevalence of mental health and AOD issues among people who use violence, addressing these issues is an important part of the behaviour change process. Submissions to the Royal Commission highlighted the importance of an integrated response model whereby mental health and AOD services collaborate with family violence services to offer a joined-up response. Evidence was cited from combined AOD and MBCPs in the United States, whereby and integrative approach that targeted both addiction and aggressive behaviours had postive treatment outcomes for reducing both of these behaviours, compared with only targeting substance issues [70].
This focus on jointly addressing substance abuse and family violence in the one intervention was also demonstrated to be effective in a three year pilot program delivered by Communicare in Western Australia. In this model, men attending a MBCP were also allocated to an AOD case worker. They found that it was more effective to train MBCP facilitators in addiction work, rather than train AOD workers to address family violence, due to the nature of working with the men to address accountability and responsibility.
3.4.7 Rationale
Noting the limited, and often inconclusive nature of the current evidence on appropriate approaches for specific cohorts, it is intended that new Victorian programs will assist in building the evidence base for what works to acheive behaviour change for these population groups. Section 3.5 outlines the models that have been adopted in each of the new programs, in order to address the current gaps.
3.5 The Victorian response
3.5.1 Overview
Noting the current evidence presented in the section above, the models employed by the pilot programs have been designed or adapted to address the specific needs of these different cohorts, often drawing on approaches used overseas as they address gaps in the mainstream service delivery models typically used in Australia. As indicated Section 3.4, this often includes approaches such as trauma-informed practices, integrated response models, and cultural healing.
Table 3.1, below, outlines the specific models and approaches adopted by the new community-based interventions and case management trials, in order to address the identified gaps [71].
Table 3‑1 Program design features
|
Cohort |
Design features |
|
Women who use force (Baptcare/Berry St trial) |
|
|
People who use violence with cognitive impairment and/or learning disabilities (Bethany and Peninsula Health trials) |
|
|
LGBTI people who use violence (Drummond St trial and Thorne Harbour Health case management) |
|
|
Specific CALD cohorts (InTouch trial) |
|
|
Aboriginal and Torres Strait Islander people who use violence (Anglicare/VACCA, BDAC, and Baptcare/Berry St trials, and targeted case management providers) |
|
|
Fathers (Anglicare/VACCA trial) |
|
|
Case management |
|
3.5.2 Mental health and AOD
Perpetrators with complex needs including drug and alcohol and mental health issues were specifically identified in the request for funding submissions. Despite receiving over 50 submissions in total, FSV could not recommend a provider focusing on mental health and AOD cohorts for funding, as they did not meet the criteria. Specifically, FSV identified that many mental health and AOD organisations (community and clinical) were large-scale and had established frameworks for working and existing programs that they were unable to sufficiently adapt to the family violence context. For example, they did not fully understand the role of the Family safety contact.
Despite there being no cohort providers specifically targeting people who experience mental health and substance abuse issues, there is a clear need for this. One hundred and four of 202 of case management participants and 63 of 117 cohort trial participants are reported as having a mental illness or AOD issues in the data collection tool [72]. Acknowledging this, since the pilot programs were established, FSV has been involved in broader capacity building across the sector to better respond to people who use violence and people who experience violence who have AOD and mental health issues. This has included embedding 44 specialist family violence advisers in the AOD and mental health DHHS regions. These positions provide advice for both people who experience violence and people who use violence.
[1] Vlias, R., Ridley, S., Green, D. and Ching, D. (2017). Family and domestic violence perpetrator programs – Issues paper of current and emerging trends, developments and expectations. Stopping Family Violence Inc.
[2] State of Victoria (2016), Royal Commission into Family Violence: Summary and recommendations.
[3] State of Victoria (2016), Royal Commission into Family Violence: Summary and recommendations.
[4] As per the Aboriginal Heritage Act 2006, “an Aboriginal person belonging to the indigenous peoples of Australia.” In this report, the term Aboriginal is used interchangeably with Indigenous.
[5] Department of Health and Human Services (2018), Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families, Available at: https://www.vic.gov.au/family-violence-support
[6] ibid
[7] Department for Victorian Communities (2003). Victorian Indigenous Family Violence Task Force Final Report.
[8] Bartels, L. (2010 ). Emerging issues in domestic/family violence research (Research in practice no. 10) . Canberra: Australian Institute of Criminology.
[9] State of Victoria (2016), Royal Commission into Family Violence: Summary and recommendations.
[10] Crichton-Hill, Y. (2001). Challenging ethnocentric explanations of domestic violence. Trauma, Violence & Abuse, 2(3), 203–214.
[11] State of Victoria (2016), Royal Commission into Family Violence: Summary and recommendations.
[12] State of Victoria (2016), Royal Commission into Family Violence: Summary and recommendations.
[13] Rolle, L., Giardina, G., Caldarera, A.m., Gerino, E and Brustia, P. (2018). When Intimate Partner Violence Meets Same Sex Couples: A Review of Same Sex Intimate Partner Violence. Frontiers in Psychology, Available at: https://www.frontiersin.org/articles/10.3389/fpsyg.2018.01506/full
[14] Carvalho, A. F., Derlega, V. J., Lewis, R. J., Viggiano, C., and Winstead, B. A. (2011). Internalized sexual minority stressors and same sex intimate partner violence. J. Fam. Violence 26, 501–509.
[15] Lloyd, K (2015). Homophobia, Transphobia and Men’s Behaviour Change Work. No To Violence Male
Family Violence Prevention Association, 14–15.
[16] Miller, S and Meloy, M. (2006) Women’s use of force, Violence Against Women, Vol. 12, No.1, pp 89-115
[17] Vlais, R. (2017). Scoping study of innovations in family and domestic violence perpetrator interventions. Family Safety Branch, Commonwealth Department of Social Services.
[18] Centre for Forensic Behavioural Science—Swinburne University; Victorian Institute of Forensic Mental Health (Forensicare), Submission 649.
[19] State of Victoria (2016), Royal Commission into Family Violence: Summary and recommendations.
[20] State of Victoria (2015) Transcript of Ogloff and Transcript of Vlais
[21] State of Victoria (2016), Royal Commission into Family Violence.
[22] State of Victoria (2016), Royal Commission into Family Violence.
[23] Eckhardt, C, Murphy, C, Whitaker, D, Sprunger, J, Dykstra, R and Woodard, K (2013). The Effectiveness of Intervention Programs for Perpetrators and Victims of Intimate Partner Violence. Partner Abuse, The partner abuse state of knowledge project part 5, 4 (2). Springer Publishing: 196–231.; Urbis (2013). Literature Review on Domestic Violence Perpetrators; NSW Attorney General & Justice (2012). Towards Safe Families: A Practice Guide for Men’s Domestic Violence Behaviour Change Programs.
[24] Farrelly, J. (2016). ‘What is the Duluth Model for tackling domestic violence?’
[25] DAIP. 2019. “What Is the Duluth Model?” Available from: https://www.theduluthmodel.org.
[26] No To Violence (2018). Position Statement: Online programs for men who use family violence. Available at: https://ntv.org.au/advocacy-media/resources/
[27] Urbis (2013). Literature Review on Domestic Violence Perpetrators. Available at: https://www.dss.gov.au/sites/default/files/documents/09_2013/literature….
[28] Gondolf, E.W. (2007) Theoretical and research support for the Duluth Model: A reply to Dutton and Corvo .
[29] ibid
[30] NSW Attorney General & Justice. 2012. Towards Safe Families: A Practice Guide for Men’s Domestic Violence Behaviour Change Programs .
[31] Ibid.
[32] Maiuro, Roland D, and Jane A Eberle. 2008. State Standards for Domestic Violence Perpetrator Treatment: 23 (2); Urbis. 2013. Literature Review on Domestic Violence Perpetrators, Available at:https://www.dss.gov.au/sites/default/files/documents/09_2013/literature….
[33] Scott, K and Wolfe, D (2003). Readiness to change as a predictor of outcome in batterer treatment. J Consulting and Clin Psyc. 71 (5); Williamson, P., Day, A., Howells, K., Bubner, S., & Jauncey, S. (2003). Assessing offender readiness to change problems with anger. Psychology, Crime and Law,
9(4), 295-307.
[34] Zalmanowitz, S., Babins-Wagner, R., Rodger, S., Corbett, B. and Lescheild, A. (2013). The Association of Readiness to Change and Motivational Interviewing with treatment outcomes in males involved in domestic violence group therapy, Journal if Interpersonal Violence 28(5) 956-974.
[35] Levesque, D. A., Gelles, R. J., & Velicer, W. F. (2000). Development and validation of a stages of change measure for men in batterer treatment. Cognitive Therapy and Research, 24, 175-199.
[36] Zalmanowitz, S., Babins-Wagner, R., Rodger, S., Corbett, B. and Lescheild, A. (2013). The Association of Readiness to Change and Motivational Interviewing with treatment outcomes in males involved in domestic violence group therapy, Journal if Interpersonal Violence 28(5) 956-974.
[37] Mackay, E., Gibson, A., Huette, L. and Beecham, D. (2015). Perpetrator interventions in Australia: State of knowledge paper, ANROWS.
[38] Stith, S. M., McCollum, E. E., Rosen, K. H., & Thomsen, C. J. (2004). Treating marital violence within intact couple relationships: Outcomes of multi-couple versus individual couple therapy. Journal of Marital and Family Therapy, 30(3), 30-18.
[39] New York Model for Batterer Programs (2015). NY Model. Available at https://www.nymbp.org/
[40] The following is a list of showing how program length varies across jurisdictions:
- NSW standards: recommend a 20-48 week (international standard program length) as 12 weeks is inadequate.
- QLD standards: 32-40 hours duration over 13-16 weeks
- VIC: 12-20 group work sessions followed by one or two sessions of individual assessment
- WA: most include about 26 sessions of group work and also offer additional individual sessions
- USA: Survey of 276 batterer intervention programs in the USA found the average length was 26 sessions.
[41] Relationships Australia Victoria (2013). Effective Men’s Behaviour Change Programs for Culturally and Linguistically Diverse Men. Available at: http://www.familyviolencehumeregion.com.au/wp-content/uploads/2013/04/R….
[42] Maiuro, R, and Eberle, J (2008). State Standards for Domestic Violence Perpetrator Treatment . 23 (2): 133–55. doi:10.1891/0886-6708.23.2.133.
[43] Vlais, R (2014). Ten Challenges and Opportunities for Domestic Violence Perpetrator Program Work. Available at: https://ntv.org.au/advocacy-media/resources/
[44] No to Violence (n.d.) Submission to the Family Law Council.
[45] Of US programs, only 3 (of 50) states have a different treatment plan if a repeat offender.
[46] ANROWS (2019). Men’s behaviour change programs: Measuring outcomes and improving program quality: Key findings and future directions (Research to policy and practice, 01/2019). Sydney, NSW: ANROWS.
[47] ibid
[48] Vlais, R (2014). Ten Challenges and Opportunities for Domestic Violence Perpetrator Program Work. Available at: https://ntv.org.au/advocacy-media/resources/
[49] Brown et al, (2016). A study of the impact on men and their partners in the short term and in the long term of attending behaviour change programs . Department of Social work, Monash University, Pg. i.
[50] RMIT Centre for Innovative Justice (2016). Pathways towards accountability: mapping the journey of perpetrators of family violence- Phase 1 , Pg. 3.
[51] Eckhardt, C, Murphy, C, Whitaker, D, Sprunger, J, Dykstra, R and Woodard, K (2013). The Effectiveness of Intervention Programs for Perpetrators and Victims of Intimate Partner Violence. Partner Abuse, The partner abuse state of knowledge project part 5, 4 (2). Springer Publishing: 196–231.
[52] ibid
[53] Kelly, L and Westmarland, N (2015). Domestic Violence Perpetrator Programmes: Steps towards change. Project Mirabal Final Report. London and Durhm: London Metropolitan University and Durham
University.
[54] No to Violence. 2017. Men’s Behaviour Change Group Work: Minimum Standards and Quality Practice. https://providers.dffh.vic.gov.au/mens-behaviour-change-program
[55] State of Victoria (2016), Royal Commission into Family Violence.
[56] Mackay, E., Gibson, A., Huette, L. and Beecham, D. (2015). Perpetrator interventions in Australia: State of knowledge paper, ANROWS.
[57] Queensland Parliament (2014). Legal Affairs & Community Safety Committee
[58] Mackay, E., Gibson, A., Huette, L. and Beecham, D. (2015). Perpetrator interventions in Australia: State of knowledge paper, ANROWS.
[59] ibid
[60] ibid
[61] Debbonaire, T. (2015). Responding to diverse ethnic communities in domestic violence perpetrator programs. Berlin, Germany: Work with Perpetrators European Network.
[62] Bethany Community Support Inc. Submission to DHHS Call for Funding Submission, 2018.
[63] State of Victoria (2016), Royal Commission into Family Violence.
[64] Edwards, K., Neal, A. and Sylaska, K. (2015). Intimate Partner Violence Among Sexual Minority Populations: A Critical Review of the Literature and Agenda for Future Research, Psychology of Violence, 5:2.
[65] Hill, J (2019). See what you made me do, Black Inc Books.
[66] Johnson, M.P. (2008). A Typology of Domestic Violence: Intimate terrorism, violent resistance, and situational couple violence. Boston: Northeastern University Press.
[67] Hill, J (2019). See what you made me do, Black Inc Books.
[68] State of Victoria (2016), Royal Commission into Family Violence: Summary and recommendations.
[69] State of Victoria (2016), Royal Commission into Family Violence: Summary and recommendations.
[70] Submission to the Royal Commission into Family violence from Dr Caroline Easton, Professor of Forensic Psychology, College of Health Sciences and Technology, Rochester Institute of Technology
[71] Based on ‘Overview of proposed approach’ in provider responses to the request for funding submissions
[72] Deloitte Access Economics data collection tool.
Lessons from practice
Key findings
- Service providers found that once trusting relationships are formed between the participants and their facilitator and/or fellow group members, a deeper level of engagement is reached.
- When one-on-one support is offered in parallel to group programs it provides additional educational support to participants who are struggling to grasp concepts covered in the group sessions, and prepares individuals for group work by addressing higher level needs.
- For many of the cohorts included in the new programs, an element of ‘healing’ in the behaviour change process is often required in order to achieve lasting change in the use of violence. This needs to be delivered within a framework of acknowledging responsibility for the use of violence.
- An aspect of most of the programs was to facilitate holistic wrap-around service provision for the people who use violence. Addressing these needs enables the person to then better engage in addressing their violent behaviours.
- When delivering cohort trials, providers have demonstrated flexibility in approaches, taking into account individual need. This included flexibility of session content, timing, delivery methods, and intensity.
- Providing support to people who experience violence via a Family safety contact provided a tailored service to these people, and increased visibility of risk factors. There were some challenges in resourcing this role.
- Some challenges were identified, including the impact on the resources available to deliver this more intensive level of support, and barriers to engaging with people who experience violence.
- Large amounts of the brokerage funding in the first twelve months went unspent, with only 14% of the total allocated brokerage acquitted, as of October 2019. There were reported difficulties in making decisions about how to spend brokerage appropriately, given a hesitance to provide financial assistance to people who use violence.
4.1 Introduction
The evidence suggests that tailoring perpetrator interventions to cater for a diverse range of individual needs, enables a greater variety of people who use violence to access and benefit from these programs. There are specific approaches that better enable previously excluded or under-serviced groups to benefit from government funded perpetrator intervention, as outlined in the previous chapter. The evaluation has determined effective approaches to delivering interventions to people who use violence, through these six key features that have been observed in the current practices of the providers delivering the new cohort trials and case management:
- trusting relationships between participants and facilitators, and among group members to encourage engagement and participation
- utilising both individual and group work [1] in a complementary manner
- balancing responsibility for violence with a trauma informed approach to address the underlying factors contributing to violent behaviour
- facilitating a holistic, wrap-around approach to address contextual factors in a person’s life by connecting them to the broader service system
- allowing flexibility in approach for people with different levels of need and at varying stages of change
- providing support to people who experience violence via the family safety contact function.
The evidence to inform these lessons are based on findings from cohort-specific group trials and case management for people who use violence with complex needs. However, a small number of examples were provided in consultations of strategies used in these trials being applied to mainstream practice. This occurred as providers were sharing learnings from the trials which they deemed to have benefits for mainstream services also. Therefore, the above features may be beneficial aspects of perpetrator interventions more broadly.
The evidence presented in the following sections outlines the ‘enablers’ of these features, and any ‘barriers’ (what challenges still exist) to achieve each of these key features.
4.2 Trusting relationships
In order to fully engage in an intervention, people who use violence first need to acknowledge their violent behaviour. Their willingness to honestly admit to violence, and demonstrate a need to address this, is most likely to occur when participants feel safe and trusted by those around them.
Participants reported that the stigma associated with perpetrating violence was a barrier to being involved in a behaviour change program. This attitude was particularly prevalent among male participants, but in some cases also extended to women who use force and LGBTI participants. Some male participants indicated that they felt ‘judged’, ‘attacked’, or ‘threatened’ by programs for people who use violence. Therefore, overcoming this feeling within participants, by gaining their trust, was a key component of the perpetrator intervention.
Well, there isn't probably that many services for men. I'm not 100% saying that that's true or not, but in my eyes, there's probably not that many for men and if there is, it has got that stigma behind it… It reflects badly on you, but it shouldn’t reflect badly. You're out there to try and help yourself and it shouldn't ever - nobody should ever feel bad about themselves for doing something for themselves.
Really, I’m feeling better when I share the things with him and I know it’s confidential and all that and I’m feeling positive energy with him.
4.2.1 Trusting relationships - ‘enablers’
Service providers found that once trusting relationships are formed between the participants and their facilitator and/or fellow group members, a deeper level of engagement is reached.
4.2.1.1 Trusting relationships between facilitators and participants
Cohort trial and case management facilitators stated that in cases where they are able to create trusting and positive professional relationships with participants, this was the avenue to achieve reliable and consistent contact between the facilitator and participant.
Most participants highlighted that the programs had helped them to feel safe and comfortable to discuss challenging topics. Participants reported that they valued the ‘non-judgemental’ approach adopted by program staff, as they felt that they were in an environment where they could discuss their behaviours. This enabled the case worker to focus on the needs of the individual in order to address their use of violence, through a lens of accountability. For many participants, this was a new experience.
Emotional support… when you're a kid, when you're a male, your emotions get compressed by other people, like you know, 'man up,' 'be tough,' you know? 'Be strong,' 'don't be a wuss,' you know? And you compress that. But he got in there, and yeah, it was quite – he opened me up like a can of worms.
ust the fact that you talk through problems, talk through scenarios and they make you feel comfortable, they don’t judge you… As bad as the truth is, they don’t judge you. And you walk out feeling – walking out a better person.
4.2.1.2 Closed group format
All the cohort trials adopted a ‘closed-group’ format, whereby the same attendees would be present each week, and new members could not join after the first week. This approach is in contrast to a number of mainstream MBCPs which are ‘open’ or ‘rolling’ groups, meaning that participants can join or leave at any point in the program, and therefore there is variation each week.
The group-based support in cohort trials generally involves multiple individuals of similar backgrounds or social contexts taking part in weekly group sessions. This dynamic whereby participants shared common experiences is reported to have generated a greater level of rapport and support among group members. This was an important factor in providing additional motivation for attendance and engagement in the intervention.
Some participants indicated that it was beneficial for them to be in a group of people who shared similar experiences. This was particularly evident among LGBTI participants, as well as women who use force, with participants from both cohorts indicating that they had previously struggled to find suitable services prior to engagement in the program. Some participants talked of the importance of being part of their ‘community’, highlighting that this had helped to create a comfortable environment to address their behaviour.
It was so, I suppose, a comforting feeling and we knew that we were all there through traumatic circumstances of some type, it was a safe spot. It became a real safe spot that we looked forward to going to. (Person who uses violence, Cohort Trial, Women who use Force)
You feel really supported… It makes you feel really connected just to have people there. I've made a lot of friends through the group… Having that connection with other people who feel the same way that you do, and being able to share your experiences with each other, really helps. (Person who uses violence, Cohort Trial, Women who use Force)
It was in some cases, however, important for providers to monitor the status of these relationships, through awareness of participant interactions and conversations, to ensure collusion between participants would not occur, whereby they would justify each other’s use of violence.
4.2.2 Trusting relationships - ‘barriers’
For some case management participants who also attend mainstream MBCPs, they experienced difficulty developing connections with other participants, which in turn impacted on their ability to engage. Some highlighted the diversity in experiences and backgrounds among participants as something that impacted on the group dynamic, including a mixture of mandated and voluntary participants. For example, participants without children noted difficulty in being able to relate to participants who were parents.
There’s me and one other guy in there that don’t have kids, all the other guys have kids. Sometimes the group becomes a bit kid focused (Person who uses violence, Case Management)
You're sitting there with 20 guys, and you're not really – you know, same thing over, and over again, and they're not listening to it. He said, “I just rocked up, paid the money, sat down, nodded my head, and went back home.” And I don't think that's – it must work for some, but… it's very hard to be heard, and felt like being heard in a group… eventually you’ll open up in one-on-one, and understand more. (Person who uses violence, Case Management)
Whilst these participants are able to develop trusting relationships with their case manager, there is still a challenge that exists whereby they feel somewhat isolated from ‘peer support’, which, as indicated above, can be an enabler for addressing violent behaviour.
4.3 The complementary nature of individual and group work
Both group work and one-on-one case management each play an important but distinct role in the behaviour change process. It has been acknowledged in a number of large-scale studies that the incorporation of individualised case management approaches to complement group MBCPs will assist to increase readiness for group work, and reduce program drop-out [2]. This ability to support group-based interventions with one-on-one case management was recognised a top priority for MBCPs in Victoria [3].
But if I went straight and did the group, and then walked away and didn’t do the individual sessions, I don’t think it would have been as positive as a result. Definitely going in and almost debriefing was very important after the group.
The one on one probably more beneficial on your own situation but I would say they work well together.
The course is essential, I reckon, the group work. But the one on one's good too. Yeah, I couldn’t discredit either of them as being not worthy. But you've got to do the course first, I reckon. For sure.
Five out of seven cohort trials offered a combination of group and one-on-one work to their participants. A number of case management providers offered this one-on-one support to people who were also participating in mainstream MBCPs.
Providers reported three main reasons for offering more intensive individualised support in parallel with group work:
- providing additional educational support to participants who are struggling to grasp concepts covered in the group sessions
- preparing individuals for group support by addressing higher level needs or their willingness to undergo behaviour change
- addressing complex needs that had not been addressed previously by mainstream services.
4.3.1 Providing complementary individual and group work - ‘enablers’
4.3.1.1 Providing additional support
As described in Section 4.2.1, the closed-group nature of cohort trials generated an environment of trust and support among group members. This had the benefit of facilitating peer learning, resulting in group participants supporting each other through the change process.
In addition to being supported through the sharing of common experiences, participants were exposed to the different ideas and opinions of other group members. Some participants noted they learned things from groups that they otherwise would not have.
Sometimes I don’t know what I don’t know. So when I’m sitting in a group, I can hear somebody else’s story and identify something that I didn’t know. Whereas if I was doing one-on-one I can’t really identify those things...
I think in a group you learn new ideas as well, people be there to contribute new ideas through experiences they’ve had in life...
Being a group environment you, I, find that I learn a lot from observing others. So by watching, when the new guys came in, there was a guy that came in who had sort of drug problems and his relationship was breaking down. And he was sitting there really owning his shit, and sort of talking through everything really candidly. And I found it really helpful because I saw myself in him. So listening to his story and hearing what we was going through and hearing the emotional, the feelings that he was feeling. And the way that he was overcoming it. Things like that I started implementing those things for myself to.
However, many participants indicated that they felt more comfortable sharing their experiences in a one-on-one setting compared to a group. Participants stated that they would be anxious about opening up in a group context. Building trust with a case worker one-on-one encouraged participants to discuss sensitive issues.
Sometimes when you’re in the group sitting there’s certain things that you feel too afraid to face, or questions that you might feel are too stupid to ask. I feel like if you have that one-on-one time, it could give you the opportunity to ask something without facing – inner demons or self-doubt...
One on one’s a little bit more intimate I suppose… I’m a bit weary I suppose of talking about myself to other guys. You feel a bit vulnerable.
It's more confidential - it's more private, I suppose. Yeah, it's more comfortable. You haven't got the pressure of having 40 eyes looking at you.
Some participants mentioned that case management allowed them to identify specific causes and triggers of their behaviour, by facilitating a greater self-understanding. They considered that having a case worker who was able to understand their unique circumstances was an integral component of this.
[Case Worker] would look at different angles, okay. ‘what are the things that are attached to my relationship that actually have gone to take an ugly turn?’ Then he would find all the causes… identifying these things and then controlling them… and then implementing on yourself… it was a rigorous sort of approach…
When program staff work individually with people who use violence in conjunction to their group work, they are able to tailor behaviour change strategies to the specific needs of the individual. This tailoring assists people who use violence with their learning by focussing on specific and relevant aspects of things covered in the group work.
So it was important to me to have that contact with [Case Worker] afterwards, just to chat. I mean, we went over some of the things in the course one-on-one, some of the things that were relevant to me, some of the things that weren’t, some of the things other people concentrated on them and I wanted to talk about me. It was good to do. I would strongly say to any of the guys who finish that course, go and have a couple of one-on-one sessions for yourself. For no one else, just for yourself.
How I could essentially fix my shortcomings. I liked the - the Men’s Behaviour Change program the group aspect, was quite enlightening. But it wasn’t personalised I suppose, or individualised and I like that with the one on one sessions. Where I could explain different aspects about me, and how certain things specifically affect me.
Well yes, they went more in depth here with my personal issues. More so than, as what I had in the men’s behavioural. And ongoing issues that were arising. So yes, it’s been more focused around what I’m dealing with at the present. And ways to get around that.
Individual case managers were also able to monitor participants as they progressed through the group program, and provide additional support to participants if they identified any challenges. Participants reported that meetings with their case worker involved ‘touching base’ and unpacking topics from group sessions.
Every four weeks we have a one on one instead of group. For a check-up of how you’re doing and what’s new or if you’re having a hard time… It’s a tell-all just so the instructors know we’re on the same level...
I see for one-on-one sessions just to catch up. That's usually once a week, every fortnight, whatever, just to see how I'm going with the program and if everything is all good. She just likes to check up on me.
4.3.1.2 Group readiness
The ability of one-on-one work to address barriers to individuals accessing perpetrator intervention programs is often crucial to their continued engagement in support. Removing barriers to engagement is often necessary for people who use violence, as some are living with multiple issues including physical health, mental health, social and/or economic instability. Providers found it difficult to focus on accountability and strategies for behaviour change when a person was in crisis or had a number of physical and social support needs that needed follow up. Supporting people to meet their basic physical needs (particularly in times of crisis) creates additional time and space for individuals to attend the group sessions and address higher level needs. Additionally, individuals exhibiting low readiness to change at the time of referral or with complex needs often require additional intervention/s so they are more able to engage in a group work process. Due to the one-on-one component of most cohort trials and the addition of case management, individuals received more individualised support. This approach increases the inclusivity of perpetrator interventions to those who are not suitable at the time of referral. It provides an opportunity to educate the participant about the support they will receive through group work, and the need to take accountability for their violent behaviour. Further, with the inclusion of these individuals in case management support, this also means the person who experiences violence will also be contacted for support. Previously they would not have been engaged unless the person who uses violence was.
Many participants expressed difficulty with the concept of taking responsibility for their behaviour. Some participants talked of needing to be at a stage where they felt ready to accept responsibility and commit to the program.
It took me a bit of convincing that this would be the right sort - I was sort of afraid to go into a program like that. Sort of found it a bit scary and then I thought, oh, my situation isn't that bad; I don't need this program.
I think there's definitely always going to be women who aren't quite ready… [to] actually accept that, maybe you could have done things differently. If you don't think you're wrong in any way, shape or form, then it's really hard to look forward and change behaviour… I definitely think you'll always get those women that, for no other reason, than they're just not quite at that point.
For some participants, they may never be ready for group work and therefore will continue with one-on-one support for the duration of their intervention. The availability of ongoing one-on-one work is an important focus of the new case management program, as it increases the service delivery options for people who use violence but may not be suitable for MBCPs.
4.3.2 Providing complementary individual and group work - ‘barriers’
Whilst there are obvious benefits to offering both group and individualised support as part of perpetrator intervention, this does have an impact on the resources available to deliver this more intensive level of support. In some cases, providers noted that the burden on staff to meet the demand for individualised support was greater than anticipated. This included both the time commitment, as well as burn out and the effects of vicarious trauma in some cases. For those providers who did not offer both group and one-on-one work, one of the reasons given was the lack of staff capacity to undertake this.
4.4 Addressing accountability with a trauma informed approach
Providers of the programs included in this evaluation (both cohort trials and case management) were aware that unless there is an element of ‘healing’ in the behaviour change process, there is unlikely to be a lasting change in the use of violence. This was particularly evident when working with women who use force, LGBTI people, Aboriginal and Torres Strait Islander people who use violence. Providers of programs for these groups explicitly designed their interventions to acknowledge and address trauma, as indicated in the funding submission for the program for the LGBTI cohort trial:
When working with clients, we will be guided by trauma informed approaches and use a trauma lens that explores the motives, dynamics and context for the violence so that they can be properly addressed. In addition, we will assess current victimisation and personal safety and will use a client centred approach to explore the existing strengths and resources that clients can utilise in their journey to take responsibility for and stop using violence.
4.4.1 Addressing accountability with a trauma informed approach – ‘enablers’
4.4.1.1 Recognising past trauma
Participants in the program for women who use force indicated that a key focus of the program was recognising the relationship between past trauma and current acts of violence. The women identified themselves as ‘victims’ of family violence, while still also being recognised as ‘perpetrators’ of violence. By addressing experiences of victimisation, the intervention aims to facilitate a change of mindset to one of accountability, which then leads to behaviour change.
Providers employed frameworks and techniques in order to shift participant’s perspectives, using techniques designed to demonstrate the lasting impact that their violence has had on others, whilst also recognising the trauma they themselves had experienced. This enabled them to link their experiences of trauma with their use of violence:
I was seeing [Case Worker], and she was probably one of the better kind of people that I've worked with in dealing with some of the trauma that over the past has accumulated and she was really incredible. Like, she knows the intersection of queerness and how we use violence and how that manifests.
4.4.1.2 Enabling self-awareness
Many participants discussed how the program helped them to understand their own behaviour, and improve their knowledge of family violence more broadly for example, that it does not pertain only to physical abuse.
It's for women who were at a point in their relationship where there's some type of family violence and they have now lost control of how they would respond to that situation, and respond out of desperation, which in turn, makes them do things that they wouldn't do under normal circumstances.
I saw lot of family violence as a child, and there are things that I do to try to protect myself from those happening, that also is a form of family violence. So like, I did those things because I'd seen so much.
Additionally, a trauma informed approach addresses the intersection between the work being undertaken with people who use violence, and the engagement with people who experience violence. Trauma informed practice focuses on physical and emotional safety, in seeking to support empowering relationships for both parties, underpinned by an awareness of the impact of violence on others.
The ‘A Better Way’ program utilised by Anglicare and VACCA highlights this approach particularly for Aboriginal clients who have experienced intergenerational and cultural trauma which intersects with their violent behaviour. Their intervention approach includes “understanding the impact of the perpetrator’s behaviour on Aboriginal children and the victim-survivor’s right to cultural practices and connections”.
4.4.2 Addressing accountability with a trauma informed approach – ‘barriers’
Whilst not necessarily a barrier to success, it is essential these trauma-informed approaches are always delivered within a framework of acknowledging accountability for the use of violence. Many people who use violence have a perceived sense of victimisation, which they use to justify their own use of violence. Multiple examples were given by providers of participants entering into an intervention with the perception that they were the victim in their violent situation, and that other people were responsible for their violence. Enabling people who use violence to be able to acknowledge and take accountability for their violent behaviours is a primary purpose of perpetrator intervention programs.
4.5 Holistic intervention
In order to increase the inclusivity of perpetrator interventions in Victoria, it was important to address the factors that make mainstream services inappropriate for certain cohorts. This was done by identifying the contextual factors that may be contributing to violent behaviour, as well as the potential barriers to engagement with services.
For most participants interviewed as part of the evaluation, the cohort trial or case management intervention they were involved in was their first time receiving assistance for family violence. Providers noted that, for many participants, it was clear that they had experienced a somewhat turbulent pathway through the service system, accessing a number of ad hoc or short-term interventions, prior to engaging in the current program. It was therefore necessary for the program staff and case managers to play a role in identifying and assessing each individual’s range of needs, in addition to addressing their use of violence. Whilst these needs do not provide justification for the use of violence, they do impact on the ability of individuals to participate in in the program and commence a meaningful behaviour change process.
4.5.1 Holistic intervention – ‘enablers’
4.5.1.1 Delivering wrap around services
A number of providers had a formalised assessment or intake process incorporated within their referral process, in order to understand the complexity of an individual’s needs, and therefore provide them with the required level of support. Once a cohort trial or case management provider has identified underlying concerns or needs for a participant, they are able to connect them in with the relevant services. Common examples included employment programs, housing services and court support.
Mental health and alcohol and other drug comorbidities are common amongst the people who use violence accessing these interventions, as discussed in Section 3.5.1. Therefore, providers commonly adapt their approaches to accommodate these needs and connect participants to appropriate supports. Specifically, neuropsychological assessments are being accessed by participants through brokerage funding.
Some participants talked of being referred to counselling, drug and alcohol support, and parenting programs by their provider in participant interviews. In many cases, it appeared that general conversations about being referred to other services had been held, however there was varying levels of actual translation into engagement in services at the time of the interviews. Reasons for a potential lack of engagement in other services is discussed further in Chapter 7.
I’m starting couples counselling shortly through [Provider]... And that will be good, but yeah, it’s just some sort of counselling and sort of talking to them about other ways that they can help... [Case Worker]’s been quite proactive about getting me in touch with the counsellor that deals specifically with family violence.
[Case Worker] has recommended trying to get me involved with a doctor or a counsellor that specialises in ABI personalities, so I’m interested in how he approaches that because that would be encouraging to me.
She understands where I’m coming from, supports, she’s pointed me in directions that I was asking. Housing, men’s behaviour, talking about that, place I could go. Other organisations I suppose that could help out in what I’d been asking her… just for places to stay, emergency accommodation and stuff like that. Other men’s help lines. Places to eat… just stuff like that… I kind of use [Case Worker] as my main service rather than going to those services… I stick to what I know.
Additionally, a small amount of brokerage was provided to case management providers. The intention of this brokerage is to assist people who use violence in circumstances where they may be experiencing crisis (e.g. homelessness) or to address a barrier which is preventing their engagement in the service (e.g. taxi vouchers). Providers reported that this assistance enabled them to offer flexibility in the assistance they provided, and respond to men’s needs as required.
Results from the FSV brokerage data showed that the top five uses of brokerage were as follows (noting that this does not reflect the total spend in each category):
- immediate basic needs
- transport
- physical and mental health and wellbeing
- support for social engagement
- short-term accommodation.
Case study
An elderly man was referred to a case management provider due to his lack of group readiness. The initial assumption from the case management provider was that his problem with engagement was due to his poor proficiency in English. He began to attend case management weekly and over the course of the engagement, the case manager noticed the participant experiencing significant issues with memory and orientation (to time and space). Through following up on this observation, the provider was able to determine that the participant had early stages of dementia. Following this diagnosis, the provider connected the participant to community support, aged care and mental health treatment. Once his health was being treated, the participant was a lot more engaged with the intervention. The provider was able to organise support in order for him to attend meetings and groups which allowed for this increased engagement.
A secondary benefit of wrap around service provision, particularly where individual support was provided, was to enable the participant to have one person to correspond with regarding all of their needs. Case managers reportedly assisted with communicating between the individual and external services, particularly in situations where there had been no follow-up or communication had broken down.
Participants indicated that they were also able to contact their case worker outside of sessions, usually by calling them or sending a text message, and generally reported that their case workers were always accessible and responsive.
I was in touch with him through text messages and all that as well. If I needed anything I would just ask him and even he would just say how things are going, he would just text me and all that. So that, the contact was always there.
Even outside of the program, like sometimes I’ll email [Case Worker] and she’ll be in contact with me within the day. Or if I’ve called [Provider] and asked to speak to them, they’ve been available. They’re very, very available.
4.5.1.2 Increased visibility
A secondary benefit of providing a more holistic intervention to people who use violence, which touches on different aspects of their life, is the greater insight into individual needs case workers gain which in turn contributes to a more accurate picture of risk. The primary purpose of these interventions is to increase the safety of victims of family violence. By providing a more intensive service to people who use violence, particularly involving an element of one-on-one work, case workers gain a deeper contextual understanding of the person’s situation, and consequently the interactions they may be having with the person who experiences violence.
4.5.2 Holistic intervention – ‘barriers’
4.5.2.1 Brokerage
Despite the intended benefit of the brokerage funding to enable a more wrap-around support by meeting the basic needs of case management participants, large amounts of the brokerage funding in the first twelve months went unspent. Only 14% of the total allocated brokerage was acquitted, as at October 2019.
Anecdotally, there is a hesitance to provide financial assistance to perpetrators of family violence due to the potential or perceived risk that this may be supporting their use of violence. This has led to difficulty in making decisions about how brokerage can be spent appropriately, and to ensure it meets the expectations outlined in the guidelines. However, many providers report that they are spending greater amounts of brokerage as the case management program becomes embedded, as it took them some time from when the funding was released to get their case management programs up and running. The brokerage spend increases across each quarter are shown in Table 4.1. This is the first time brokerage has been allocated to programs for people who use violence, and both FSV and providers are undertaking work to better understand best practice in this context.
Table 4‑1: Quarterly brokerage spend
| Total spend by quarter (thousands) | Accumulated spend as a percentage of total allocation | |
|---|---|---|
| Q1 2018-19 | 4.8 | 0.5% |
| Q2 2018-19 | 16.9 | 2% |
| Q3 2018-19 | 42.1 | 6% |
| Q4 2018-19 | 46.4 | 11% |
| Q1 2019-20 | 32.6 | 14% |
4.5.2.2 Burden on staff
As has been previously mentioned, the more intensive, wrap-around nature of the new programs, as compared with traditional MBCPs, can lead to over-burdening the case workers, many who have large caseloads. In some cases, the support goes beyond the scope of their role to provide case management in the context of a family violence intervention. One cohort trial provider indicated that the intensive nature of this wrap-around support was leading to staff burnout. Providers should ensure that program facilitators and case workers understand the scope of their role, and the limits of the support they are expected to provide to participants. Ongoing supervision should also be provided to staff members to ensure they are receiving the necessary support in order to undertake their role, and to mitigate burnout. Providers indicated that supervision typically involves both fortnightly individual sessions (or on as as-needed basis), as well as frequent group supervision which is often more informal, and involves sharing experiences and learnings with other facilitators.
4.6 Flexibility of interventions
People enter perpetrator intervention programs with different needs, different life circumstances, and at different stages of change. Therefore, these programs need to demonstrate flexibility to cater for different levels of motivation and individual contexts to keep participants engaged. This aligns with the TTM model outlined in Chapter 3.
In addition to group readiness as outlined above, due to individual circumstance and characteristics, individuals will progress through perpetrator interventions at different rates. By acknowledging this difference, facilitators can adjust their approach and expectations to allow for long term progression.
4.6.1 Flexibility of interventions – ‘enablers’
4.6.1.1 Flexible delivery model
When delivering cohort trials and case management, providers have demonstrated flexibility in approaches, considering individual need. Examples of flexible approaches include:
- The women who use force cohort trial model had a structured 16-week curriculum, yet depending on the needs of the group on the day, the order of the sessions could be tailored.
- The LGBTI cohort trial also demonstrated high levels of flexibility in what the topic of each session would be, through regularly asking participants what would be most helpful for them to work on each session. The provider also demonstrated flexibility in the intensity of the service provided to participants, for example whether they needed more frequent one-on-one support depending on what else might be happening in their life at the time.
- Cognitive impairment cohort trials utilised visual tools and hands-on activities for participants who did not respond as well to more traditional forms of communication. They also noted that mainstream facilitators had become more flexible and more aware of cognitive impairment presentations in their groups since the implementation of the cohort trial.
- Some case management providers indicated that they did not put a cap on the number or frequency of sessions a person could access.
The flexible nature of support was highlighted by many participants as a positive aspect of programs. Part of this pertained to the flexibility of what was covered in sessions. For example, some cohort trial participants noted that despite there being overarching structure to groups, most sessions were fluid.
It allows open conversation, you can get what you want out of it… it's not structured to the point of, 'No, now we're talking about this.'
In the one on ones or if we’re about to start group or coming back from the break, the case worker takes the time to approach me then and ask if everything is all right… they’re quick to pick up on if I’m really angry.
The flexibility of case management was appealing to participants as it allowed them to combine paid work with attendance in the program.
I work full-time, and I'm able to go at my lunch, which has made it a really, really good, really good thing to have for me, otherwise I wouldn't be able to do it. I would have had to basically change jobs, or quit my job to do the other courses other organisations wanted me to do. It didn't work, it was ridiculous what they asked me to do, but [Provider] have worked around it, and made something very easy.
I think even when I first started looking at this [Provider] stuff that one or two providers came back and said, “Yeah, we do sessions” or “we can do your interview at this time.” It was during business hours. And I said basically I can't just give up my work to be able to do these things, so it's got to be a bit more flexible.
Participants appreciated the flexibility in the timing of individual case management sessions. Participants discussed that case workers were generally available and willing to schedule or re-schedule sessions to a time most convenient to participants. This compared favourably to traditional MBCPs, which run at set times on a weekly basis.
Oh yeah, no, it was – I don’t think I would have finished the program if it wasn’t for that. I really don’t think I would have finished the behaviour change thing because that was the only reason why I really stuck with it was because I was able to do it easily the whole way through…The flexibility was great, and the actual position of it, it was – like, it took me like a minute and a half to drive there. That was probably the best thing about it.
4.6.2 Flexibility of interventions – ‘barriers’
4.6.2.1 Program timing
Although some cohort trial and case management providers did make an attempt to provide flexibility for participants, participants did find the time commitment a barrier to participation. This related to both to the total length of some of the programs, as well as the times available to attend the programs. These considerations appeared to be of particular relevance for participants receiving group-based support, and was most problematic for participants who were currently working.
Six months is quite a long time… Some people will look at the duration, it may be too much for them, because it’s every week… so if you combine that with work and other stuff, some people may feel it’s too much.
Relating to case management, some participants highlighted that a 20 session program was a big commitment for a lot of people, particularly as this was to be balanced with competing demands, such as work, family, and for some, legal cases.
I’m at uni full time and I’m trying to do this on the side plus I’m trying to have my relationship with my partner… And I’m also trying to look for a new house and – so it’s just a lot on and I’m doing also drug recovery, so I’m doing narcotics anonymous and my meetings, and I’m just constantly around the clock.
4.7 Family safety contact support
Both case management and cohort trial providers work with partners or ex-partners and child(ren) of people who use violence (where they wished to be involved). This occurs via contact with the Family safety contact worker, and the level of support varies based on the program structure and the needs of the individual. For example, some people who experience violence have access to face to face sessions with the Family safety contact worker, whereas others receive phone calls or information via email. Of the people who experienced violence for which data was recorded, sixteen of the 58 responses of those associated with the cohort trials had previously accessed specialised family violence services, and 20 of the 99 responses associated with the case management program [4]. Where the person experiencing violence is already engaged with a specialist family violence service, the family safety contact worker will liaise directly with that service with their consent.
Two cohort trials are explicitly providing family safety contact support for children of participants. Others are providing indirect support to families of participants, primarily through assistance with Child Protection matters.
4.7.1 Family safety contact – ‘enablers’
4.7.1.1 Tailored support
Discussions with the family safety contact worker involved ‘touching base’ to see how the participant had been going, and to check if they had any safety concerns. Some participants indicated that the family safety contact worker would update them on how the person who used violence was progressing in the program, although there were limits with what they were able to disclose. People who experienced violence appreciated having the family safety contact worker, noting that it was beneficial for them to have someone available to listen to their story and acknowledge their experiences.
As with the people who use violence, having someone trusted to speak with was also emphasised as an important benefit among people who experience violence. This cohort noted that having someone who could acknowledge their struggle and support them was integral to their recovery process.
I felt like she was listening. Yeah, I felt like she was actually listening and she was there to help me and not just ticking the boxes and moving on to the next question… I love that [Case Worker] listens to me, to my needs.
And just to have somebody there who – with the confidence to go no, this is wrong. And it is really supportive and it’s really good to know that you’ve got somebody on your page… as an advocate… it means more than they know.
People who experience violence derived value from the family safety contact function when they were made to feel empowered and gained confidence as a result of their support.
So, that’s why [provider] is such a godsend to some people. It’s such a valuable, a resource to use and it just gives you the confidence to be able to do what you need to do. Like report those breaches that you’re going to get laughed at or you’re going to get told that, no, no, no, that’s not a breach. Well, yes, it is.
Earlier on, some participants indicated a need for more tangible support, such as counselling, referral to other services, or financial assistance, noting that support from the safety contact was often limited. However as the trials progressed there was evidence to suggest that some people who experience violence are gaining greater access to other support services. For example, psychology appointments, English lessons, lawyers and financial counselling.
4.7.1.2 Increased visibility
Case management and cohort trial providers agreed that partner feedback is a more accurate indication of perpetrator behaviour change compared to feedback from clients themselves. Where the person who experiences violence is engaged in support via the family safety contact function, they can provide information with which to either substantiate or contradict the person who uses violence’s account. Providers who engage with partners and ex-partners can collect and record their feedback and can use it to better understand participant progress.
Some people who experience violence stated that their communication with the family safety contact worker involved corroborating the veracity of claims made by the person who used violence.
I don’t meet with [Husband]’s case worker… he calls me fairly regularly… to see if what he’s been told is true and correct in [Husband]’s session (Person who experiences violence, Cohort Trial).
This also means that in an event where risk may escalate, the provider has a means to notify the person who experiences violence, and provide support as required.
4.7.2 Family safety contact support – ‘barriers’
4.7.2.1 Association with the person who uses violence
Once people who had experienced violence had been contacted by a provider, a unique barrier to participation was the reluctance of the person who experiences violence to be involved with the same provider that was also currently engaged with the person who uses violence. This was particularly relevant for participants whose relationship with the person who used violence had ended. They reported that deciding to be involved in the program was difficult due to the perceived association with the person who used violence.
There was also some hesitation reported by some people who experienced violence regarding broaching the topic of program participation with the person who used violence, with the fear of retributive violence evident.
There was also one example given which suggested that the role of the family safety contact worker was being used to facilitate engagement with people who use violence, rather than support people who experience violence. It is important that FSV provide communication to providers to ensure this practice is not a systemic issue and that it does not occur in the future.
4.7.2.2 Resourcing
There was also feedback from providers that there were some issues with appropriate resourcing for the family safety contact function. Some providers indicated that this role was not a large focus of their program, and was often shared with the mainstream MBCP also delivered by the provider. As these mainstream programs have a large number of participants, the family safety contact worker would be over-capacity in terms of their caseload once taking on additional case management clients, and therefore not able to dedicate a sufficient amount of time to this work.
Family safety contact funding is bundled within the unit price of a working with a person who uses violence for these programs. With this funding structure, providers have typically chosen two frameworks to offer family safety contact support. The first framework is that a new cohort trial or case management program is set up to work with people who use violence and the family safety contact role for these new participants is allocated to an existing team within the organisation that works with people who experience violence. The second framework is that the same pool of workers that work with people who use violence, also work with those who experience violence. There was one example of a provider hiring a new staff member to exclusively offer family safety contact support for the partners of the participants in a new cohort trial.
[1] This includes the cohort trials which incorporate both individual and group aspects, as well as people engaged in the case management program who also participate in mainstream MBCPs, noting that MBCPs are out of scope for this evaluation.
[2] Centre for Innovative Justice (2015). Opportunities for Early Intervention: Bringing perpetrators of family violence into view.
[3] No To Violence, Men’s Behaviour Change Programs in Victoria – a Sector Snapshot, April 2011. At https://ntv.org.au/advocacy-media/resources/#publications.
[4] Deloitte Access Economics data collection tool. Note: For the case management people who experience violence, 33 out of 51 responses were left blank. There were no blank responses for the cohort trials.
Approaches for specific cohorts
Key findings
- While there are overarching design features that contribute to good practice, there are also specific design features that are appropriate for particular cohorts.
- For Aboriginal cohorts, cultural healing and connection to culture and country is an important feature, so they are able to first address their own healing from past trauma and grief, in order to subsequently address their use of violence. Further, engagement with Elders, sufficient time to deliver and implement the programs, meaningful partnerships and Aboriginal design and delivery are important success factors.
- The program for CALD participants delivered the program in a culturally appropriate manner, including applying a cultural lens to mainstream materials, and having facilitators who belonged to the two cultural groups. This enabled facilitators to explain concepts and information in a manner that could be better understood by participants. The Family safety contact was also an important feature of this program.
- There are some parallels for the LGBTI and women who use force cohorts in terms of enabling participants to heal from violence/trauma and the use of peer support.
- For people with cognitive impairment, the program is a more resource-intensive version of the MBCPs. This is because the small group size, slower pace, specialist workforce and closed group are important features contributing to participant engagement (but are also more resource intensive). Using prompts and visuals has also been beneficial.
5.1 Introduction
Based on the findings from the Royal Commission, FSV sought submissions from service providers to provide community-based perpetrator interventions specifically designed for the following target cohorts:
- culturally and linguistically diverse, including new and emerging communities
- gay, lesbian, bi-sexual, transgender and inter-sex communities
- Aboriginal communities
- females (referred to in this report as women who use force)
- fathers, and/or
- perpetrators with complex needs including drug and alcohol, mental health and cognitive impairment.[1]
This section examines specific design approaches adopted by providers to service the needs of the aforementioned target cohorts, and the effectiveness of these design features. It focuses on the cohort intervention trials, and the case management where the provision of case management targets these cohorts (i.e. Aboriginal case-management providers). As noted in Chapter 3, a gap still exists for a program for men with complex needs, including mental health and AOD issues, as FSV were unable to identify a provider with the required capacity and expertise to deliver this service. Nonetheless, a large proportion of the case management and cohort trial clients had a mental health and/or AOD issue (as assessed by the service provider).
Additionally, data obtained via the data collection tool shows the diversity of participants receiving services via the new community-based perpetrator interventions and case management trials. This is shown for each program type, in Figure 5.1 [2]. It must be noted that total numbers, rather than proportions, are reported due to the large number of blank responses in the data collection tools. Appendix D provides a more detailed view of the responses for each domain, including the total numbers for each response option in the tool, and the number of blank responses.
Participant demographic data – case management (total participant responses = 710)
- 432 are male, 6 identify as transgender
- 267 are under 40
- 336 identify as heterosexual
- 65 identify as Aboriginal and/of Torres Strait Islander
- 419 speak English at home
- 306 have children
- 93 have a history of homelessness
- 256 have mental health and/or AOD issues.
Participant demographic data – cohort trials (total participant responses = 159)
- 117 are male, 8 identify as transgender
- 105 are under 40
- 117 identify as heterosexual
- 17 identify as Aboriginal and/of Torres Strait Islander
- 109 speak English at home
- 126 have children
- 24 have a history of homelessness
- 87 have mental health and/or AOD issues.
Source: Deloitte Access Economics data collection tool
5.2 Culturally and linguistically diverse, including new and emerging communities
There were limited services targeting people from CALD communities that were able to be appointed as a cohort trial provider. FSV reported submissions from CALD communities typically focused on a community prevention response, which was not the intention of the trials. Further, there were submissions from numerous CALD community organisations that did not have the requisite skills in family violence, including working with people who use violence.
InTouch were awarded the tender to provide the CALD cohort trial to newly arrived migrants and refugees from the Hazara (Afghani) and South Asian communities. In 2019/20 this will expand to include programs for African and younger men (18-20 years). Their approach involves a trauma informed approach to address the identified needs of this cohort, related to the intersectionality of their violence from experiences of migration, war and racism, as outlined in Chapter 3. The Afghan groups are run in language and culture as many participants have not been educated in English. However, the South Asian groups are run in English and are open to men from eight countries across South Eastern Asia, including India and Pakistan. Motivation for Change participants receive weekly group work and case management. Effective elements of program delivery are outlined in the following sections.
5.2.1 Culturally and linguistically appropriate
Delivering interventions in a culturally appropriate manner for multicultural cohorts aids participation and engagement. InTouch reported that they were able to deliver the groups in a culturally appropriate manner by applying a cultural lens to mainstream materials, and that this helped participants to better connect to the program content and each other through sharing common cultural aspects. This also provided opportunities to dispel common ‘cultural’ and other myths and excuses that can often be used by some men as justification for their use of violence.
Delivery of the program in the first language of participants improved participants understanding and comprehension of family violence. One group (for South Asian men) was delivered in Dari; the first language of participants. This addressed a barrier to these men being able to previously access perpetrator services, and enabled facilitators to explain concepts and information in a manner that could be better understood by participants.
It’s done in English. But, at the same time, if somebody doesn’t understand things, they can explain in, say Hindi or Gujarati or a different language, because they’re multilingual.
It’s on our own language so we understand 100%. If course go to English rather than my own language, or go other languages, we might not understand. On other programs we just say “Yes, yes, yes” but don’t understand.
Further, the program incorporated shared cultural norms, including facilitators belonging to the two cultural groups. For example, South Asian participants connected over shared family rituals such as marital contracts, which is not possible in mainstream groups. This is turn eased group dynamics, so much so that participants had to be ‘pushed out the door’ at the conclusion of the group.
But, it helped because most of the people were in the programme because they were all Indians or from the same environment. It helped because people opened up. They would talk. Whereas, like, if they had come from different backgrounds – say you were with Australians – you wouldn’t have the same situation, you know? You wouldn’t be able to explain your side of the thing as Australians or some other nationality. If everybody were Westernised, it would have been a different way of doing things. A lot of people wouldn’t join the programme if they were different nationalities. Because it was all similar – I think that’s why it was more comfortable. People were talking, and that. Otherwise, I think a lot of people would have just kept quiet and been there but not actually participated. They wouldn’t have come out and spoken freely, you know?
5.2.2 Community perception
In communities where family violence is considered taboo or poorly understood, there are increased barriers to accessing a perpetrator intervention. This appears to be true for the multicultural cohort. Shame associated with being a person who uses violence appeared to be a reason for some individuals not wanting to attend the multicultural cohort specific groups. To avoid their community members finding out about their use of violence, these individuals attended mainstream groups where their community members would not be present.
InTouch also identified the need to build capacity in the communities with whom they work to understand what constitutes family violence. Community consultation showed there was uncertainty regarding the context of the program. As such, part of the funding was used to build community understanding of the need for family violence programs. Building knowledge of what constitutes family violence was also a core feature and outcome of the program, more so than other programs (see Chapter 6). This may reflect the level of readiness within the community as it relates to understanding of family violence and challenging behaviours.
5.2.3 Referrals
Most referrals for this cohort reportedly came from Magistrates Court or Child Protection (with a small number of intra-organisational referrals from InTouch’s victim service), which can provide an incentive to participate. The data collection tool showed that 19 of the 36 referrals were from the courts. Although InTouch undertook outreach work to educate the community about family violence perpetration, this reportedly had limited impact on creating referrals into the trial.
5.2.4 Family Safety Contact
A history of providing services to women experiencing violence was a strength of the InTouch model for two reasons. Firstly, having the perspective of the people experiencing violence meant they were able to understand the family and cultural context in which they were working with the people using violence. This allowed workers to apply their knowledge of how the family unit operates within the cultural context, and apply that knowledge to the design and interaction of working with men. Secondly, it contributed to the family safety contact worker playing a particularly prominent role relative to other programs Family safety contact workers regularly met with those who were experiencing violence. This feature was highly valued among the women who received the support, and provided them with confidence and strategies to improve their and their child’s safety. However, the role has been more intensive that initially envisaged, and resourcing for the role is currently being shared across other programs.
Before the first time I have a –in the family violence I was really upset and I was really – I get confused and I didn’t know what then I do. Then I come to the [Provider] and talk with the lady…every month…it was really good and opened my mind, how I manage my life…how I’ve lifted myself and how can I protect my children…it was very good.
5.3 People who use violence who are LGBTI
Drummond Street services is delivering Futures Free from Violence, an intervention program designed for the trial for people who use violence who are cis women (heterosexual, bisexual and lesbian) and people who are transgender and diverse in the North Eastern Melbourne and Western Melbourne areas. The aim of this program is to engage women and trans and gender diverse people who use violence, address their underlying needs and identify individual drivers for change. A tailored response to address violent behaviour is developed for each individual participant, which includes both case management and group work. This response manages risk, increases safety for families and creates accountability, as well as addresses the trauma and victimisation many members of this community have experienced, which can lead to a mistrust of government funded and/or delivered services.
5.3.1 Community delivered and peer workforce
Community ownership and delivery has been a key feature of program delivery that has been highly valued by this cohort. Referrals reportedly stem predominantly from word-of-mouth within the LGBTI communities, resulting in high numbers of self-referrals. The data collection tool showed that 24 of the 27 referrals were self-referrals. Workers delivering the program identified as belonging to the LGBTI communities. Participants emphasised the importance of having specialised staff with lived experience to work alongside LGBTI people. This reportedly built trust and rapport between program staff and participants, and was highly valued by participants:
The two therapists that were running it, left the group and that changed. So, there's before that, it was very customised to everyone's needs and we all felt very seen and heard in that space, and then they changed the therapists to two people who weren't specialised in that area who didn't seem quite clear or didn't understand those needs, and so it did shift during the program.
Participants talked of the benefit of being in a safe and non-judgemental environment with other people from similar backgrounds. Having a safe space to discuss issues pertaining to family violence was seen as a crucial element of the program. One participant emphasised the importance of having a ‘community.’
It's actually very profound in a therapeutic sense because I think it's fundamental to being human, is being seen, especially when we're hurting, especially when we've caused hurt to other people. When you feel seen by, say, a community, something special happens, and that's why group is a powerful space.
More than anything, is building up a safety and a trust within the group who have similar lifestyles or similar viewpoints or similar upbringings and that similarity is the first thing that probably – and of course the absolute lack of judgement to people’s lifestyles that is going to be the first bond in any group.
5.3.2 Integrated service response and intensity of service
An integrated service response [3] with a high intensity of service provision, where required, was considered an important feature of the Futures Free from Violence program for several reasons. Firstly, it served as a risk management strategy, given participants could have also experienced violence themselves. This reportedly helped to create a more holistic picture of risk, as the provider was able to provide a range of suitable supports.
Secondly, for LGBTI participants, experiences of discrimination and/or judgement within the mainstream service system has prevented use of services, or distrust of some services. Providing more wrap-around support reportedly ensures that any additional needs can be identified and managed. Given participants have often been isolated from the service system, intensive wrap-around services are often needed.
Despite the intended benefits of the integrated service design, this model did present some significant issues in the delivery of this program. The level and intensity of the service being provided to each individual was greater than anticipated in the original design of the model. This meant that staff became overburdened, and case throughput was not being achieved. This resulted in the original target of 90 participants being reduced to 40. Further, the telephone response for clients was not implemented (initially part of the model design), which may have contributed to the intensity of the face to face support required.
One final aspect of integration has been that team members have worked across both the community-based perpetrator trial and the justice system perpetrator trials.
5.3.3 Healing from violence/trauma
One feature of the model has been its trauma-informed approach, as discussed in Chapter 4, recognising the ‘intersection’ between the experience of trauma and the use of violence in LGBTI communities. Participants noted that they had a history of trauma and violence, having experienced abuse themselves that influenced their presentation of family violence.
I was seeing [Case Worker], and she was probably one of the better kind of people that I've worked with in dealing with some of the trauma that over the past has accumulated and she was really incredible. Like, she knows the intersection of queerness and how we use violence and how that manifests.
5.4 Aboriginal communities
Bendigo and District Aboriginal Cooperative (BDAC) is delivering a culturally relevant program for Aboriginal men and non-Aboriginal men in Aboriginal families. The program’s delivery primarily occurs in bush settings with strong cultural healing underpinnings. The program is based upon the premise that before men can address their behaviour they need to heal from past trauma, loss and grief and that for some perpetrators their role as a parent is an important motivator for behaviour change. Healing is facilitated through 15 sessions that make use of programs, tools and resources.
Anglicare and VACCA are also delivering a program which includes participation of Aboriginal and non-Aboriginal fathers. The trial operates within a culturally safe and inclusive framework for the purpose of being accessible to a diversity of fathers.
Case management funding has also been provided to Aboriginal Community Controlled Organisations (ACCOs) to work with people who use violence who are Aboriginal. As is described throughout this section, some case management providers incorporated cultural healing elements into their case management program and interactions.
5.4.1 Cultural healing and connection to self-identity, culture and country
Recognising the inequalities and intergenerational trauma faced by Aboriginal people (see Chapter 3), a cultural healing component is an important design feature of interventions for people who use violence who are Aboriginal. Stakeholders identified it is necessary for participants to first address their own healing from past trauma and grief, in order to subsequently address their use of violence. [4] Several Aboriginal providers of case management and cohort trials expressed that this focus on healing helps to overcome the ‘root cause’ of violence. Addressing healing first was an explicit design focus of the BDAC cohort trial, while Anglicare adopted a trauma-informed model (Safe and Together) with a Cultural Therapeutic Framework to ensure a cultural healing approach featured in the program.
Different mechanisms were adopted to support cultural healing, such as story-telling, incorporating men’s business, and embedding cultural activities and practices and including Elders. Activities that supported connection to culture were identified as particularly critical for enabling cultural healing to occur (see case study). Components to support cultural healing were also combined. For example, one provider talked about how providing time for men’s business on-country enabled men to open up and talk about their experiences of family violence, facilitating the cultural healing process.
Case study
Through engaging with the local Aboriginal community, one of the providers of a cohort trial for Aboriginal people who use violence recognised that there was a strong desire to provide the opportunity for participants to create cultural items as part of the cohort trial. This feedback was then incorporated into the cohort trial through allocating participant time to creating cultural items - didgeridoos and clapping sticks. This time allocation was purposefully set in the afternoon, after the theme for the day had been discussed.
During this afternoon activity participants were provided with an opportunity to connect to culture. This alone was powerful for participants, particularly for men who had never had the opportunity to connect to culture previously. However creating cultural items also acted as an art therapy session. This is because the time spent creating cultural items facilitated the reflection process. During this time participants reflected on their trauma, family violence and how they had wounded and affected others.
The didgeridoos that the participants made were collected and saved after the session. They were then used again at the closing ceremony of the 12 week cohort trial. Elders participated in the closing ceremony and played the role of handing back the digeridoo to each participant after they had stated the changes that they wanted to make to their behaviour and ‘what they would like to let go of’.
Connection to country, including via program delivery on-country, was identified as an important design feature to support cultural connectedness, immersion and healing. Many Aboriginal case management providers and providers of Aboriginal cohort trials work outside, on-country, with participants. This work outside can be intermittent or regular. For example, one Aboriginal case management provider meets participants at an outdoor café, near a river on a regular basis, while the BDAC cohort trial is delivered on-country weekly. In contrast, Camp Jungai was used on an ad-hoc basis by both Aboriginal cohort trial providers and Aboriginal case management providers to enrich perpetrator interventions for Aboriginal men. Similarly, A Better Way intends to use Gathering Places and cultural sites for program delivery outreach with Aboriginal men. One case-management provider reported using brokerage funding to support on-country participation.
Generally, case management providers in regional areas found it easier to find space to work outside, on-country with participants compared to providers in metropolitan areas. One Aboriginal case management provider in a regional location commented that they are lucky that they could get back to country as much as they do, particularly when comparing their situation to the situation of metropolitan providers.
Elders also played a role in connecting program participants to culture and country, because they were acknowledged and respected community members due to their contribution, cultural integrity and ethical practice. This meant they were in a unique and respected position in the community to relay cultural knowledge:
Elders (especially those who are traditional landowners) have a significant, sacred relationship with the environments where the groups are meeting. Their strong connection to this land permits them to conduct an official Welcome to Country ceremony, show and present historical landmarks and features of the land, and demonstrate how to respect the land in harmonious unity… It can be extremely difficult for one to attain such knowledge, especially if there are no connections to local Aboriginal Elders.
This focus on cultural healing was important for the Aboriginal participants, and enabled them to engage in the content. In one example, a service provider commented that one participant was attending both a mainstream MBCP because it was mandated, and their program because it was culturally safe. They commented that not having a culturally appropriate program for Aboriginal people increases risk to people who experience violence.
5.4.2 Engagement with Elders
A number of cohort trial and case management providers engaged Aboriginal Elders to either guide the development of interventions or to actively participate in the delivery of case management and/or cohort trials.
Engaging Elders in the design phase of cohort trials for Aboriginal people who use violence ensured that cohort trials were appropriate for an Aboriginal cohort. For example, one cohort trial engaged an Elders Advisory Group when deciding the framework to use for the cohort trial, including through direct consultation with the Safe and Together Institute. Elders informed the BDAC trial for the on-country component.
BDAC also included Elders in the delivery of their intervention. They considered having the presence of Elders was at the ‘heart’ of what they do. One of the roles of the Elders was to share their cultural knowledge and artefacts with the group. This led to conversations about different types of trauma and a conversation about how participants had wounded others. Elders were also involved in the closing ceremony for this intervention. Their guidance and physical presence commanded respect from the group and was highly valued by the provider and participants. They considered Elder’s involvement to be vital, and that the work would not be possible without the involvement of these men.
Given the critical role Elders play in the design and delivery of the programs, providers reported it was important they were appropriately compensated for their time, or costs be covered (for example taxi vouchers to provide transport).
5.4.3 Community engagement and referral pathways
Community engagement is paramount in providing an intervention for people who use violence for an Aboriginal cohort, both in case management and the cohort trials. As one case management provider stated – “if we are not seen in the community people will not engage with us” . This provider reported investing considerable energy and time engaging with other ACCOs, men’s groups and the community more generally. However as multiple case-management providers mentioned, this work is not included in KPI measurements or funding allocations.
Community connection was a key mechanism for facilitating referrals. Providers reported it was important for programs to slowly establish a positive reputation in the community in order to attract referrals (predominantly word-of-mouth). An implication is that it may take longer for providers of programs to Aboriginal people to recruit participants if trust and reputation of the program needs to be built first, and evidence of its success visible to community members.
It was also noted that the connection with community could, in certain situations, place pressure on Aboriginal workers who also serve as trusted members of their community. This dual role of worker and community member means they are accountable to the community outside of work hours and could be personally affected if there was an adverse effect of the program. A consequence of this is that it may take more time for a program to become fully operational, as workers need time to familiarise themselves and develop deep trust in the program before they feel comfortable promoting it. This also elevates the responsibility of the worker delivering these programs. These challenges can also contribute to staff burnout and vicarious trauma. Self-care strategies, including support from providers, may therefore be particularly important for Aboriginal workers to prevent burnout and vicarious trauma.
5.4.4 Aboriginal designed and delivered
Case management and cohort trials for Aboriginal people were designed and/or delivered by Aboriginal Community Controlled Organisations and/or workers. This has been necessary for ensuring the cultural appropriateness of the program and for building acceptance and trust (and subsequently uptake) of the program within communities. One mechanism to enable Aboriginal-led program design has been through governance structures. For example, one provider has established a Cultural Advisory Group to provide advice and guidance on cultural practice and knowledge. Further, all case management providers targeting Aboriginal participants are delivered by ACCOs, have an Aboriginal worker or have auspiced an Aboriginal organisation.
5.4.5 Meaningful partnerships
Where partnerships between the ACCO and non-ACCO delivery organisations has occurred, these have taken time to establish, and require mutual trust and respect. This is because the organisations bring different perspectives and knowledge, and working through these differences can take time. When it works, it can be an important enabler of success. For example, both Anglicare and VACCA respectively wrote the submission together, established governance arrangements and held working group meetings together. The different ways of working, and challenges in bringing together two organisations in a short period of time to deliver a program, contributed to the partnership between BDAC and Centre for non-Violence discontinuing.
Co-location enabled creation of meaningful partnerships, recognising it is important supervisory and accountability lines are clearly understood where co-location occurs. VACCA reported that the physical office of Anglicare is welcoming and culturally safe for Aboriginal people. This provided VACCA with the confidence to co-locate an employee within Anglicare. Anglicare also offered to co-locate at VACCA which represented to VACCA a genuine commitment to an equal and respectful partnership. An unintended benefit of this is that it has reportedly helped in building collective knowledge and expertise between Aboriginal and non-Aboriginal services.
Cohort providers reported that while the establishment of these meaningful partnerships may have lengthened the implementation process, it created a trusted and respectful foundation upon which the program has continued to be built.
5.4.6 Time to deliver and implement programs
A common theme was the length of time it takes to appropriately deliver and implement programs for Aboriginal cohorts. As mentioned in Section 5.4.3, cohort trial providers reported it was necessary to establish recognition and trust of the program within the community to aid the flow of referrals; something that takes time. Similarly, as outlined in 5.4.5, meaningful partnerships between ACCO and non-ACCO also take time to establish but are critical for program success. Providers reported there has been an inherent tension between having a 12-month pilot and the need for sufficient time to ensure the programs are culturally safe and create referral pathways. Twelve months is seen as a relatively brief period with an arbitrary end date.
Further, it was reported that an extended length of time for content delivery is important. Anglicare and VACCA’s submission notes that “programs with Aboriginal men are most effective when operating in non-time limited environments”. Similarly, BDAC extended the number of sessions it delivered because it found more time was needed to cover the content.
5.5 Women who use force
One program targeting women who use force was initially funded, with a second program (Futures Free from Violence) subsequently including women who use force into their program. Positive Shift is a perpetrator intervention program for women who use force in the Central Highlands, North East Melbourne and Western Melbourne. The intervention is being delivered by Baptcare in partnership with Berry Street. The +SHIFT program uses a different approach to Men’s Violence programs, as the literature indicates that women’s use of force is guided by different dynamics to men’s.
The feedback provided by these participants was consistent with the views provided by the LGBTI participants. A majority of women who use violence in intimate relationships are also victims of violence [5]. Considering this, specific approaches are required for this cohort which are sensitive to experiences as a victim, yet also empathise accountability.
5.5.1 Healing from violence/trauma
Baptcare adopted a strengths-based approach to working with women who use force, recognising that most or all participants have past experience of violence. By drawing on systems theory and a feminist framework, the program enabled women to understand what led to their use of violence and the relationship between past trauma and current acts of violence. Many participants discussed how the program helped them to understand their own behaviour, and improve their knowledge of family violence more broadly for example, that it does not pertain only to physical abuse.
It's for women who were at a point in their relationship where there's some type of family violence and they have now lost control of how they would respond to that situation, and respond out of desperation, which in turn, makes them do things that they wouldn't do under normal circumstances.
I saw lot of family violence as a child, and there are things that I do to try to protect myself from those happening, that also is a form of family violence. So like, I did those things because I'd seen so much.
5.5.2 Peer support
Many participants emphasised the importance of feeling a sense of belonging within the group. Having a safe space for women to discuss family violence was appreciated by participants, with many noting that they were not aware of other programs that specifically serviced women. One participant discussed that there is minimal recognition that women can use violence, noting that this limits opportunities for change:
I think having a safe place for women to be able to talk about it is really good, because society thinks that, 'Oh no, only men. Men only do this' but it's not true… it's nice to give girls a chance to change as well.
5.6 Fathers
Most program participants across the cohort and case management trials were fathers. Seventy-four per cent of case management participants were reportedly fathers and of cohort trial participants. One cohort trial was specifically designed for fathers – Aboriginal and non-Aboriginal – and is the focus of this section.
Anglicare and VACCA are trialling the Safe & Together Model which is a flexible community-based intervention program, based on internationally recognised best practise. The model has the intention of finding a better way for fathers who have been using violence to be in their children’s lives. The trial offers tailored responses to the needs of fathers and addresses the underlying drivers of behaviour. There are three phases of the intervention which include:
- engagement and motivation
- assessing underlying drivers and intersecting factors which includes psycho-social-cultural assessment, individualised intervention (one-to-one and face-to-face), case management and referrals, cultural healing and mid-point review
- generativity and looking to the future.
A key feature of the cohort trial for fathers is that it focuses on the whole family unit (including children). Rather than delivering the program in a group with other people who use violence, it is delivered as more of a case management model with each family unit including the children where appropriate. This encourages people who experienced violence to be involved in the program, and they were more involved in support compared to other programs. Some participants indicated they would have appreciated even further engagement with the child.
I wanted to make the best choices… and get the help that not only I needed but that [daughter] needed. And the program provided that
It also means that the family safety contact function is a strong feature of the model, noting that the family safety contact worker is also the case worker for the person using violence (unless the person experiencing violence has a preference otherwise). The service provider reported that this has assisted them having a complete picture of the situation to manage risk.
Sessions for people who used violence were not dissimilar from the other perpetrator intervention programs, apart from having a greater emphasis on parenting skills in the context of family violence. Participants reported that most of their discussions with their case worker centred on how to be a better father, with this being a key focus/goal of the program.
[Case worker] just talks about good parenting, being a role model to your children…like being a protector, and being a good partner.
[A typical session] Basically [involves] talking of what I did for the last week or the last fortnight with the kids, with the children. Was there any hiccups, was there any arguments, how did I react if there was?
The service provider reported that focusing on parenting and children can be an important motivator for engaging program participants.
5.7 Cognitive impairment
Bethany Community Support is providing an intervention program for perpetrators who have a cognitive impairment. In the past, Bethany have found that many perpetrators referred to them via police active referrals present with complexities that influence their use of violence, including an estimate of 20-30% with cognitive impairment. To address this gap in service provision Bethany Community Support engaged a specialist disability practitioner to adapt group work and individual session activities and materials to suit the needs of perpetrators with cognitive impairment.
Peninsula Health’s intervention addresses the needs of male perpetrators of family violence with cognitive impairment primarily due to brain injury. Like Bethany, Peninsula Health has recognised in the past that as many as three to four men in each Men’s Behaviour Change Program group demonstrate low levels of participation and facilitators have questioned whether this may be due to participants’ ability to learn. These needs are addressed through a modified MBCP group as well as one-to-one cognitive behavioural therapy and Good Lives Model case management.
5.7.1 Group design – slow pace and small, closed group
Service providers and people who used violence with cognitive impairment identified that the smaller group size relative to mainstream MBCPs was a beneficial design feature for engaging with the group. A few program participants identified that the group had a smaller number of participants compared to ones they had previously been involved in, and noted that it was difficult for them to integrate in larger groups. Participants felt that the people who were involved in the program were those who would struggle being part of a larger group.
The first group they didn’t do – arrange one on ones as such… this one I’m in now is focused on those perhaps struggling a little bit more. Or perhaps feel uncomfortable in a bigger group. And it’s the kind of guys who perhaps need more mediation and support than the average Joe.
There was this program and a similar one, a bigger group, but they insisted that I do the smaller group because I would get lost in a bigger group being autistic. It's easier for me to associate in a smaller group.
The smaller group size, coupled with the closed group, has reportedly assisted program participants to ‘open up’ more and talk about their violent behaviour. Service providers reported this is because the small closed group means they feel safer to talk about their violent behaviour, and consequently are more engaged in the program itself. Further, the slower pace of the group has been helpful, including because it provides more time for people with language difficulties to formulate their answer.
5.7.2 Using prompts and visuals
Both providers of cohort trials for individuals who use violence with an intellectual disability used ‘prompts’ in their perpetrator interventions. The idea to create theses ‘prompts’ came from subject matter experts in disability. These ‘prompts’ were used to teach participants how to correctly interpret the emotions of others, in particularly their partners. This was done through visually demonstrating the different emotions. Feedback from one of the participant’s partners was that after the first session that utilised ‘prompts’ her partner recognised her emotion correctly as sadness. Previously he had been misinterpreted her emotion for smugness, which had previously escalated his anger.
Participants involved in the cognitive impairment trials reported an emphasis on using visual stimuli, such as pictures and videos, to promote discussions in groups, and that this assisted in their ability to interpret emotions and understand. These groups also appeared to adopt elements of cognitive therapy, such as exploring the links between thoughts, feelings, and behaviours.
They've usually got some pictures on laminated sheet of paper about what's violence, nonviolence, so it's visual. So yeah, we just usually take a card and talk about what we see on that picture… I'm more a visual person so yeah, that photo really helps. It makes sense to me a lot easier.
5.7.3 Workforce intensity and skill-set
An enabler of the program has been having specialists assist in the design and delivery of the program. For example, the Peninsula Health trial was led by psychologists, a neuro-psychologist, while Bethany engaged a disability specialist to design and implement their trial program. This means the programs adopt a more clinical approach. In addition, there is greater resource intensity compared to MBCPs. Facilitators use more visual aids and slow down the pace of the content.
5.7.4 Unintended consequence
One service provider reported that an unexpected consequence of the program has been that it has increased awareness and understanding among facilitators within the mainstream MBCPs around working with people with cognitive impairment. This includes facilitators being more aware of challenges within their group, and how and why participants may present with particular behaviours, all of which has contributed to them being more flexible when running the MBCP.
Additionally, one provider commented on the unanticipated complexity that has arisen in some cases whereby a client carer is seen to be contributing to the cycle of abuse. Case workers had been noticing controlling-type behaviours from some carers, which they assessed to be a factor in the dysfunctional relationship dynamic. This included examples where a carer enforced strict daily regimes on the client. The provider indicated they have been in contact with a disability peak body in order to determine how to address this issue.
[1] Department of Health and Human Services, Call for Funding Submission, 2018.
[2] While data was collected for 710 people who use violence in case management and 159 in cohort trials, as the data is not complete for every individual, the sample underlying these different ratios vary
[3] An integrated service response includes a multi-faceted approach to responding to the complex needs of people who use violence and people who experience violence. This includes assessment, co-ordinated case planning and management, co-ordinated service responses and providing wrap-around support and specialised services to meet the risks and needs of the family.
[4] Bendigo and District Aboriginal Co-operative. Submission to DHHS Call for Funding Submission, 2018.
[5] Baptcare new perpetrator interventions funding submission: ‘Positive Shift - Women who use violence in intimate relationships – intervention trial’
Early client achievements
Key findings
- Providers of cohort trials and case management reported that participants have been demonstrating high levels of engagement compared with their experience facilitating mainstream programs.
- Some participants have reportedly begun to understand the effect that their violence had on others and began to take responsibility for their behaviour.
- Participants acknowledged that they would need to continue to work on implementing these strategies in order for them to become ‘learned behaviours’.
- The programs are contributing to a greater level of risk management of people who use violence, particularly those with complex needs.
- People who experience violence reported that the support they received had helped them to feel less isolated, and a number indicated their feelings of safety had improved.
6.1 Introduction
The data collection process identified some early client achievements as a result of participating in the cohort trials and case management. The achievements identified are limited in breadth and nature due to the short amount of time that has passed since the commencement of the programs.
Early achievements of cohort trials and perpetrator case management are explored in this section in respect to three key areas:
- attendance, retention and engagement of people who use violence in perpetrator intervention
- people who use violence’s insight into their violent behaviour
- the behaviour change strategies of people who use violence
- outcomes for people who experience violence.
6.1.1 Data collection limitations
This section predominantly draws on data collected from the interviews with people who experience violence and people who use violence, and the data collection tool.
The data collection tool required providers to ask people who use violence and people who experience violence a short series of questions related to their perceptions of and current use of violence [1] at the commencement and exit of the program.
Of the data returned via the data collection tool, outcome data was only provided for a subset of individuals [2], which was particularly small for people who experience violence. Therefore, these results only represent a small sample of participants involved in the programs. Additionally, while the results of the people who use violence and people who experience violence are reported together, the responses for each group were aggregated, and therefore should not be interpreted as linked between partners or family members.
Secondly, the outcomes (entry) data is intended to be self-reported by people who experience violence and people who use violence. Training was provided by FSV to providers to assist them in incorporating asking people who use violence and people who experience violence these questions into their practice. Providers were advised that in circumstances where the participant was not available to be asked the question directly, they could use their own judgement to respond to the outcome question. There is likely to be variation between a participant’s perception of their own insights or behaviour, compared with the provider’s, particularly noting that a number of participants were either near completion or had completed the program at the point of data collection, and were asked to report retrospectively. One example was given from a provider regarding this issue, whereby one participant believed that he was insightful about his behaviour at the start of the program, however he would have been assessed as having no insight.
6.2 Attendance, retention and engagement
The cohort trials and case management were funded and designed to increase the number and range of people who use violence who could engage with perpetrator intervention. Whilst availability of programs is the first, and important, step to prevention of family violence through perpetrator interventions, continued engagement and retention of participants in the programs is crucial to their success.
6.2.1 Attendance and retention
With reference to the demographic data from the data collection tool, reported in Chapter 5, there are positive signs that a greater diversity of people are now able to access perpetrator interventions. This is also supported by anecdotal evidence from providers. For example, case management providers are now working with people who use violence who had previously attempted to participate in mainstream MBCP but found it unsuitable for their circumstances or were excluded by providers. Furthermore, many participants disclosed in interviews for this evaluation that they were receiving support for the first time. The data collection tool showed that only 13% of people who use violence undertaking a cohort trial had previously attended a MBCP [3]. For case management, 11% of people had previously attended a MBCP [4].
A number of cohort trial providers noticed that retention rates were higher in cohort trials compared to mainstream MBCP. They reported that this was a consequence of increased resources being available to achieve more regular contact with participants, particularly participants who can typically be challenging to engage with. They also noticed that when men could not attend a session they would text in advance and let the facilitator know the reason, which was uncommon in their experience. The provider of the women who use force cohort trial found that women were continuing to attend the group when they were experiencing crises in their lives and furthermore women in crisis were arriving early to the sessions.
The design features outlined in Chapter 4 contributed to the strong retention, including closed rather than open groups, and the creation of strong relationships between facilitators, participants and group members.
Analysis of the data from the data collection tool shows that the average program participation rate was 60% for case management and 72% for the cohort trials. This is not an indication of overall program completion, but just indicates the average proportion of available sessions that were attended, at the time of data collection.
6.2.2 Engagement
A number of providers reported that participants have been demonstrating high levels of engagement compared with their experience facilitating mainstream MBCPs. This was evident not just through increased attendance levels, but by participants willingness to participate in the group activities, and being relaxed and ‘opening up’ in sessions.
Key enablers of positive engagement with the program included:
- Personal development - including the desire for self-understanding and emotional regulation. A number of participants spoke of wanting to be a ‘better person’.
- Family reasons – the desire to improve their relationships and communication with family, including their children or a partner or ex-partner. Some participants mentioned that they did not want their children to emulate their own behaviours.
- External motivators – a number of participants indicated that they perceived their involvement in the program would reflect positively on them, which would assist with legal proceedings or child custody negotiations.
Some identified barriers to engagement included:
- the negative stigma associated with perpetrator interventions
- a lack of preparedness to change behaviour or take responsibility for violent actions
- a lack of awareness about the program and how it could help them, resulting in uncertainty and trepidation to become involved
- the time commitment of the program, and the inability to balance participation with competing demands such as work, family, and for some, legal cases
- dissociating from person who uses violence – a unique barrier for people who experience violence related to having an ongoing association with the person who uses violence.
- if the person was mandated to attend, this sometimes reduced their willingness to engage, as they weren’t yet at a point where they had acknowledged their violent behaviour or the need to address it.
In some cases, there were concerns raised about the intention behind the motivation to engage in the programs. This related to whether the person was participating in the program in order to change their behaviour, reduce their violence, and improve their relationships, or whether there was a motive associated with wishing to be viewed positively by others.
As mentioned in Chapter 5, for CALD cohorts there is still a barrier to understanding what constitutes family violence, and this contributes to a lack of readiness to change behaviour. There was anecdotal evidence that this cohort were motivated to participate so that they could remain with their family, and reduce their contact with the justice system.
A lot of migrants that come from the country – they don’t know their own – what do you call it? The rules of the country. They’re new. They don’t even know that it’s a crime, if they’ve done something wrong here, you know? And you could have a heated argument and that could end up in court. A lot of these – it’s not, like, physical violence, or things like that. You’ve had an argument, or something like that, and that’s considered family violence, you know?
In the context of the Aboriginal cohort, connection to country and community involvement has been a significant factor in providing a culturally appropriate and engaging service for this cohort, as discussed in Chapter 5. However this close connection to community has raised concerns in some instances where participants may perceive their involvement in the program as a means of developing a positive profile in the community, especially through association with the local case workers who are well respected community members. This shows that there is a need to address motivation for change as part of the program, framed in the context of firstly addressing violent behaviours, with positive community connections as a secondary benefit.
Another bonus too, probably indirectly, is living here in [Location], for me the type of person [Case Worker 1] is and with what I'm doing and the situation I'm in, I can be anywhere and I have people say, "Hey, how are ya?" and I say, "Oh hey, how you going?" I don't know who it is. Or so and so. But they know who I am and they know what I've been doing, know where I'm going to. So actually outside of the group the people that I've met that are in other organisations that are happy to say "Hi". And that's awesome.
6.2.2.1 Exit planning
One issue identified with engagement has been around exit planning and the role of ongoing engagement and support for people who use violence. There has not been a clearly communicated and consistent approach to exit planning among providers. In many situations people who used violence reported they had not had a conversation with their case manager or group facilitator regarding when their support would end. This has meant people who use violence themselves were not always clear on the end of their engagement, and what they could do if they felt they required more support.
In contrast, there were other examples where providers communicated to people who use violence that while official support had been finalised, they could get back in touch with the provider. This has assisted people who use violence become more aware of the supports available to them, so they know where to go for help if needed. Some Aboriginal providers have established yarning groups as a means of providing a less intensive ongoing support to people who use violence.
It's just good knowing I can ask and I can receive, you know what I mean? Normally you'd be sitting around and you wouldn't know what to do. You wouldn't know how to find people to help.
6.3 Insight
Acknowledging the current short-term analysis of the programs, increased insight into their violent behaviour is an early indicator of the change process for people who use violence. It is common that participants commence perpetrator intervention programs with limited acknowledgement of responsibility for their actions. They may claim that their behaviour was the fault of the people around them, and that they were the victim in their situation. However, anecdotal evidence shows that through program education and activities, some participants began to understand the effect that their violence had on others and began to take responsibility for their behaviour.
6.3.1 Awareness and understanding of family violence
Several service providers, notably the two trials working with Aboriginal cohorts, reported they focused on increasing understanding and knowledge of different types of family violence with people who use violence. Anglicare reported they specifically ask the father to name the type of violence they use, to increase understanding that their behaviour constitutes violence. Similarly, BDAC reported that after several weeks of the program they dive deeply into understanding what family violence is, and the behaviours that comprise family violence. They emphasise that family violence is not just physical, but also emotional, cultural, financial and social. In this way, they reported it broadens people who use violence’s understanding of their controlling behaviour.
This work appears to have had some effect on people who use violence recognising that their behaviours constituted abuse. This change in understanding was most prevalent among participants who were previously unaware that non-physical actions could be violent, such as yelling or emotional abuse.
I’ve always been aware of family and domestic violence. It’s always been on my radar. I just never knew the intricacies of it. I never knew how small these little things are that we do that contributes to being a part of the violence realm. So, I think it’s broadened my knowledge of what the violence realm is.
Increased understanding of what constitutes family violence was particularly apparent among those from the InTouch trial. People who used violence seemed to demonstrate greater understanding of what behaviour was family violence, however this was often couched in terms of the justice system and what was legal versus illegal. In contrast, the people who experienced violence from this trial did have an understanding that the behaviour was family violence, and used this language more commonly than the people who used violence.
No, I used to stop my wife “Don’t go there. Don’t go there. Don’t meet your friend. Don’t meet this friend.” Like this, yeah. I used to stop but not anymore because in group session they teach us you can’t stop legally, it’s violence. Even this is violence.
Some participants also indicated that the perpetrator intervention helped them to identify that they were, or had been, involved in a family violence situation. Interventions helped them to gain a deeper understanding of the dynamics involved in family violence, including its pervasiveness across all population groups.
Once you start the course is that you understand that family violence is not solely for one age group or one nationality, it can affect anyone of all different nationalities, cultures, ages, sexes, et cetera.
This increased awareness was also experienced by people who experience violence, many of whom had previously excused or minimised the abuse. Those interviewed reported that the family safety contact worker had helped them to acknowledge that family violence had occurred, and that they were not responsible for the violence they had experienced.
And my understanding of – more of just what family violence is. I think initially I didn’t even know that half the stuff that was going on in my life was down to family violence. I thought it was just oh, you know, part of a relationship. But the more I look back, the more I go… Jesus Christ, how long did I put myself through shit?
There were examples where the increased knowledge appeared to have equipped the person who used violence to use this knowledge to perpetrate violence. For example, they used language such as reporting they were ‘anxious’ to describe and justify their violent behaviour.
He didn’t have any insights, he didn’t have any acknowledgement, there was no apologies, there was no nothing. All he learnt from the men’s behaviour change program was that, ‘Oh, it’s my anxiety, that’s why I behave like that.’ …And he came, and he’s like, ‘Oh, I’ve had this revelation. I behave like that because I was anxious.’ That’s always been his excuse, that his anxiety has been a massive control mechanism in our relationship.
6.3.2 Understanding the impact of behaviour on others
Perpetrator interventions helped people who use violence gain insight into their behaviour through providing education on the impact of family violence. Gaining an awareness and understanding of other people’s perspectives of their behaviour was reported to be a key learning from participation in the programs. Some participants stated that they previously had not given much thought to how their actions would be perceived by others. For example, a few participants stated that they were unaware that raising their voice, or their mere physical presence could be intimidating for other people.
I'm 6'4”, I'm a big guy, and it would be scary for her in a sense of things, and I also didn't really realise that that much, but maybe that was probably the fact being that the size of me, and my voice gets quite loud, I can get very loud, would be terrifying to someone. I didn't know until [Case Worker] pointed it out to me.
I can be pretty intimidating if I need to be… what I’m finding out is that psychological side of things can even have a bigger impact on people. I’ve looked at people and seen that they’ve been scared of me, and I don’t like that...
I think I’ve got more compassion for other people now. I’ve got more understanding of other people, how they would feel if I was acting in an angry way, so to speak. He’s done well, he pulled me out of my shoes and put me in someone else’s shoes. He done a good job, he really did.
In some cases, this also extended to understanding the impact that family violence has on children. As noted above, some participants indicated that becoming a better role model for their children was a key motivator for their involvement.
I have two boys … a 15 year old and an 11 year old - it's really important for me to show them how to treat women… even being accountable for what I say to them… those little things that we might not think [have] an impact on our children because they're just kids, when they're things that they take into their future and their own personal experiences… It's changing a generation.
I do think he’s more aware of how his behaviour impacts particularly [Child], and obviously me, but particularly [Child]…so definitely I think it’s made him more aware of the impact of his behaviours. And we’ve managed to get to a point where he’s – where we’re going to have a financial settlement, which I never thought we’d get to. I do think I’ve definitely seen a change. It’s definitely not perfect or – and I anticipate there’s probably still going to be some difficult times in the future, but I have 100% seen some change.
This is supported by findings from the outcomes measures included within the data collection tool, where there was a higher proportion of people strongly agreeing that the person who uses violence understood the impact of their behaviour on others at exit compared to entry. This was the same for people who experience violence and people who use violence (see Appendix E). While people who used violence had higher proportions of people agreeing or strongly agreeing compared to people who experience violence, there was nonetheless a positive shift in the perception from both parties. There were more people who experienced violence who agreed or strongly agreed that the person who uses violence understood the impact of their behaviour at exit for the cohort trials compared to the case management.
Between 14% and 26% of people who experience violence reported positive changes in the person who uses’ violence understanding of the impact of their behaviour at exit compared to entry (see Chart 6.1 and Chart 6.2). This was similar across both the cohort trials and case management. A higher proportion of people who experience violence reported negative changes in the case management programs compared to the cohort trials. In the case management trials, there was a similar proportion of people who experience violence reporting negative changes as there were positive changes. This may reflect the intensive nature of the cohort trials, which included both group learning to address behaviour and a case management component. In addition, it reflects the long-term nature of behaviour change.
Chart 6.1 Cohort trial, proportion of people who report changes in outcomes, people who experience violence
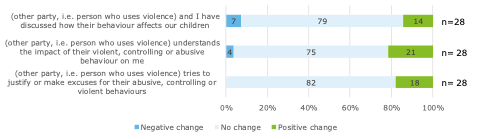
Chart 6.2 Case management, proportion of people who report changes in outcomes, people who experience violence
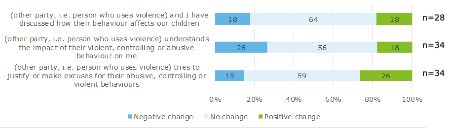
For the InTouch trial, participants focused on their increased knowledge of what constituted family violence, yet this had not necessarily translated into understanding the impact it had on others. As mentioned in 6.3.1, participants’ understanding and motivation for change was framed in the context of the justice system and keeping their family unit together, rather than because of the impact it had on their family. This is not a reflection of the program, but perhaps the level of readiness for change among participants, and a lower level of baseline knowledge regarding family violence. This reinforces the need to work with these communities.
A lot of migrants that come the country – they don’t know their own…The rules of the country. They’re new. They don’t even know that it’s a crime, if they’ve done something wrong here, you know? And you could have a heated argument and that could end up in court. A lot of these – it’s not, like, physical violence, or things like that. You’ve had an argument, or something like that, and that’s considered family violence, you know?
6.3.3 Taking responsibility for behaviour
There is mixed evidence on the extent to which people who use violence are taking responsibility for their behaviour, with many examples of this occurring while other examples of victim blaming persist. This is to be expected given the short-term nature of the programs, compared to the long-term process of behaviour change. This is discussed more in Section 6.4.
Through participation in the cohort trials and case management, some participants began to reflect on the negativity of their past behaviour. Many participants indicated that being part of perpetrator intervention allowed them to reflect on their past behaviour and actions, and recognise that it was wrong. Some participants talked of realising their behaviour was not ‘normal’, and others indicated they felt ‘ashamed’ or ‘embarrassed’ of their actions.
I didn’t realise how bad I was. I can’t apologise enough for it… [provider] made me realise how off track you are. You think it’s normal. I don’t know. I think it’s not normal going off at bank managers or going off at Centrelink or going off at your best mate… beating the hell out of your kids… It’s not normal, you don’t do that.
You feel ashamed of what you have done. You just look back and say ‘God, what did I do?’ I’m fully embarrassed of what happened...
The program, to me, is based on acknowledging your behaviour, acknowledging your part in the behaviour, and acknowledging your wrongdoing. Accountability is a big one. You’ve got to be accountable in order to change your behaviour and move forward.
Many participants talked of recognising a need to take accountability for their actions. Some participants noted that they were ultimately responsible for how they responded in certain situations. Participants stated they learned not to ‘minimise’ or ‘smoke screen’ their abusive behaviour.
I find myself explaining why things happen. But you’re not there to explain why something’s happened. You’re there to accept full responsibility for why things have happened. You’re not here to blame other people.
I’m reminded of the severity of the incident that I was involved in. As I didn’t believe it was so severe, but it didn’t matter… from severity of say 1 to very severe at 100 or extremely severe. It didn’t matter. I might have thought that I was probably around about 15. It doesn’t matter if it’s 15 or it’s 100, it’s the same thing.
While these examples are promising, data from the data collection tool and other interviews suggest there are still a large proportion of people participating in the programs who are not yet taking responsibility for their behaviour. A low proportion of people who experience violence strongly agreed or agreed that the person who uses violence does not justify their behaviour across both the cohort trial and case management (see Table 6.3 and Table 6.4). There were also continued examples of victim blaming and people who use violence not taking responsibility for their behaviour. This is discussed in more detail in Section 6.6. This does not mean the programs are ineffective, but rather these programs are needed to reinforce learnings over a longer time period to reflect the long-term nature of behaviour change. This is discussed more in Section 6.4.
6.4 Behaviour change strategies
Despite the early stage of implementation of the cohort trials and case management, there were reports that some participants were beginning to apply strategies in order to change their behaviour. This included examples given by service providers working with the participants, and self-reported behaviour change by participants themselves.
The main strategies used by people who use violence to subdue their behaviour included regulating their emotions, or removing themselves from a situation.
Learning how to regulate emotions was a key driver for participant behaviour change. Participants usually associated their change in behaviour with an increased ability to regulate anger, or by taking time to think before reacting. Participants talked of being calmer as a result of applying their learnings from the program.
I’m a completely different person now. I would just get angry like that and lose temper. But now I don’t know, I don’t know what happened to be completely honest. It just gone… yes, you are human, you get angry, but the extreme of that angriness is not that high. You know what I mean? It’s before… I think I was just sort of an animal or something... I’m sorry to say this...
Some participants mentioned that they learned to recognise when they were feeling a certain way (e.g. physical changes in their body as a result of anger). By regulating their emotions, they could lessen their propensity for violence. They also learned to separate actions from their emotions, for example, noting that whilst it might be normal to feel anger, it was important for them to be mindful of their behavioural response.
Usually my body starts shaking, I start sweating, I start pacing, my heart feels like I've got two hearts, like it's double beating or something. Yeah I just usually want to hurt the person really bad. But if something usually happens now it's just like I think about my future. I stop and actually realise well if I do this, if I act in this matter, then the outcome is going to be me in prison.
Well the strategies, like even just focusing on regulating my own emotions. Like I’m sitting there angry. It’s okay to feel the anger but it’s not okay to act out on it. So those sorts of things. It’s okay to feel sad but it’s still not okay to hit someone because you’re sad… how to feel your emotions in a healthy way and a safe way.
Another common strategy was to remove themselves from a potentially volatile situation. For example, participants would take time out to compose themselves whenever they felt upset or angry. This involved ‘walking away’ to find a quiet place, meditate, or distract themselves with physical exercise.
Strategies, is simple; if you're frustrated, or you're angry, stay away from the grog, stay away from anything that might stir it up, stay away from people, stay away from the person who's made you frustrated… he suggested to get a bit of paper and write down all this stuff on the bit of paper, and write it all down, and then screw it up and throw it out… very kind of handy – which really worked for me.
The meditation… That's been particularly helpful because I've been able to use it at home to relax from work, and sleep better.
Anecdotally, some providers commented on the potentially negative impact this can have on people who experience violence if they are not emotionally prepared for these changes in their partner, even when this is a reduction in violence. There may be cases where ‘abnormal’ behaviours on the part of the person who uses violence may cause the person who experiences violence to become ‘on-edge’ about what to expect, particularly if their partner typically presents with unpredictable behaviour that results in violence. One example given was when a person who uses violence chooses to ‘walk away’ from a situation, the person who experiences violence may perceive this as abandonment rather than a de-escalation strategy. This demonstrates the importance of the family safety contact worker being able to manage expectations with the person who experiences violence, and communicate potential changes in the behaviour of the person who uses violence.
The below case study, provided by a cohort trial provider, demonstrates one participant’s change in behaviour.
Case study
Roger*was referred to the cohort trial from another program. Roger’s ex-wife Nancy and daughter Belinda were engaged with the other program. Nancy reported that during their relationship Roger would be derogatory towards her, stating she was “useless” with money and criticised her for the housework and her parenting. Roger also had a history of restricting Nancy’s access to money during their relationship and was now withholding child support post-separation. Roger had refused to contribute to rent payments following their separation. The reported incident which led to the IVO was when Roger made a threat to his wife to “watch your back”.
During the initial cohort trial meeting with Roger, it was apparent that he had very limited insight into his behaviour. Roger was blaming Nancy and did not demonstrate accountability for his behaviour. He also did not demonstrate that he understood the impact that his behaviour had on Belinda. Roger advised that he understood the purpose of the program, but was unsure why he would be referred given he did not believe he was abusive in any way. Despite Roger being dismissive of his behaviour, he agreed to continue to attend sessions. The sessions focused on concepts of being a father, roles within the family, family violence behaviours, making positive parenting choices and goal setting. Roger struggled to keep a focus on Belinda and would frequently try to divert the topic of discussion.
During the program, there was a noticeable shift in Roger’s behaviour. Roger described that his communication with Nancy was now “friendly for Belinda’s sake” and that he was making a conscious effort to speak more positively about Nancy when Belinda was present. Roger was pleased that he has now been able to ensure his focus remains on strengthening his relationship with his daughter.
Nancy also provided feedback that she was pleasantly surprised at the improvement in Roger’s communication with her. Nancy was pleased that recently Roger had agreed to change access arrangements during the school holidays to ensure Belinda was able to take a holiday to Queensland with Nancy. Also Roger had paid all the required child support and had also paid for Belinda’s school jumpers and Scout camp. Nancy also said “He seems to be making a genuine effort with his daughter”.
The cohort trial also spoke with Belinda who provided positive feedback. Belinda was very excited to talk about the rice and vegetable dish that her father had cooked for her over the weekend. Belinda also said “My dad was struggling a lot before, he used to yell at my mum a lot, he would say bad things about my mum all the time, well that was until you came along”.
*Names have been changed
6.4.1 Strategies for lasting change
Being able to achieve lasting behaviour change is pivotal to the long-term success of the cohort trials and case management.
Participants acknowledged that they would need to continue to work on implementing these strategies in order for them to become ‘learned behaviours’, and this particular perpetrator intervention program was a single step in what was a long-term process.
You learn something and it's like riding a bike, you don't forget it and it's always in the back of your head. You cannot do that for six years, but it's going to come back to you. It's something that's always there.
I’ve had to do also my own work outside of the program…. The program gives me the ingredients and then I go home and put it all into action.
Whilst some participants expressed confidence that they would be able to maintain progress even upon conclusion of their intervention, others expressed concern over the long-lasting impact of perpetrator intervention programs on behaviour change outcomes. This reinforces that these programs represent one intervention over a finite time period, when the process for behaviour change can be long and require multiple interventions over an extended period of time. This perspective was reinforced by accounts from people who experience violence, who expressed uncertainty about the lasting impact of behaviour change.
He knows he can't get away with anything while the program's there. And yes, I'm hoping it stays that way but you don't know, do you?
I'm worried about what’s going to happen when the program finishes, because he's going to go back to not really having any support… We’ve got to get through all of that relatively unsupported, I guess. So that's what worries me.
6.4.1.1.1 Readiness to complete program
Whilst some participants stated they accessed other formal supports such as drug and alcohol support, or counselling, or telephone referral services which would continue to be available to them outside the perpetrator intervention program, there was limited evidence that people who use violence had concrete support networks established to transition into post-completion.
Whilst the program end date was clearer for cohort trial participants, and there was therefore greater structure around exit planning, a number of the case management participants indicated that they were in need of ongoing support. Similarly, a number of participants indicated they have developed a reliance on, or attachment to their case worker. Most indicated that they would like to see their case worker for as long as possible, and some were of the belief that they would be able to contact their case worker indefinitely, despite the program only being funded for 20 hours per participant. This places an additional burden on case workers, who in many cases already have significant client caseloads.
I don't think you can put a timeline on it, to be honest. I don't think you can because – I don't think you can put a timeline on it because I grew up with what I've just dished out so in order to me to – I've crossed the line. So I need to keep doing refreshers, so I don't get complacent and fall back into a hole. I believe I need to do this for the rest of my life.
I don’t think there’s anything other than that. I mean otherwise if I will need anything, which I don’t think I will, I will still ask for a hand, because I’ve got a contact for [Case Worker]… I feel free to go back to them at any time.
I would be happy to see [Case Worker] for the rest of my life, you know, to talk about all those things. I don’t feel like stopping it, let’s continue it.
Similarly, people who experienced violence were unclear as to how long they would be receiving support from the family safety contact worker. One person reported that their support had ended, but they had not been informed by the provider. This participant stated they were not made aware until they had tried to contact the provider.
I called her a month or couple months ago and then she just told me that they closed but they didn’t actually tell me they were closing or send me a letter… the closure process was not great. I was quite surprised… it was disappointing.
There are some providers who indicated they have a process of notifying the person who experiences violence when the engagement with the person who uses violence is ending. They then provide support as needed to the person who experiences violence, for periods of up to six months in some cases.
Across the board, however, there is the need for improved communication and planning regarding the end of support process. Participants should be made aware of other avenues for support, and the protocols for continued contact with the case worker. Particularly as there are instances where program staff are feeling overburdened by the intensity of the support they are providing to participants, it is important that there is exit planning to reduce the ongoing reliance on case workers.
However, this also demonstrates that the short-term nature of the program is often at odds with the long-term process for changing behaviour. Recognising that behaviour change can be a process which takes many years, it is unreasonable to expect that the individuals involved in these programs will not need further support to maintain and build on their progress beyond a 10-20 week program. Some participants expressed the need for ‘refresher’ courses or follow-up sessions once the program finished.
Yes, it was too brief. And I voiced that concern to [Facilitator 1] when we were finishing off the Men’s Behaviour Change program they were talking about things saying, 'How has it helped you, and how do you think you can do this and implement it, do you think you can implement it?' And I said, 'No, I know myself and I’ll probably need reminders.' And that was one of the reasons that I ended up seeing a counsellor after the course finished.
It’s like learning to drive a car then all of a sudden you’re on your P plates and you’re driving by yourself. It’s a different feeling then. Where you’ve got that support when you’ve got somebody next to you. And that’s what I felt with the course. I think the course was really good. And I just think that it should have something that has the follow-ups where you can go and continue on.
6.5 Outcomes for people who experience violence
6.5.1 Risk management
Despite the limited timeframes for which to measure notable changes in participant behaviour, providers have commented on the value of the programs in allowing for a greater level of oversight and risk management of these individuals. Particularly for people with complex needs, by engaging them in service provision and case management, this is an effective mechanism for keeping them in view.
This is particularly important in the context of the introduction of the multi-agency risk assessment framework (MARAM). Whilst the practice guide is currently focussed on victims, the information sharing and knowledge of the risk presented by the perpetrator, from the case manager’s perspective, is a vital component of this process. This adds to providing a more comprehensive picture of the risk presented to the victim, in order to increase their safety. When a person who uses violence disengages from service provision, this risk can increase.
6.5.2 Reduced isolation and improved understanding of family violence
Whilst some challenges affecting the uptake of family safety contact support have been outlined in Chapter 4, there were instances where people who experience violence reported positive effects of engagement with this support.
Most people who experience violence reported that the support they received had helped them to feel less isolated. They highlighted that involvement in the program had assisted them to realise that they were not alone in what they were experiencing. Some participants stated that discussions with the family safety contact worker had helped them to see that they were not going ‘crazy’ or ‘insane’, but that their reaction to the violence they experienced was normal.
Having a person available to listen to their story was an important contributor to this positive experience, as it allowed them to feel understood.
[Case Worker]’s really given me the confidence to know that what I’m doing matters and what I’m doing is right. And what he’s doing was wrong.
I was so used to have this fight or flight mode in me… She explained all of that. And it made you realise that you weren’t crazy. It was just normal. And that anyone who’d been in our situation would be dealing with it the same way.
But [provider] set my mind at rest, made me feel like I wasn’t going insane. That what I had been through was not normal but understandable…
This increased understanding of their experience also led some people who experience violence to acknowledge that the violence being perpetrated against them was not their fault, and that it is the person who uses violence who should be taking responsibility for their behaviour.
Yes, it’s kind of hard sometimes to not blame yourself because you shouldn’t have allowed it to happen. But yes, she always implemented to me, remember this is not your doing, it’s his doing. This is him doing it, not you doing it. And she said to me, don’t go thinking that this is your fault, because it’s not, it’s him. It’s him doing it, not you. And she said you’ve done everything you possibly can to protect those kids and yourself. And I just said to her, that’s thanks to you, because I wouldn’t have known otherwise. Like sometimes it does go through me head that, could I have done something different? But I know that it’s nothing I could have done different. He’s got to change not me. And the kids, he’s got to change.
For some people who experience violence, the program has helped them to learn that their situation is in fact one where family violence is being perpetrated. This was particularly the case for people who experience violence who come from a cultural background where these behaviours may be more accepted or tolerated. This realisation allowed these women to feel a greater level of empowerment, and seek support to improve their situation.
It was a wakeup call to me. Not to accept it. That it shouldn’t happen. Because I didn’t think it was domestic violence and they said yes, it is. And I had no idea that the screaming and yelling were domestic violence.
Yeah, and like is it the all culture, is it all the times is the lady should be so work in the home. Is it the men is came from the work and just sit in the couch and the lady should be do everything and the ladies told me in the Australia then [inaudible] yeah, I know he is a work, you are in the home, but they told he's at work, you look after children and you have a lot of shopping, you have a lot of do it, lot of job as well. When he is a come in the home, if he needed something, if you are busy, he can do that by himself as well. Yeah.
6.5.3 Feelings of safety
A number of people who experience violence indicated that their feelings of safety had improved as a result of the family safety contact function. Some felt that this was because they had a point of contact if they were to ever feel unsafe. Others noted that they felt reassured that the person who used violence was in a behaviour change program.
It's more the safety part of it. Telling me what I can do, what – and I know they're there and I know they're a phone call away, I can ring them. That's what I like about it as well. And you feel safer and the kids feel safer because of that. (Person who experiences violence, Cohort Trial)
I definitely do feel safer. I know what to look for. I keep my eyes open. And I feel stronger to actually stand up… to him. To have the strength in myself to go, okay, you can do this. You can get past this and nothing is going to stop you from living the life that you deserve. Not just the one that was on offer. (Person who experiences violence, Case Management)
The below case study provided by a cohort trial provider demonstrates the involvement in the cohort trial of a person who experienced violence, after previously being misidentified as the primary aggressor.
Case study
Miranda is a cisgender, lesbian woman in her late twenties. Miranda was arrested and charged after an incident in which Miranda smashed some of her girlfriend Emma’s property at the home that they shared. As well as criminal charges, this incident resulted in an IVO which obliged Miranda to leave the home, making her homeless.
Miranda was referred to the cohort trial by her criminal defence lawyer who believed that Miranda’s participation in this cohort trial would reflect well on her, and indicate to the magistrate that Miranda was engaged in taking responsibility for the impact of her behaviour.
On entering the cohort trial, Miranda and Emma were engaged as part of the Integrated Service Response model, with separate therapeutic family violence specialists working with each, overseen by the senior practitioner. Miranda expressed high levels of shame and remorse about her behaviour, and anxiety and suicidal ideation.
Through a rigorous assessment process, it became clear that the long-term dynamic of Miranda’s relationship with Emma was one in which Emma used aggression, intimidation, threats and emotional abuse to achieve coercive control over Miranda’s life. Like many victim/survivors of abuse, Miranda had for a long time blamed herself for the abuse she experienced, and had very low self-esteem. Miranda’s arrest and criminal charges, including her interactions with police, her lawyer and the Magistrate, compounded her feelings of self-blame and shame, and encouraged her to see herself as the problem.
Due to a high number of cases like Miranda’s, where a person who experiences violence had been misidentified by their community or the criminal justice system as a person who uses violence, the cohort trial facilitators created a separate group program for people who had used forceful resistance (including physical aggression) against an abusive partner. This group became an invaluable space for mutual support and healing. Emma, who was not yet in a pre-contemplative stage of change, was supported by her practitioner in individual work only.
A vital early stage in the work with Miranda was supporting her to believe that she was someone who deserved to be supported at all. Concurrently, Miranda’s individual case worker supported her with intensive family violence case management. Difficulties with securing housing ultimately drove Miranda to move back in with Emma for a period, during which Miranda’s support worker provided her with intensive, daily support with safety planning, risk management and negotiation. Because Emma was still engaged in individual support with another cohort trial facilitator, the senior facilitator was able to monitor safety through the two facilitators.
Working closely with Miranda, her worker was able to advocate for her to be returned to the social housing register, a process which required agreement from both Emma and from the Department of Health and Human Services. Throughout this period, Miranda was provided with individualised therapeutic support, largely over the phone, focussed on understanding intimate partner violence, recognising warning signs, negotiation, fairness and responsibility.
The data collection tool asked for a self-assessment of the safety of people who experience violence who are engaged in the survey, both at entry and exit from the program. Although it should be noted that data was only collected for a small cohort of people who experience violence, the results indicated that the programs are having a positive effect. This effect was most notable for the cohort trials. Chart 6.3 shows the change in responses between entry and exit. Seventy-five per cent of people who experience violence in the cohort trials indicated an increase in their feeling of safety.
Chart 6.3: People who experience violence – change in feelings of safety between entry and exit
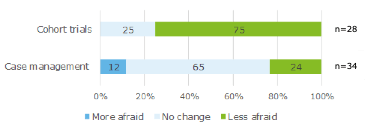
6.6 Limitations of client achievement observations
Despite many participants describing that perpetrator intervention had helped them undergo positive changes, it was evident through discussions that some participants continued to engage in victim blaming, minimising, and denial of abuse. This does not mean participants were not genuine in noting positive outcomes, but instead, highlights the complexity of achieving behaviour change over a short period of time.
Furthermore, both people who use violence and people who experience violence felt that perpetrator intervention was unlikely to be effective for those participants who did not recognise a need to change their behavior, as previously discussed.
I think having programs available is good. I don’t think they’re successful with a certain body of male, people with personality disorders and that sort of thing, like a narcissistic or sociopathic or a borderline, because if people don’t want to change, they’re not going to change. They’ll go because it’s a means to an end for them.
There is evidence to suggest that a number of people who use violence still see themselves as the victim. Some participants emphasised that men were blamed for family violence and that they were not adequately supported compared to women. These participants often talked of services being ‘against’ them.
A unique element of the cohort trials involved recognising the intersection between past trauma and current violent behaviour. Although this was reported by participants to be beneficial, in some instances participants appeared to make reference to their past trauma as a means of distancing themselves from taking responsibility. This highlights the fine balance between recognising comorbid barriers and addressing accountability.
I didn’t believe that I used force against other people and now after doing this course, I realised that I do use force and it’s not specifically my fault why I do use force. It’s also understanding my background and how I was raised and the whole development of it as to why I now use family violence.
Unfortunately, a lot of the people who go into the program have had something used against them… yeah, they make one mistake now and they say, oh, yeah, but they did this 30 years ago so they still must be a bad bloke.
Other negative attitudes were observed when participants reflected on past incidents of violence they had perpetrated. Some participants minimised the seriousness of these incidents or denied that violence had occurred. A common rationalisation used by participants was that they had not been ‘physically violent’ to their partner.
In the end it resulted in a physically violent situation. The short story is I threw a stand that my wife and I were putting together and it hit her, and I didn’t even know it hit her. Not that that’s a justification or an excuse it’s just a fact.
We didn’t get along as well in the long run, because she was very demanding and manipulative with what she wanted. And that just led to constant arguing and abuse and I just always found myself reacting to everything. And she was just completely relentless and making me live a very limited life.
There were also instances where people who use violence engaged in a narrative of victim blaming. This involved rationalising their behaviour by claiming that the victim had ‘asked for it’ or deserved it.
But with [Son’s name], there were times when, oh – I could say years ago, when I had smacked him, that he just didn’t seem to want to learn. Or he – I tried not to – smacking was not my go to, or wasn’t my go-to feeling with his shenanigans. That was only the very last straw. But admittedly I would yell, I would scream.
There were other guys who felt that they were victims, and yet, they were clear abusers. And there were some guys who were there who sort of felt, well, she made me do it. If she hadn’t have made me do it, it wouldn’t have happened.
Drawing on the perspective of the person who experiences violence is often the most reliable indication of whether their partner or ex-partner is demonstrating change. This is because where people who use violence have not taken accountability for their actions, they may not recognise or reveal violent behaviour. They may also inaccurately report positive change in order to demonstrate progress. On the other hand, people who experience violence can provide a more complete picture.
Compared to the feedback given by people who used violence, most people who experienced violence were more cautious in expressing that perpetrator intervention had resulted in any changes. Whilst some people who experience violence noted there had been a certain level of improvement, such as increased communication, they noted there was still ‘a long way to go’ to achieve ongoing change.
There's a lot more work to be done but I can see the changes and he knows the consequences of his actions now, whereas before he didn't.
Furthermore, some participants indicated that they had observed minimal change in the person who had used violence, expressing that it would be very difficult to change their attitudes or behaviour.
I think he will continue to do what he’s doing. I don’t think he’ll ever change, and I don’t think he’ll ever see that there is a need for him to change.
Of concern, some people who experienced violence reported that the people who use violence could apply learnings from perpetrator intervention to become more manipulative and better at hiding their violence.
His awareness of family violence may have changed. He may be a bit more aware of what is family violence, but that has just made him more cunning with how he then uses it to control because if he’s aware that you can’t blackmail and stalk and do all of those things, then he’ll probably just be a bit more covert.
This demonstrates the importance of risk assessment processes, which include the victim perspective, as well as ensuring that program staff and case workers are trained in recognising and responding to collusive behaviour.
[1] Where the person could not be asked in person, the provider used their own judgement.
[2] Refer to limitations of the data collection tool in Chapter 2
[3] There were 20 ‘yes’ responses, 93 ‘no’ responses, and 46 blank or N/A responses
[4] There were 80 ‘yes’ responses, 282 ‘no’ responses, and 348 blank or N/A responses
Implementation - workforce and process
Key findings
- Attracting staff with the appropriate skills and experience in working with people who use violence was a particular challenge for some cohort trial and case management providers.
- A number of providers reported that the initial 12 month funding allocation for the new community-based interventions made implementation challenging. This particularly impacted on staff recruitment and attrition.
- There appears to be some confusion regarding eligibility for the programs, particularly related to their voluntary nature (as opposed to being mandated via courts or Child Protection).
- There are some challenges to effective service coordination across the sector, including a lack of capacity or willingness to work with people who use violence.
- Performance management of the programs needs to be strengthened, to ensure there is accountability for intended outcomes, and consistent data collection and reporting.
- There were examples of underspend among cohort intervention trials, including large proportions relative to the total funding amount.
7.1 Introduction
This chapter examines the activities and processes that were involved in establishing the cohort trials and case management. This includes the following aspects:
- Workforce and training – the ability to recruit and train the workforce required to deliver the programs
- Referrals and service coordination – the processes for generating referrals to the programs, and providing access to other services across the broader service system
- Funding and timelines – an assessment of the funding and timeframes for program delivery.
- Governance and communication – the formal governance mechanisms and communication processes between FSV and providers
7.2 Fidelity of implementation
Fidelity explains the extent to which a program was implemented as it was prescribed in the original protocol or as it was intended by the initiative developers (Proctor, et al. 2010). Fidelity considers adherence to the program protocol, dose/quantity of the program delivered, and quality of the program delivered. Changes to program design and implementation are not in and of themselves negative. Rather, they may reflect appropriate adaptations to a model or program based on the maturity of implementation to reflect learnings.
Case management was generally implemented as intended. Over the course of implementation, the main adaptations made related to increasing use of brokerage (discussed in 4.5.1) as providers became more confident and familiar with how to use brokerage, and flexibility with the sessions provided. Numbers of sessions depended on the needs of the person who used violence. Where someone needed more sessions than the up to 20 allocated per person, this was offset by appropriate underutilisation by other participants (where their needs had been met after fewer than 20 sessions).
Small adaptations were made to the cohort intervention trials as they were rolled out, particularly for the two trials working with Aboriginal clients. BDAC increased the number of sessions to 15 (up from 12), upon recognising that the quantity of content that needed to be covered required more sessions than initially designed. Further, recognising the need for continued support post-program, a fortnightly yarning circle has been established for the exiting participants to continue in post-program. The change made in the Better Ways program is quite different to BDAC, in that it relates to the intake criteria. Previously the criteria was for fathers to have some contact with child or mother. Upon realising this was a barrier to accessing support, particularly for Aboriginal fathers, this intake criteria was relaxed. In both these instances, adaptations made were appropriate iterations of the program design to respond to participant needs. Additionally, the program for people with a cognitive impairment delivered by Bethany was changed to a ‘semi-open’ group whereby participant intake occurred at certain points throughout the program delivery timeframe. This change was made in order to increase the number of participants that could access the program, as there was lower than anticipated program engagement and completion in the first round of program delivery.
In two instances, partnerships between providers have broken-down, representing a change from the model as intended. This involved BDAC and the Centre for Non-Violence, and Drummond Street with On The Line and Merri Health.
The cohort trial program that had the greatest level of change to what had been intended was the program delivered by Drummond Street. This included no longer delivering a telephone support service as had been intended in the model design. This was because, following initial contact with the client cohort, Drummond St deemed that the level of complexity of the issues they were experiencing deemed it inappropriate to undertake a phone response at this point. This program also adapted its program focus in the second year of funding to offer a program for women who use force, as well as embed the program for LGBTI clients within the provider’s ‘Queer Space’ service, which offers an integrated service response.
7.3 Workforce and training
The family violence sector in Victoria is currently undergoing a period of significant reform, with a number of new initiatives and ways of working being developed and implemented (i.e. family violence and child information sharing information sharing scheme, MARAM and the introduction of the Orange Door). There is also a greater level of demand for services than has been experienced by the system ever before. These system-level factors have had direct implications in terms of the ability of service providers to recruit and train case workers to respond to the complex circumstances of many of the clients in the perpetrator case management and cohort trials.
7.3.1 Recruitment
Attracting staff with the appropriate skills and experience in working with people who use violence was a particular challenge for some cohort trial and case management providers. While some providers were able to recruit highly qualified staff without difficulty, others were required to advertise multiple times to attract a suitable candidate.
Challenges with recruitment were largely due to a shortage of qualified staff, particularly in regional areas. The reasons for this include:
- Competition for resources across the sector, which is particularly heightened in rural areas. There are a limited number of case workers and program facilitators who have experience working in the perpetrator context, particularly compared to the victim/survivor case management workforce. This can be partly explained by the limited funding invested in perpetrator programs historically, compared with victim support programs.
- There are a limited number of case workers and program facilitators with specialised experience in working with the identified target cohorts, which was a specific feature of the program design in some cases, e.g. for CALD, Aboriginal and LGBTI groups.
In some cases this was reported to have led to lengthy recruitment processes which contributed to delays to the program start dates. In circumstances where there were no suitably qualified applicants for the role, a culturally appropriate applicant was hired and subsequently trained in working with people who use violence.
Reflecting the broader need to build workforce capacity across the family violence sector, to respond to the increasing demand for services, there is work taking place to address this through the State Government’s Building from Strength: 10-year Industry Plan for Family Violence Prevention and response. This includes a significant funding grant provided to No To Violence to develop more programs and provide training across the sector, including increasing the number of family violence subjects offered at TAFE institutions. These programs will include building capacity in more specific areas of practice, such as working with people who have AOD and Mental Health issues, and Aboriginal clients. Additionally, FSV is funding a select number of places in the Graduate Certificate in Client Assessment and Case Management offered at Swinburne University, which is a specialist course for working with men who use violence.
Case study
One cohort trial provider for Aboriginal and non-Aboriginal fathers was seeking to hire a staff member from the local Aboriginal community. However, there were a number of features that made this role unattractive to a candidate which included:
- the short tenure of the contract
- the 0.6 FTE position
- the abundance of other opportunities available for Aboriginal personnel working in this field.
To overcome the negative aspects of the job description, this cohort trial provider organised a secondment position for the successful applicant, which provided them with job security, while filling the cohort trial role.
Additionally, the timing and length of the trial contributed to recruitment challenges for a number of the providers. Delays to the initial release of funding for the programs resulted in providers recruiting for staff in late 2018 or early 2019 with short contract tenure. This was exacerbated by the uncertainty of further funding beyond June 2019, which led to staff attrition at some service providers due to job insecurity. There were some instances where this had flow on impacts for clients, particularly where a number of the program staff left towards the end of the program. Clients said in interviews that they were disappointed to lose the relationship they had built with their case worker.
7.3.2 Training
Providers of both case management and cohort trials invested time and funding into training staff. This has predominantly been done out of necessity to ensure staff were appropriately qualified to be working with people who use violence.
7.3.2.1 Cohort trial training
There is one short course offered in Victoria that qualifies workers to facilitate intervention groups for people who use violence. This course is run by No To Violence. It is a two-day course designed to support community sector workers with clients who use male family violence. Given the time commitment required to complete this course, it is a significant investment for staff and service providers.
In addition to accessing the external training, a number of cohort trial providers delivered additional training specific to their delivery model, or contacted external trainers for this purpose. Two cohort trial providers flew experts in their chosen model from the United States to deliver training to program delivery staff. These experts were specialised in the ‘Vista’ model and the ‘Keeping families together’ model. Following this initial training, these experts where then kept engaged throughout the delivery of the program, including providing supervision support to on the ground staff in some cases. Another service provider paid external consultants to provide training and supervision.
Individual cohort trial providers also provided internal training for recruited staff, such as orientation programs and trauma informed approach training.
7.3.2.2 Case management training
Specific training in individual case management models for people who use violence appear to be more limited, and a number of providers expressed a need for the development of more materials in this space. It was mentioned that Relationships Australia have developed an internal training program which would be beneficial for other case management providers to have access to. Another provider suggested that extra training could be provided by DHHS. Furthermore, one case management provider mentioned that they were currently in the process of setting up a Community of Practice of people working with people who use violence, in order to share learnings across the sector.
Although the investment in staff training has been made by individual providers, it will have a broader impact on sector’s capability to deliver interventions for people who use violence. A larger impact of these trials on the broader family violence system in Victoria is that more case workers are being upskilled in working with these cohorts. This is increasing workforce capacity and capability in the system, and setting the ground work for this type of service to expand.
7.4 Referrals and service coordination
7.4.1 Referrals
Both cohort trial providers and case management providers received referrals from a variety of sources. The most common sources of referrals, as reported via the data collection tool were via L17s for case management and from courts for the cohort trials. The referrals sources are shown in Chart 7.1.
Chart 7.1 Referral sources
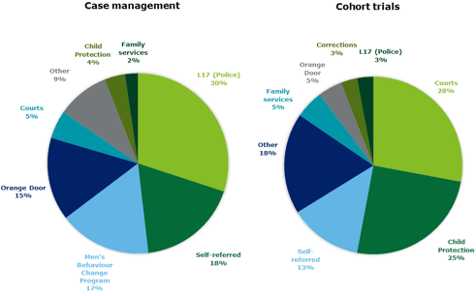
7.4.1.1 Third party referrals
Unexpectedly, a high number of referrals to the cohort trials came from the courts and Child Protection. Unlike in the justice context, participation in the community-based trial programs is voluntary, and therefore an individual cannot technically be mandated to attend via a court order. It was however reported by a number of providers that Magistrates were recommending attendance at a MBCP as part of a FVIO, which resulted in either direct or indirect referral to a cohort trial or case management. This then led to a perception that clients were ‘mandated’ to attend in order to meet the requirements of their FVIO.
The provider delivering to CALD cohorts specifically engaged with the Magistrate at the court in their area, in order to generate awareness for their program and request referrals for people who were on a FVIO. This was to ensure these men would receive a culturally appropriate intervention. Subsequently, 30 of the 48 people who use violence presented in the data collection tool for this program had been referred via the court.
It was clear from interviews with people who use violence that they were not always aware of the difference between voluntary and mandated attendance when referred from courts and Child Protection. Some participants indicated that the program was recommended to them by a third party, e.g. a DHHS case worker or their lawyer, however they acknowledged that involvement in the program was ultimately their choice.
I wasn’t told by anybody to go there. I voluntarily accepted what [the provider was] saying when I rung that number, and I said okay, well yeah, that seems like I might need that sort of guidance… I didn’t get forced to do it.
With a lot of the programs like that, a lot of the people - that's the first thing I say: "I'm forced to do it, either by law or DHS or the courts or whatever." The way I see it, you might be recommended by a court to do a program, but no-one's forcing you to do it. It's up to you to show up… no one is making you stay.
Other participants talked of being ‘required’ to participate, or being ‘ordered’ or ‘told’ to participate in the program. This was particularly evident when the program was recommended to participants involved in legal proceedings. This type of referral is considered to be “service mandated”, despite the fact the individual is not technically mandated to attend.
I’ve just come out of like a court case for like drug use and breaches of intervention orders, so then as part of that been told I had to do this men’s behaviour change program…It was a compulsory requirement.
It was an agreement through Family Court, Federal Court to do that… they asked me just to do a men's behavioural change [program]…It was basically a negotiation between two lawyers, and they asked me to do something...
Providers commented that where a person was ‘service mandated’ they tended to be more resistant initially to participating in the service, as they had not made a choice to be there. Additionally, the engagement of those who are ‘socially mandated’ can depend on the status of their relationship with the person who experiences violence, and whether they believe reconciliation is possible. Despite this, providers reported that where they persisted in building the relationship and trust with these individuals, instead of ‘giving up’ on them, there were instances where they noticed a shift in thinking, and engagement became more genuine. This demonstrates a shift from pre-contemplative to contemplative engagement.
Case study
An Aboriginal person was reportedly ‘mandated’ to attend the cohort trial. They were a respondent to an IVO, and if breached this would have serious implications for their work in the community. During their participation in the cohort trial, the service provider noticed significant progress. This progress included the cessation of text message contact with the partner who implemented the IVO, and beginning to prioritise self-care (which is something they had never previously done). When they were required to go back to court they took a letter of support from the cohort trial provider. This resulted in a non-conviction in court. They were able to avoid the IVO having an impact on their work in the future.
FSV is reportedly undertaking communication with referral agencies as well as the Department of Justice and Community Safety in order to clarify the voluntary nature of the programs, and to provide further guidance on the conditions for referrals and participation in the programs. This is required in order to ensure there is a consistent process for accepting referrals across all the programs. This also has implications for the interface with the justice-based programs, and the consistency of the referral pathways across the two sets of programs. The complexity of the perpetrator cohort, and the large number of referrals from the justice sector, means that it is rarely a straightforward decision that an individual would be purely ‘community-based’. Interaction with the courts and Child Protection is going to be a factor in a significant number of cases, and therefore should not be a factor which limits their eligibility to participate in a program. There is an opportunity to streamline the referral process across the community and justice sectors, so that people who use violence are able to access the most appropriate program for their individual circumstance, regardless of the referral source.
7.4.1.2 Self-referrals
There are a substantial number of self-referrals being reported via the data collection tool. When this was discussed with providers, both cohort trial providers and case management providers indicated that it is rare for an individual to refer themselves as a means of self-motivation to change their behaviour. Conversely, when a person does refer themselves, it is most often the case that there is an external motivation, such as pressure from a family member or lawyer, as discussed in Section 6.2. Interviews with clients indicated that often these self-referrals were made following an incident of violence. This type of referral is considered to be ‘socially mandated’ – that is that there is an acknowledgement that their attendance is voluntary, however there is a known consequence, either legally or otherwise, if they do not attend.
You have to make the decision yourself. So after my incident, I put my hand up and I said yes. On this occasion, yes, I was in the wrong. I’m willing to wear what I’ve done. I’m willing to take part in the [Program name]. So I’m now taking part in [Program name]. The facilitator’s name is [Facilitator name].
And I thought, well I’ve lost my partner of six years. I’ve lost my job. I’m like, I need the support. I need the focus on things. I need to get my life into order in order to make everything work. And so I contacted a number of companies. I can’t exactly remember what ones they were. And then they referred me to [Provider], which then [Case Worker] gave me a call back and we eventually had a meeting. And yeah, I asked her to help me with some sort of group in changing my behaviour and everything else. And it went from there.
People who use violence reported that when they self-referred, they searched online for perpetrator programs, and then contacted the provider directly. However, no participants reported being aware of the unique nature of the cohort or case management trials. Rather, awareness was limited to knowing the provider offered a ‘men’s behaviour change’ program.
I went into the program on a voluntary basis. I did not go through a court order which a lot of the men are there in court orders… I found it online and pretty much put my name down to see if I could get some counselling and also see if I could get into a program which would help me with my communication.
7.4.1.3 Intra-organisational referrals
While there were instances where referrals were made directly to the cohort trial or case management program itself, most often referring agencies would make a referral to the organisation more generally, who would then assess the individual as suitable for the specific program. IRIS data shows that “internal from this agency” referrals make up 12% of referrals for the cohort trials and 12% of referrals for case management. This process is important for identifying individual needs which deem the individual suitable for a cohort trial rather than a mainstream MBCP, and assessing the readiness of the referred person for group work or individual case management.
A few people who used violence had prior or ongoing engagement with the provider delivering the program. In such instances, provider staff identified the participant as a suitable candidate for the program. Participants engaged through this approach reported that it was a straightforward process.
It was quite good… I was already doing drug and alcohol with [Provider] and then they wanted me to also do this course… So, by the time I’ve already done them courses and continued on with drug and alcohol, they rang me.
Cohort trial providers that also run services for people who experience violence also referred persons who use violence through these connections.
7.4.1.4 Timeliness of referrals
Stakeholders highlighted that that there is a window of opportunity between violence occurring and service intervention, which maximises the likelihood of engagement. This demonstrates the importance of timely referrals.
Case management providers found that being present at the courts, and therefore having face to face contact with the person who uses violence, was an effective engagement strategy. Providers explained that, in their experience, the point at which someone is required to present at court is the point they have the highest level of motivation to ‘do something’ about their violence.
Another case management provider utilised automated text messages to ensure that timely contact was made with people who use violence following an L17 report. They found that this led to increased responsiveness.
Participants reported that a common way they accessed the intervention was through receiving direct contact from the program provider shortly after the family violence incident. This contact reportedly followed an incident that required police presence. Some participants mentioned that they had received a text message or letter directing them to contact the provider, whereas others recounted that they had received a phone call directly from the provider.
When I have the trouble with the police and the court guys and all that, I didn’t wait long to see the help… The police sent a letter here… The police referred for the – on the letter… to three different places or something like that.
[The police] sent a text message through two days after the incident to say that [Provider] would be contacting me. Then yeah, within a day, I was contacted. I was contacted the same week the incident happened.
There was some confusion expressed by participants who were referred to programs in this way, particularly when compared to participants who had a Child Protection worker or legal representative available to explain the process. Participants noted that they were somewhat unsure as to what the content or purpose of the program was until they were able to meet with provider staff. The need to offer a more comprehensive explanation of the program was highlighted by some participants.
It needs to be a face-to-face meeting for someone to explain that it's okay to be in that room and it's okay to take up that space… Once you talk to the people you go, ‘oh, my god, this is where I need to be’.
After being marched into a police station to do a statement… two days after, a message came through on my phone, which I knew nothing about. I just knew it came from Vic Police, blah, blah, blah... And [there was] a phone number. And I didn’t know what I was supposed to do with it, so thought I’d give it a call.
7.4.1.5 Common barriers to referral
There were a number of barriers to referral raised by providers of the case management and cohort trials. These barriers were sometimes isolated to certain locations or providers, however there were some common themes identified across providers which are outlined below.
Criteria not to work with individuals on bail or on community corrections orders (CCOs)
A common concern of case management providers was that they were unable to accept referrals for people who use violence who were on CCOs or on bail, as the program could not be mandated, and there is no justice sector equivalent. Case management providers saw a need for case management within this group of people where their needs are not being met, for example as preparation for involvement in a group program. As described above, this distinction between mandated and voluntary referrals was not consistent across providers, particularly for the cohort trials. One provider staff member commented:
One of the complications – it is very clearly targeted at voluntary participants. But some might start off as voluntary and become mandated. It’s not something we can easily predict. And if we had a mandated person with cognitive impairment, it would be remiss if we didn’t include them.
Program awareness and understanding
There was reportedly inconsistency across the service system regarding awareness of the new community-based interventions, and an understanding of their intent, which impacted on the number of referrals in some cases. Particularly, there was a lower than anticipated number of referrals from Orange Doors. The Orange Door reform is still in early stages of implementation, with a number of processes still being worked through. An evaluation of the Orange Door implementation is currently underway.
In some regions, it was identified that the Orange Door had little awareness of the cohort trial being delivered in their area. It is possible that this lack of awareness reflects the early stages of implementation of both the pilot programs and the Orange Door. In areas where the organisation had an established relationship with the Orange Door, particularly in geographically smaller regions such as Barwon, this issue was less notable, and referrals from the Orange Door were common.
Misidentification of the primary aggressor
For providers delivering services to women who use force and LGBTI clients, including in the case management context, misidentification of the primary aggressor was sometimes noted as an issue in the referral process. In some cases, it was reported that there was a misidentification in L17s as to the nature of the perpetration of violence, and therefore who is identified as the primary aggressor. This would result in individuals coming into programs being named as the ‘perpetrator’, whereas the assessment process would subsequently identify them as a person who experiences violence. Related to this is a hesitance by some legal services to refer clients to these programs due to the risk of misidentification. Particularly for LGBTI clients, this carries a significant risk of re-traumatisation if there is a history of discrimination and isolation within the service system. Further education is required to prevent misidentification of the primary aggressor, which further persecutes individuals who are experiencing trauma.
7.4.2 System level factors
A secondary objective of the new community-based interventions is to facilitate referrals to other community-based programs, in order to address participant’s needs which may be related to their offending behaviour or impacting on theirs or their family’s lives.
Results from the data collection tool show the proportion of participants referred to other services, the total number of referrals, and the most common referrals. This is summarised in Figure 7.1.
Figure 7.1 Referrals to other services
| Case management | Cohort trials | ||
|---|---|---|---|
|
At least 252 participants were referred to one or more programs 182 not referred, |
There are a total of 401 referrals to other programs |
At least 35 participants were referred to one or more programs 88 not referred, |
There are a total of 61 referrals to other programs |
|
Top 4 most common referrals
|
Top 4 most common referrals
|
Source: Deloitte Access Economics data collection tool
Referrals across each of the cohort groups, for participants in both the cohort trials and case management, were analysed to determine if there were any differences in the nature of the referrals being made. Table 7‑1 presents the top two service system referrals reported for each cohort.
Table 7‑1 Referrals out – cohort specific
|
Cohort |
Top two referral types |
|
Aboriginal and Torres Strait Islander |
|
|
Fathers |
|
|
Women who use force |
|
|
CALD |
|
|
Cognitive Impairment |
|
|
LGBTI |
|
There were a number of considerations providers had to make when referring participants to external community services. These are outlined in the following sections and indicate that further education activities are required to ensure that holistic and equitable access to services can be provided to all individuals in need of assistance.
7.4.2.1 Reluctance to provide services to people who use violence
There was a level of apprehension among some external organisations about providing services to perpetrators of family violence. For example, one provider explained that “the minute you say that you want to refer a man who has used family violence, workers become apprehensive”.
Gender appeared to be a factor in this response. Staff from the trial for women who use force stated that external service providers were accepting of their program, and open to providing other supports to participants. This difference in acceptability of services based on gender was confirmed by the consult with the provider of the LGBTI cohort trial. This provider had noticed that a client’s degree of ‘femininity’ (as perceived by external service providers) affected their ability to be accepted for other service support.
7.4.2.2 Negative experiences with services
The nature of the cohort trials being targeting people typically from a vulnerable background, means that these individuals often have previous experiences of trauma, discrimination, and institutionalisation. This has contributed to mistrust of community services and government agencies in many cases. For example, it was reported that perceived discrimination, and in some cases, past negative experiences with police or ambulance services, meant clients would not call the police or ambulance even when they required their services. When providers of the cohort trials and case management first reach out to these people, it is sometimes the first contact they have had with a service, due to their past experiences and isolation from the system. Before being able to refer them onto other related services, the staff must work with these individuals to build their trust. This means providers are sometimes required to address past failings of the broader service system, creating additional burden on staff.
7.4.2.3 Appropriate services in the context of family violence
Stakeholders raised the importance of using counselling or other services appropriately in the context of family violence. It is important that the individuals working with people who use violence are trained in identifying and avoiding collusion. For this reason, providers were hesitant to refer individuals to external services unless they had a trusted relationship with the provider, or knew that they had experience providing services in the family violence context. It is also important to recognise the context of the person’s entire family unit, and the services that are being provided to their partner or children, to ensure that there is alignment and that a comprehensive risk assessment has been undertaken to understand the level of service required. The recent implementation of the Family Violence Information Sharing initiative will assist in providing this ‘complete picture’ of the context of both the person who uses violence and the person who experiences violence, including the level of risk and associated need.
7.4.2.4 Gaps in available services
A lack of housing services was reported to be the largest gap in the service system for people who use and experience family violence. It was consistently reported by both case management providers and providers of cohort trials that it was extremely difficult to find temporary accommodation for their clients.
An example was provided of one temporary accommodation option for men who use violence in the western suburbs of Melbourne, where police are able to admit them for one night. However, this one service was insufficient to meet demand. Service providers reported that the lack of available accommodation services for people who use violence acts as a disincentive for these individuals to leave the living situation in which they are perpetrating violence.
Supporting this finding was that case management brokerage funding was often spent on accommodation. Case management providers reported that brokerage would pay for three nights of accommodation, however following this, these individuals would often have nowhere else to go, and would return to the family home.
7.4.3 Community outreach
Both case management and cohort trial providers reported to have spent time undertaking outreach and educational work with other service providers and the community, and indicated that this was an important aspect of their work to promote referrals. For some providers this has been a more necessary focus of the work than for others, depending on the referral pathways in the local area. For example, noting some of the unanticipated difficulties generating referrals from the Orange Door in certain regions, providers in these areas have had to undertake a greater level of outreach to account for this.
Each provider came up with their own approach to community education. For example, one case management provider prepared a script on why they offer support and why people who use violence are deserving of a case management service. Another case management provider developed brochures and spoke at community forums about the service they offer.
The effort that providers invested in outreach work appeared to depend on how established they were as a perpetrator intervention provider. For example, one case management provider who had not delivered case management for people who use violence previously explained that they had put a lot of effort into building relationships with potential referral sources. Whereas another case management provider commented that they already had links within the community, and that networking activity had already been established by the time the case manager commenced their role.
Outreach work was particularly important for providers of Aboriginal case management. This is because they needed to establish trust in the communities in which they work. Aboriginal case management providers particularly made an effort to engage with ACCOs. They also spent time attending cultural groups and noted that if people in the community don’t know you, they won’t feel comfortable engaging with you. Similarly, the LGBTI cohort trial provider gained strong traction with the community through putting out fliers and recruiting staff belonging to the community.
7.5 Funding and timelines
7.5.1 Funding timelines
A number of cohort trial providers reported that the initial 12 month funding allocation for the new community-based interventions made implementation challenging. The timeframe created a feeling of ‘being rushed’, as there was a large amount of work to establish the program within the one-year period. These activities included:
- deeveloping the trial
- establishing governance
- recruiting staff
- attracting clients
- data collection.
This challenge was exacerbated by delays to the initial funding availability, which was delivered in late August as opposed to July. This gave staff limited time to train and familiarise themselves with the delivery models prior to working with clients. Additionally, providers of cohort trials for Aboriginal men who use violence found that one year was not enough time to gain trust with the local Aboriginal community.
Providers highlighted that changing violent behaviour is a long-term process, which requires long term intervention. Many service providers commented on the limitations of what outcomes could be expected over a one-year trial timeframe. Providers had observed early signs of change in participants, however they would have liked more certainty regarding funding over a longer time period, in order to establish more robust mechanisms for measuring program success.
As of the date of this report, funding for cohort trial providers has been extended for an additional year, ending 30 June 2020, and funding for case management has been made ongoing except for brokerage funding.
Despite this positive outcome, the significant delays to the funding announcement meant that there were implications for delivery of the programs. The most commonly reported impact was staff leaving due to the uncertainty of ongoing work. Retaining staff during this period of funding uncertainty was a challenge for providers, with one cohort trial indicating they had a large number of staff resignations in the months approaching July 2019. Staff turnover leads to the necessary process of re-training staff and rebuilding trust with the cohort trial community. Providers highlighted the importance of having long term staff for the success of their work.
7.5.2 Funding amount
Five out of seven cohort trial providers underspent their budget in the 2018/19 financial year. Underspend ranged from $64,818 to $509,384. When asked about this in consultation, providers noted that the delays to receiving the initial funding allocation, and the subsequent condensed timeframe in which to implement the programs, was a factor in the inability to acquit all funds.
Without specific funding for these programs, they would cease to operate. This would mean people who use violence from these target cohorts would only have the option of attending mainstream MBCPs which are not always appropriate to their needs.
During the evaluation, it was determined that a number of the case management providers had still not recruited into the case manager role after more than twelve months, which meant that their funding remained unspent, and no clients had been engaged. There was inconsistency in how this was being reported to FSV and the APSS, and therefore at times limited awareness as to the nature and extent of this problem, including where funding remained unused. Additionally, participation in the evaluation has been mixed, despite being a requirement of the provider funding agreements, and there have been no consequences for providers who failed to respond.
7.6 Governance and communications
7.6.1 Provider forums and advisory group
Family Safety Victoria facilitated four governance forums for the new community-based perpetrator inventions and case management. These were:
- perpetrator Interventions Advisory Group –to oversee the implementation of the case management and cohort trials, by reviewing progress, challenges, and improving an understanding of program approaches and strategic implications[3]
- cohort trials provider forums – to guide and oversee the implementation of the seven perpetrator intervention trials, by providing implementation updates and a forum to discuss common challenges [4]
- case management provider forums - to guide and oversee the implementation of the case management, by providing implementation updates and a forum to discuss common challenges[5]
- Aboriginal provider forums – as above, for all providers delivering services to Aboriginal and Torres Strait Islander people who use violence.
These forums are generally considered to be an effective mechanism for FSV to maintain a level of oversight of the programs, communicate with providers, and for providers to give updates regarding their programs. This also has the added benefit of providers being able to share learnings among one another of what is working, and what are common barriers to success. This is particularly important in a context where these programs are a new and innovative initiative within the family violence system, and therefore it is important that there is a mechanism to share experiences, build effective and consistent approaches, and contribute to a community of practice for improving service delivery in this space.
The Perpetrator Interventions Advisory Group includes representatives from across government who are involved in the delivery of services to people who use and experience violence. This forum is an effective mechanism to collaborate and share learnings within and across different sectors, such as Corrections and courts. Subject matter experts from family violence peak bodies are also able to share their expertise in this forum, and contribute to best practice approaches for program development and delivery.
7.6.2 Working relationship between FSV and perpetrator intervention providers
Overall, the relationship between FSV and the providers of the new community-based interventions was considered appropriate. Service providers reported varying levels of communication with FSV, however there was a common view that they could access assistance or information when required.
Although the overall relationship with FSV was appropriate, there were two logistical issues were barriers identified:
- the timing of the funding announcement and release (as mentioned above).
- performance management.
Data collection and monitoring, particularly for pilot programs, is fundamental for accountability and performance management. Now that the programs are past the initial establishment and implementation phase, some providers have begun to prioritise data collection and performance monitoring processes internally within their organisation. While providers are required to report against their individual KPIs and targets to the local APSS, there is not a consistent approach to outcome reporting across the programs. Additionally, a number of service providers reported difficulty installing and using the IRIS software, which was intended to serve the function of recording participant data. A data collection tool was developed as part of this evaluation to overcome this issue. However, with the evaluation concluding in November 2019, a longer-term solution is now required for outcome reporting.
More established processes for provider management are needed, including further clarification with providers of the roles and responsibilities between FSV and the APSS.
[1] Cohort too small to report further
[2] All responses tied. Cohort too small to distinguish ranking
[3] Family Safety Victoria (2018). Terms of Reference - Community Based Perpetrator Intervention Trials – Perpetrator Intervention Trials Advisory Group
[4] Family Safety Victoria (2018). Terms of Reference - Community Based Perpetrator Intervention Trials – Providers Forum
[5] Family Safety Victoria (2018). Terms of Reference - Community Based Perpetrator Intervention Trials – Case management Forum
Conclusion and future considerations
8.1 Conclusion
The perpetrator cohort intervention trials and case management are addressing a service delivery gap for people using violence, and have contributed to delivering on recommendation 87 of the Royal Commission to “research, trial and evaluate interventions for perpetrators”.
The cohort intervention trials have provided a more tailored program design to particular cohorts of people who use violence, to better meet their needs. The analysis demonstrates that different design features work for different cohorts, for example cultural healing components for Aboriginal cohorts.
Within the cohort intervention trials there is a current service gap for people with mental illness or substance abuse, indicating a different approach may be required for engaging workforces and organisations within these sectors to design and pilot an appropriate program. Further, it will be important to consider the future delivery of the programs moving beyond a pilot stage, to ensure people who use violence have access to the tailored support programs they need, regardless of where they reside in Victoria.
Case management has also received positive feedback in terms of appropriateness of its design and implementation. In particular, providing one-on-one support that is tailored has reportedly assisted in meeting the needs of people using violence, particularly those who have more complex needs. It has also contributed to ‘group readiness’, prior to people who use violence entering into group MBCPs. Consultations with people who use violence indicate more could be done to support and provide clarity around exit planning.
Several enabling features of the cohort intervention trials and case management were identified.
- Creating trusting relationships between participants and facilitators, and among group members to encourage engagement and participation.
- Utilising both individual and group work in a complementary manner.
- Balancing accountability with a trauma informed approach to address the underlying factors contributing to violent behaviour.
- Facilitating a holistic, wrap-around approach to address contextual factors in a person’s life by connecting them to the broader service system.
- Allowing flexibility in approach for people with different levels of need and at varying stages of change.
- Providing family safety contact support to people who experience violence
Specific challenges were faced by both case management and cohort intervention trials during implementation.
- Funding uncertainty and short timeframes, which made implementation later for some cohort intervention trials and made workforce recruitment and retention challenging.
- Lack of focus on the family safety contact function, including adequate resourcing.
- Workforce capability, including challenges recruiting appropriately skilled staff and retaining them throughout the duration of the program (exacerbated by funding uncertainty).
- Data collection through IRIS was not fit-for-purpose.
- Exit planning was not always considered from the outset, and was unclear to some program participants
- Referral processes have not been systematic, often relying on intra-organisation referrals or from the courts or child protection
- Brokerage underspend due to uncertainty in how to use it appropriately
- Confusion regarding eligibility and referral pathways, particularly the mandated versus non-mandated aspect of the program.
These challenges are not uncommon for pilot programs during their establishment phase, and in light of the significant reforms occurring in Victoria in family violence. Provision of ongoing funding for case management and an additional year of funding for the cohort intervention trials provides new opportunities to overcome these challenges.
There are positive indicators of program effectiveness, including high rates of attendance, retention and engagement with the programs among people who use violence. People who use violence have also reported improving their understanding of what constitutes family violence, understanding the impact of their behaviour on others and there are examples of them self-reporting taking responsibility for their behaviour. While promising, triangulating these findings with the views of people who experience violence suggests these early indicators of progress need to be treated with caution. Ongoing monitoring particularly from the perspective of the person experiencing violence will be critical to measuring outcomes over the longer term.
8.2 Future considerations
This outcome evaluation report identifies several areas for ongoing improvement or enhancement, particularly as the programs transition from pilots to ongoing funding (case management) or providing services for an additional year (cohort trials). There are eight overarching improvement opportunities, and three that relate to cohort interventions. These are described in detail below.
8.2.1 Overarching opportunities
Building focus on the role of the family safety contact. The family safety contact role has not been a focus of the programs to date. As outlined in Section 4.7, the family safety contact function has either been ad hoc and unexpected and/or created barriers to access through the involvement of the person who used violence with the same service provider. This role is currently being aligned to the MARAM framework. Communities of practice for the family safety contact function and their supervisors is now occurring, delivered by No to Violence. Several steps can be taken to ensure the intention of the role is understood and embedded within the programs going forward:
- Funding agreements and/or submissions should allocate specific funding to this role, over and above what may currently be provided by the service provider. The purpose of this is to overcome existing family safety contact workers being used for these programs without additional resourcing. Service providers and funding submissions should factor in resources for this role in their budgets.
- FSV utilise the newly initiated training and communities of practice for the family safety contact function to better understand the roles, their function and broader system integration implications.
- FSV can provide additional guidance material to service providers on how the person experiencing violence can be appropriately connected to ongoing support, where this is preferred to contact with the family safety contact worker. Particular requests were made by people who experienced violence for financial support, referral to programs, and on-going involvement in support groups or counselling. A few participants also identified that there could have been greater support provided for their children, such as access to a child psychologist.
It is advised this opportunity is prioritised, as it directly affects the safety of the person experiencing violence.
Strengthening the referral pathway by raising awareness of the programs within the service system. As outlined in Section 7.3 there is a need for a more sophisticated approach to referrals that encourages and leverages system connectivity. Raising awareness of the programs, and providing guidance on when and how to refer to the programs, is an initial step to improve the referral pathway. Capacity building within the broader service system connectivity is particularly important to avoid misidentification of the primary aggressor. To strengthen the referral pathway, it is advised that:
- FSV actively work with the Orange Door implementation teams to ensure that as they are rolled out, there is a process for knowing which cohort intervention trials and case management programs are available within the DHHS area.
- Guidance material is provided on client eligibility, to avoid confusion regarding whether or not the programs are mandated. This material could be developed for different audiences, including service providers, so they understand what the process is for accepting someone if they are on a CCO, clients, and major referrers including Magistrates and Child Protection.
Contributing to building workforce capability. Recognising the challenges associated with recruiting an appropriately skilled workforce, there may be a role for FSV to play in ensuring there is sufficient representation of, and training to develop, the perpetrator workforce, including those from a diverse background. This should align with implementation of Building from Strength: 10-year industry Plan for Family Violence Prevention and Response. This plan identified a high desire among the family violence workforce for training in working with people who use violence, and that immediate actions included ‘funding the development and delivery of training to meet immediate upskilling needs’ and specifically identified working with people who use violence as an example of this. As such, the Industry Plan represents an opportunity for the FSV project team to share their knowledge on working with people who use violence, and articulate why this is important to promote safety among people experiencing violence. While this may be beyond the initial scope of the project team’s work, it is nonetheless a critical input into the success and sustainability of the programs it funds.
Improving accountability, governance and reporting of the programs through FSV. During the pilot stage, the FSV project team was appropriately focused on major project establishment activities, including developing operational guidelines, assessing and awarding submissions for funding, establishing governance arrangements and providing ongoing implementation support. Given the ongoing funding for case management and an additional year of funding for the cohort intervention trials, there is now a need to develop stronger monitoring and accountability mechanisms in future.
Specifically, this includes establishing or improving existing data collection systems for outcome reporting, including ensuring a consistent approach is adopted across providers. This would build on the work undertaken through this evaluation. This should clearly cover reliable and consistent methods for understanding how many participants have accessed the programs, demographics of the program participants, and referral pathways. Where service providers have not met agreed performance measures, this needs to be actively managed by FSV and APSS, and transparently reported. Clear role delineation between FSV and all of the APSS is required to support this process.
Currently, the data collection tool developed by the evaluators as part of this evaluation has filled a gap by collecting outcome measures and data where it may not be reliably collected via IRIS. Sustainable outcome data collection methods need to be established beyond the life of the evaluation. These recommendations are necessary for overall accountability purposes, particularly where providers are not meeting their service obligations.
Providing improved exit planning for case management participants. Service providers need to ensure exit planning is included within their services, and that this is clearly communicated to program participants. This opportunity relates specifically to the case management program, since the cohort trial participants had a clearly defined program end date. Setting boundaries between the case worker and participant upfront may assist in managing this process. Additional training or guidance to service providers on how to support exit planning may also contribute to improved exit planning, as would opportunities for ongoing supervision.
Providing clarity around funding. Lack of notice regarding future funding was a major impediment to successful implementation of the programs (see Section 7.4). Noting the additional funding provided 2019/2020, it is advised that:
- DHHS, through FSV, release and confirm funding amounts for the case-management service providers as soon as practicable.
- DHHS, through FSV, provide clarity to cohort service providers regarding the future of their funding at least one quarter prior to funding ceasing.
While this is at times outset the control of the FSV project team, it is important to pursue this recommendation where possible, given the impact it can have on the sustainability and effectiveness of the programs.
Adopting a systems approach by creating alignment with the justice perpetrator programs. The intention of this opportunity is to ensure there is clear guidance and pathways for when people who use violence should be referred to the justice programs versus the cohort intervention trials or case management. Avoiding duplication between these programs contributes to a more efficient service system. This could be achieved by using the existing program governance frameworks that incorporate members from both the justice and cohort intervention trials, but focus discussion on how the programs can complement each other.
Long-term research and evaluation. The cohort intervention trials were designed to be pilots and thus this evaluation only captured the short-term outcomes of the interventions. Further, the process of behaviour change occurs over a long time period, often involving multiple interventions through the web of accountability. As such, this evaluation was unable to show the effect of the programs over a longer time period. Further, evaluation of MBCPs has not occurred in a systematic way in Victoria, and this evaluation has not analysed the MBCP group work element (this was out of scope). For this reason, it is recommended further monitoring and evaluation occurs both for mainstream MBCPs, and the programs within scope of this evaluation. This will assist in better understanding the sequencing of interventions across community and justice settings.
8.2.2 Cohort specific
Tailoring implementation and reporting targets for Aboriginal cohorts. As outlined in Section 5.4, service providers for Aboriginal cohorts may take additional time to implement and deliver programs for a range of reasons, including to establish strong partnerships with other agencies, to build community trust of the program to facilitate word-of-mouth referrals, and so program content can incorporate cultural healing. To ensure program funding and reporting supports Aboriginal cohort providers and recognises these differences, it is suggested that:
- Consideration be given to tailoring funding agreements with Aboriginal providers to reflect these differences, particularly in relation to expected numbers of program participants within particular timeframes. Reviewing the effectiveness of these programs in the same timeframes as other service providers may lead to misleading conclusions being drawn, if it is implementation features (such as strong partnerships) that are still in development rather than the program itself that is not effective.
- Funding agreements should also allow support for cultural healing. This may include compensation for Elder involvement, transportation costs to sites of cultural importance, or longer program timeframes to create time for healing from past trauma.
Building capability within the mental health and AOD workforces to encourage the design of suitable programs for these cohorts. There remains a service need for this cohort. To ensure the Recommendations of the Royal Commission are fulfilled, and more importantly to ensure programs are delivered to cohorts where there is a clear need, it is important programs are designed and delivered for people with mental illness and/or substance abuse. Given the lack of appropriate responses in the initial funding round, this may require a different approach driven by FSV.
Future work would need to be done in the context of the Industry Plan and work already being undertaken by FSV to build the capacity of the existing mental health and AOD workforce. It is understood that FSV have already embarked on this process through the Specialist Family Violence Capacity Building Program in AOD and mental health workforces, and provision of funding for No To Violence and Domestic Violence Victoria for a coordination function. Given this may be a significant undertaking, some work in this area may fall outside the mandate of the immediate FSV project team.
There is also a need to build capacity in other mainstream services, to support these cohort over the longer term and as they engage with other support services such as housing. These mainstream services need to be equipped and capable of responding to diversity.
Consider opportunities to scale the programs. The programs were intended to be pilots in their initial year. During their second year of funding, consideration should be given to the ongoing future of the programs, and opportunities for state-wide scaling. Given the intensity of the programs, this needs to consider whether adaptations are made to existing MBCPs adopting enabling features of the trials, or adopting other means to improve access to these same cohorts located in other parts of the State. Given there is need for the programs within select areas of the State where they are currently being piloted, it is likely this need would extend state-wide. A needs analysis and feasibility assessment would need to be conducted initially to determine which programs and where to target them, recognising the resource intensity involved in scaling. At a minimum, this evaluation has identified six practice features that should be visibly incorporated into any future iteration of the programs.
References
ANROWS (2019). Men’s behaviour change programs: Measuring outcomes and improving program quality: Key findings and future directions (Research to policy and practice, 01/2019). Sydney, NSW: ANROWS.
Bartels, L. (2010). Emerging issues in domestic/family violence research (Research in practice no. 10). Canberra: Australian Institute of Criminology.
Brown et al, (2016). A study of the impact on men and their partners in the short term and in the long term of attending behaviour change programs. Department of Social work, Monash University, Pg. i.
Carvalho, A. F., Derlega, V. J., Lewis, R. J., Viggiano, C., and Winstead, B. A. (2011). Internalized sexual minority stressors and same sex intimate partner violence. J. Fam. Violence 26, 501–509.
Centre for Forensic Behavioural Science—Swinburne University; Victorian Institute of Forensic Mental Health (Forensicare), Submission 649.
Crichton-Hill, Y. (2001). Challenging ethnocentric explanations of domestic violence. Trauma, Violence & Abuse, 2(3), 203–214.
DAIP. 2019. “What Is the Duluth Model?” Available from: https://www.theduluthmodel.org.
Debbonaire, T. (2015). Responding to diverse ethnic communities in domestic violence perpetrator programs. Berlin, Germany: Work with Perpetrators European Network.
Department of Health and Human Services (2018), Dhelk Dja: Safe Our Way – Strong Culture, Strong Peoples, Strong Families, Available at: www.vic.gov.au/familyviolence
Eckhardt, C, Murphy, C, Whitaker, D, Sprunger, J, Dykstra, R and Woodard, K (2013). The Effectiveness of Intervention Programs for Perpetrators and Victims of Intimate Partner Violence. Partner Abuse, The partner abuse state of knowledge project part 5, 4 (2). Springer Publishing: 196–231.
Edwards, K., Neal, A. and Sylaska, K. (2015). Intimate Partner Violence Among Sexual Minority Populations: A Critical Review of the Literature and Agenda for Future Research, Psychology of Violence, 5:2.
Farrelly, J. (2016). ‘What is the Duluth Model for tackling domestic violence?’
Gondolf, E.W. (2007) Theoretical and research support for the Duluth Model: A reply to Dutton and Corvo.
Hill, J (2019). See what you made me do, Black Inc Books.
Johnson, M.P. (2008). A Typology of Domestic Violence: Intimate terrorism, violent resistance, and situational couple violence. Boston: Northeastern University Press.
Kelly, L and Westmarland, N (2015). Domestic Violence Perpetrator Programmes: Steps towards change. Project Mirabal Final Report. London and Durhm: London Metropolitan University and Durham University.
Levesque, D. A., Gelles, R. J., & Velicer, W. F. (2000). Development and validation of a stages of change measure for men in batterer treatment. Cognitive Therapy and Research, 24, 175-199.
Lloyd, K (2015). Homophobia, Transphobia and Men’s Behaviour Change Work. No To Violence Male Family Violence Prevention Association, 14–15.
Mackay, E., Gibson, A., Huette, L. and Beecham, D. (2015). Perpetrator interventions in Australia: State of knowledge paper, ANROWS.
Maiuro, Roland D, and Jane A Eberle. (2008). State Standards for Domestic Violence Perpetrator Treatment: 23 (2); Urbis. 2013. Literature Review on Domestic Violence Perpetrators, Available at:https://www.dss.gov.au/sites/default/files/documents/09_2013/literature….
Mikakos, J (2018). Media release: BREAKING THE CYCLE OF FAMILY VIOLENCE. Available at: https://www.premier.vic.gov.au/wp-content/uploads/2018/08/180823-Breaki…
Miller, S and Meloy, M. (2006) Women’s use of force, Violence Against Women, Vol. 12, No.1, pp 89-115
New York Model for Batterer Programs (2015). NY Model.
No To Violence, Men’s Behaviour Change Programs in Victoria – a Sector Snapshot, April 2011.
No to Violence. (2017). Men’s Behaviour Change Group Work: Minimum Standards and Quality Practice.
No To Violence (2018). Position Statement: Online programs for men who use family violence.
No to Violence (n.d.) Submission to the Family Law Council.
NSW Attorney General & Justice. 2012. Towards Safe Families: A Practice Guide for Men’s Domestic Violence Behaviour Change Programs.
Queensland Parliament (2014). Legal Affairs & Community Safety Committee
Relationships Australia Victoria (2013). Effective Men’s Behaviour Change Programs for Culturally and Linguistically Diverse Men. Available at: http://www.familyviolencehumeregion.com.au/wp-content/uploads/2013/04/R….
RMIT Centre for Innovative Justice (2015). Opportunities for Early Intervention: Bringing perpetrators of family violence into view.
RMIT Centre for Innovative Justice (2016). Pathways towards accountability: mapping the journey of perpetrators of family violence- Phase 1, Pg. 3.
Rolle, L., Giardina, G., Caldarera, A.m., Gerino, E and Brustia, P. (2018). When Intimate Partner Violence Meets Same Sex Couples: A Review of Same Sex Intimate Partner Violence. Frontiers in Psychology, Available at: https://www.frontiersin.org/articles/10.3389/fpsyg.2018.01506/full
Scott, K and Wolfe, D (2003). Readiness to change as a predictor of outcome in batterer treatment. J Consulting and Clin Psyc. 71 (5); Williamson, P., Day, A., Howells, K., Bubner, S., & Jauncey, S. (2003). Assessing offender readiness to change problems with anger. Psychology, Crime and Law, 9(4), 295-307.
State of Victoria (2016), Royal Commission into Family Violence.
Stith, S. M., McCollum, E. E., Rosen, K. H., & Thomsen, C. J. (2004). Treating marital violence within intact couple relationships: Outcomes of multi-couple versus individual couple therapy. Journal of Marital and Family Therapy, 30(3), 30-18.
Urbis (2013). Literature Review on Domestic Violence Perpetrators; NSW Attorney General & Justice (2012). Towards Safe Families: A Practice Guide for Men’s Domestic Violence Behaviour Change Programs.
Vlais, R (2014). Ten Challenges and Opportunities for Domestic Violence Perpetrator Program Work. Available at: https://ntv.org.au/advocacy-media/resources/.
Vlais, R. (2017). Scoping study of innovations in family and domestic violence perpetrator interventions. Family Safety Branch, Commonwealth Department of Social Services.
Vlias, R., Ridley, S., Green, D. and Ching, D. (2017). Family and domestic violence perpetrator programs – Issues paper of current and emerging trends, developments and expectations. Stopping Family Violence Inc
Zalmanowitz, S., Babins-Wagner, R., Rodger, S., Corbett, B. and Lescheild, A. (2013). The Association of Readiness to Change and Motivational Interviewing with treatment outcomes in males involved in domestic violence group therapy, Journal if Interpersonal Violence 28(5) 956-974.
Glossary
| Acronym | Full name |
|---|---|
|
ANROWS |
Australia’s National Research Organisation for Women’s Safety |
|
ANU |
Australian National University |
|
AOD |
Alcohol and other drugs |
|
CALD |
Culturally and linguistically diverse |
|
DHHS |
Department of Health and Human Services |
|
FSV |
Family Safety Victoria |
|
HREC |
Human Research Ethics Committee |
|
LGBTI |
Lesbian, Gay, Bisexual, Transgender, Intersex |
|
MBCP |
Men’s behaviour change program |
Acknowledgement
We acknowledge those who have been affected by family violence, including those who are currently, or have previously experienced family violence. We solemnly acknowledge those individuals lost to family violence.
We acknowledge the Victorian Aboriginal people as the First Peoples and Traditional Owners and Custodians of the land and water on which we rely. We acknowledge and respect that Aboriginal communities are steeped in traditions and customs built on a disciplined social and cultural order that has sustained 60,000 years of existence. We acknowledge the significant disruptions to social and cultural order and the ongoing hurt caused by colonisation. We acknowledge the ongoing leadership role of Aboriginal communities in addressing and preventing family violence.
A note on terminology
In this report, we use the term ‘people who experience violence’ and ‘people who use violence’. These were the preferred terms identified by service providers. People who use violence is also used interchangeably with program participants. We use the term ‘perpetrator’ to refer to the new community-based cohort interventions and case management program, since this is the name of the programs adopted by Family Safety Victoria (FSV). It is also used to refer to ‘perpetrator interventions’ more generally.
‘Accountability’ in the context of this report refers to people who use violence ‘taking responsibility' or ‘ownership’ of their violent behaviour. This definition has been adopted based on feedback from providers for two reasons. Firstly, to distinguish between system-level factors holding people who use violence to account (i.e. justice responses) versus people who use violence taking responsibility and accepting the consequences for their own behaviour. This reflects that only the person who uses violence can choose to end their use of violence.
Secondly, this definition of accountability acknowledges that, for a number of participant cohorts referenced in this report, the community and/or government is also accountable for inflicting past experiences of trauma and/or discrimination on these groups. Further, the system should provide people who use violence with appropriate mechanisms to enable them to take responsibility for their behaviour. This should be supported by a ‘web of accountability’, involving system-wide responsibility to create improved system integration, and a more connected and coordinated response to both people who use violence and people who experience violence. This reflects that the system can and should use both justice and community responses to hold responsible the person who uses violence.
Appendix A: Indicator Framework
Process evaluation questions
Appropriateness
| Evaluation questions | Indicators | Measure | Data sources |
|---|---|---|---|
| What is the evidence of continued need for the program and role for government in delivering this program? (P1) | Evidence that need is not being met by other programs for targeted cohort groups |
|
|
| Inability to access MBCPs |
|
|
|
| Diversity of participants based on needs and circumstances |
|
|
|
| Have the initiatives been implemented as designed? (P2) | Realisation of delivery activities as outlined in submissions and program logic |
|
|
| How are the initiatives innovative and contributing to best practice? (P3) | Evidence of innovative program features and contribution to best practice |
|
|
Effectiveness
| Evaluation questions | Indicators | Measure | Data sources |
|---|---|---|---|
|
Are there early positive signs of change that might be attributable to the program? (P4) |
Increase in people who experience violence’s feelings of safety and support People who use violence report to understand the factors contributing to their behaviour, and how it impacts others |
|
|
| To what extent are the outputs being realised? (P5) | Uptake of programs among people who use violence and people who experience violence |
|
|
| Have people who use violence and people who experience violence responded positively to the program, including enrolment, attendance/retention and satisfaction? (P6) |
Increase in people accessing the programs |
|
|
| Increase in referrals |
|
|
|
| Reduction in number of referrals not taken up for case management and intervention programs |
|
|
|
| People who use violence reported level of satisfaction of the program |
|
|
|
| What are the barriers and enablers to effective referral of participants? (P7) | Number of referrals and drivers of this |
|
|
| What governance and partnership arrangements have been established to support the implementation of the initiatives and are these appropriate? (P8) | Presence of governance and partnership arrangements and attitudes toward these |
|
|
| Frequency and nature of FSV and DHHS’s interaction with service providers |
|
|
|
| Do the program workforces have a clear idea of their roles and responsibilities? (P9) | Stakeholders report to have a clear understanding of their role in program delivery |
|
|
| What components of the model are perceived to be the most valuable? (P10) | Identification of enablers |
|
|
| What improvements to the service model could be made to enhance its impact? (P11) | Identification of barriers and improvement opportunities |
|
|
| Have there been any unintended consequences, and if so, what have these been? (P12) | Identification of unintended consequences |
|
|
Efficiency
| Evaluation questions | Indicators | Measure | Data sources |
| Has the department demonstrated efficiency in relation to the establishment and implementation of the program? (P13) | FSV/DHHS resources used to implement the program have not been wasted |
|
|
Impact evaluation
Appropriateness
|
Evaluation questions |
Indicators |
Measure |
Data sources |
|||
|
Are the programs responding to the identified need/problem? (I1) |
Increase in perpetrators and women who use force accessing intervention programs and case management, including where they otherwise would not have (uptake) |
|
|
|||
|
Perpetrator and women who use force report the program has been appropriate for their needs |
|
|
||||
|
What are the design considerations of the program to support scalability? (I2) |
Stakeholder assessment of program scalability |
|
|
|||
Effectiveness
|
Evaluation questions |
Indicators |
Measure |
Data sources |
|||
|
Have the program inputs, activities and outputs led to the desired change mapped out in the program logic? [1] (I3) |
Service provider workers challenge violence, threatening and controlling attitudes and behaviours |
|
|
|||
|
Service provider workers encourage people who use violence to recognise the effects of their violence on others and take responsibility for their behaviour |
|
|
||||
|
People who use violence report to understand the factors contributing to their behaviour, and how it impacts others |
|
|
||||
|
Have program participants and victim/survivors responded positively to the program (enrolment, attendance, completion, satisfaction)? (I4) |
As per the process evaluation question plus: Number or enrolments, attendance rates, completion rates |
|
|
|||
|
What are the drivers for effective participant engagement in the programs? Does this differ according to the different cohorts? (I5) |
Reasons for the increase in people accessing the programs Reason for engagement in the program |
|
|
|||
|
What is the impact of the program on victims/survivors perceptions of safety? (I6) |
Increase in people who experience violence’s feelings of safety and support |
|
|
|||
|
What were the barriers and facilitators to the programs being integrated into the broader service system? (I7) |
Stakeholders views on system barriers and facilitators |
|
|
|||
|
What impact has the program had on the management of risk associated with this cohort? (I8) |
Providers use and experience of MARAM (risk assessment framework) |
|
|
|||
|
Decrease in perpetrator use of violence and women who use force |
|
|
||||
|
What impact has the program had on referral pathways and information transfer between community services and relevant authorities? (I9) |
|
|
|
|||
|
What impact has the program had on the confidence, knowledge and skill of the case management and service delivery workforces in supporting the target cohort in the community? (I10) |
Case managers reportedly feel confident in undertaking their role |
|
|
|||
|
Are key stakeholders, including the program workforces, supportive of the model? (I11) |
Stakeholders express support for the model |
|
|
|||
|
What would be the impact of ceasing the program (for example, service impact, jobs, community) and what strategies have been identified to minimise negative impacts? (I12) |
Identification of the impact and mitigation strategies |
|
|
|||
Efficiency
|
Evaluation questions |
Indicators |
Measure |
Data sources |
|||
|
Has the program been delivered within its scope, budget, expected timeframe, and in line with appropriate governance and risk management practices? (LP) (I13) |
Extent to which the program was delivered with fidelity and within planned scope, budgets and timeframes |
|
|
|||
|
Has the department demonstrated efficiency and economy in relation to the delivery of the program? (LP) (I14) |
The program could not have been delivered in less time, or with less human or financial resources |
|
|
|||
|
The number of people who use violence referred to the program is as anticipated |
|
|
||||
|
Does the initial funding allocated reflect the true cost required to deliver the program? (I15) |
Cost to deliver the program compared with original budget |
|
|
|||
Italicised = lapsing program evaluation guidelines
Program refers to both the case management program and perpetrator intervention trials
Italicised evaluation questions reflect those that have been added by Deloitte Access Economics, that are in addition to the lapsing program guidelines and the questions posed by Family Safety Victoria in the RFP
[1] This question aligns with the lapsing program evaluation question: What is the evidence of the program’s progress toward its stated objectives and expected outcomes, including alignment between the program, its output, departmental objectives and any government priorities?
Appendix B: Detailed data collection approach
Data collection
The data collection involved a mix of primary and secondary data collection, as outlined below:
Primary data sources
Stakeholder interviews
Consultations with non-clients, including individual providers, FSV and DHHS representatives, coordination and referral staff, and advisory and peak bodies was undertaken to understand the process of the designing and implementation of the programs, and the barriers and enablers in delivering/overseeing the programs. An overview of the stakeholders consulted is shown in Table 2.2.
Table 8‑1 Phase 1 non-client interviews
|
Stakeholder group |
Phase 1 |
Phase 2 |
|
Program delivery staff in contracted agencies (including case management) |
14 focus groups (7 cohort trials and 7 case management) |
12 focus groups (7 cohort trial and 5 case management) |
|
FSV and DHHS staff |
1 interview |
2 interviews |
|
Referral agency |
1 interview |
Nil |
|
No To Violence and Domestic Violence Victoria |
1 interview |
1 interview |
A total of 87 interviews were conducted with program participants, including both face-to-face and telephone. In consultation with FSV, key characteristics of interest were identified for recruitment. Obtaining a spread of participants across cohort trials and case management programs was considered preferable, including a mix of people who have used violence, as well as those who have experienced violence. Other variables included provider location (metro/regional) and target cohort of the program. The sampling and recruitment approach is outlined in Appendix C. Table 2.3 outlines the number of participants interviewed across key variables of interest.
Table 8‑2 Phase 1 and 2 client interviews
|
Cohort |
Victims |
Perpetrators |
Totals |
|
Case Management |
|||
|
Regional |
3 |
22 |
25 |
|
Metro |
1 |
8 |
9 |
|
Aboriginal |
2 |
8 |
10 |
|
LGBTIQ |
3 |
4 |
7 |
|
Totals |
9 |
42 |
51 |
|
Cohort trials |
|||
|
Cognitive impairment |
- |
6 |
6 |
|
Parents (fathers) |
6 |
7 |
13 |
|
Culturally diverse |
3 |
5 |
8 |
|
Aboriginal |
- |
2 |
2 |
|
Women who use force |
- |
4 |
4 |
|
Gender diverse |
- |
3 |
3 |
|
Totals |
9 |
27 |
36 |
|
Overall |
18 |
69 |
87 |
Fieldwork ran over a two-month period from late May 2019 until late June 2019. Eligible participants were offered the choice between completing an interview face-to-face or over the phone.
- All face-to-face interviews were conducted at the relevant provider’s premises, to ensure a safe and comfortable environment for both the participant and the researcher.
- Telephone interviews were organised for a time convenient to the participant.
The specific approach to recruitment is outlined in Appendix C.
Service provider data collection tool
To address gaps in data availability from the Integrated Reports and Information System (IRIS) system, the data management system used by FSV/DHHS for family violence programs, data was sought directly from service providers through a data collection tool. For each program participant and victim survivor, the tool included demographic, referral and outcome information.
The process for developing and administering this tool was undertaken in consultation with providers to ensure it was easy to use, did not create excessive administrative burden, and contained information that will be useful for providers in their own performance monitoring processes. The data collection tool included client outcome questions focused on behaviour change and victim survivor feelings of safety, aligned to the family violence outcomes framework. Three providers piloted the tool and provided feedback on useability of the tool. Following the first phase of data collection, information sessions on using the tool were held with providers, to address some of the difficulties experienced in phase one. A number of providers commented that collection of client outcome questions was incorporated into their own service delivery processes.
For the process data collection phase, 17 of the 31 providers completed and returned the tool. In the outcome phase this increased to 21 providers.
The limitations related to this data are discussed in Section 2.5.
Appendix C: Sampling and recruitment approach
People who use and experience violence
Sampling approach
In order to implement a sampling strategy, a number of contextual factors were considered, including the size of the programs, and the timing of commencement, and it is acknowledged that these may impact on the number and diversity of participants recruited for the evaluation. This requires determination of selection criteria, noting that the smaller the sample size, the fewer selection criteria should be used.
For this evaluation, the following selection criteria were considered (noting that they are not mutually exclusive – e.g. victim/perpetrator sets belong to either individual and/or group interventions):
- inclusion of both ‘victims’ and ‘perpetrators’
- individual and group approaches
- inclusion of ‘cohort’ groups.
Table 8.1 shows the sampling matrix that was developed. This represents the proposed number of interviews for each phase. The final numbers were subject to participant availability and willingness to participate.
Table 8‑3 Sampling approach for people who use and experience violence
|
Cohort |
People who experience violence |
People who use violence |
|
Case Management |
||
|
Regional providers |
4 |
4 |
|
Metro providers |
4 |
4 |
|
Aboriginal providers |
4 |
4 |
|
LGBTIQ provider |
4 |
4 |
|
Total |
16 |
16 |
|
Cohort trials |
||
|
Bethany |
4 |
4 |
|
Drummond st |
4 |
4 |
|
Anglicare |
4 |
4 |
|
Baptcare |
4 |
NA |
|
Peninsula Health |
4 |
4 |
|
BDAC |
4 |
4 |
|
InTouch |
4 |
4 |
|
Total |
28 |
24 |
|
Overall total |
44 |
40 |
Recruitment
A flexible, indirect recruitment approach (recruitment via service providers) was adopted for the current research. Researchers worked closely with program providers and participant case workers to identify suitable participants for the research. Strict exclusion criteria were adhered to in the identification of participants in order to uphold the ethical integrity of the research and ensure the safety of all participants and the researchers. The following criteria were adhered to in recruitment:
Given the potential risk for violence to escalate, people who use violence should only be invited to be interviewed if the person who has experienced violence is currently engaged with a family safety contact worker or an equivalent service;
- clients must be in-service, and not just in the referral stage of the program
- involvement in the evaluation should be unlikely to disrupt client engagement in the service
- involvement in the evaluation should be unlikely to place unreasonable burden on clients
- clients should be selected who will not pose a risk to researchers.
An additional safety measure involved avoiding the ‘pairing’ of people who have used violence and people who have experienced violence known to be currently, or previously, in a relationship. This was due to potential concerns around safety and the confidentiality of discussions.
To facilitate this indirect recruitment approach, researchers followed a number of steps (see Figure 2). A primary approach e-mail was initially sent to 31 providers (7 cohort, 24 case management) to introduce the research and to invite providers to forward eligible participants. A time for a follow-up telephone conversation with providers was then scheduled, to discuss the approach in more detail.
Indirect recruitment approach adopted for the research
- send an initial approach email to providers
- arrange a phone discussion with the provider
- send information packs to providers
- monitor responses and contact participants.
Upon engaging providers and explaining the research, ‘information packs’ were then sent to providers (both electronic and physical copies were provided). Each information pack contained:
- information for case workers
- information sheets about the research for both people who have used and people who have experienced violence;
- a plain language information sheet
- an ‘expression of interest’ form for any interested participants.
Once providers had received the ‘information packs’, they were invited to approach and distribute materials to eligible participants. Interested participants were then able to complete an expression of interest form to provide consent to be contacted. Providers passed on completed forms to the research team, who contacted participants to organise a suitable date and time for interviews to occur.
Participants were not directly offered an incentive for participation in the research. Instead, an $85 ‘donation’ was made to a family violence organisation (which was agreed on being the provider offering the service). Providers were afforded discretion with regards to how they used the donation. Some providers chose to offer the incentive directly to participants or affected family members, whereas others chose to utilise the donation to fund program resources. Providers were considered best placed to make this decision, balancing the ethical need to reimburse participants, while also recognising that some deem it inappropriate to offer an incentive to a person who has used violence.
Non-client participants
Recruitment of providers, government, referral agency and peak body representatives for participation in interviews and focus groups will occur in consultation with FSV. Initial contact will be made by FSV, to inform potential participants of the evaluation and what will be involved in participation, and to seek the most appropriate contact details. If the potential participant expresses an interest in taking part, their details will then be passed onto the Deloitte Access Economics team to make contact with them to set up an appropriate time/location.
Providers will already be aware of their involvement in the evaluation due to their contractual obligations, as well as previous input sought via Deloitte Access Economics on the approach to the evaluation. All details will be confirmed in writing, by email. Providers will determine the most appropriate staff from their organisation to take part in the focus groups. Service providers will be informed that if they wish to withdraw from the consultation at any stage, or do not want to participate, this will not impact their relationship with FSV.
Appendix D: Detailed data overview
The charts below provide the detail of all responses in the data collection tool to the data domains presented in Chapter 5. This includes the total number of blank responses.
Chart C1: Case management
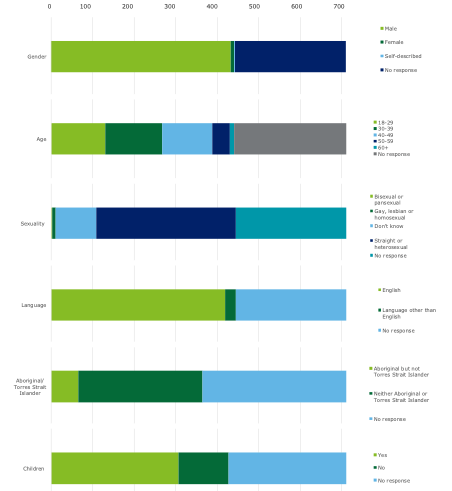
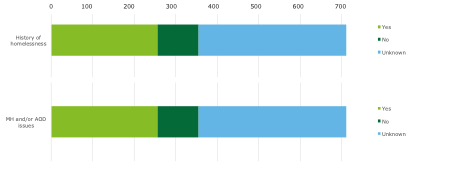
Chart C2: Cohort trials
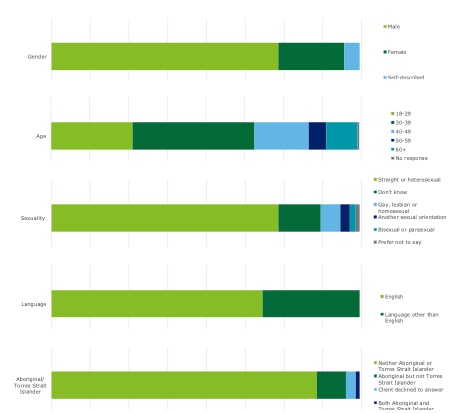
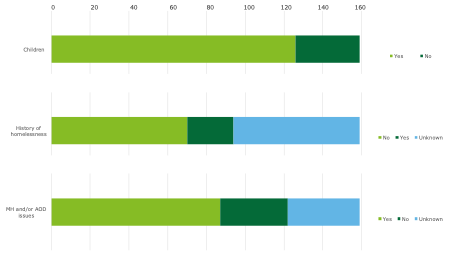
Appendix E: Outcomes data
Table 8-4 Entry outcomes data; cohort trials - people who use violence
| Entry | Exit | |
|---|---|---|
| "There is no justification for my abusive, controlling or violent behaviours" | ||
| Strongly agree | 16% | 27% |
| Agree | 45% | 35% |
| Neither agree or disagree | 22% | 25% |
| Disagree | 10% | 8% |
| Strongly disagree | 6% | 5% |
| Responses | N=77 | |
| "My abusive, controlling and violent behaviours have had lasting effects on my family members" | ||
| Strongly agree | 13% | 23% |
| Agree | 50% | 38% |
| Neither agree or disagree | 18% | 21% |
| Disagree | 12% | 9% |
| Strongly disagree | 8% | 9% |
| Responses | N=78 | |
| "[Person who experiences violence] and I have discussed how my behaviour affects our children" | ||
| Strongly agree | 2% | 25% |
| Agree | 44% | 45% |
| Neither agree or disagree | 42% | 25% |
| Disagree | 8% | 3% |
| Strongly disagree | 5% | 2% |
| Responses | N=64 | |
Table 8-5 Outcomes data; cohort trials - people who experience violence
| Entry | Exit | |
|---|---|---|
| "[Person who uses violence] tries to justify or make excuses for their abusive, controlling or violent behaviours" | ||
| Strongly agree | 11% | 4% |
| Agree | 75% | 68% |
| Neither agree or disagree | 11% | 11% |
| Disagree | 0% | 11% |
| Strongly disagree | 4% | 0% |
| Responses | N=28 | |
| "[Person who uses violence] understands the impact of their abusive, controlling and violent behaviours on family members" | ||
| Strongly agree | 0% | 4% |
| Agree | 71% | 82% |
| Neither agree or disagree | 14% | 11% |
| Disagree | 7% | 0% |
| Strongly disagree | 7% | 4% |
| Responses | N=28 | |
| "[Person who uses violence] and I have discussed how their behaviour affects our children" | ||
| Strongly agree | 4% | 7% |
| Agree | 71% | 75% |
| Neither agree or disagree | 14% | 11% |
| Disagree | 4% | 0% |
| Strongly disagree | 7% | 7% |
| Responses | N=28 | |
Table 8-6 Outcomes data; case management - people who use violence
| Entry | Exit | |
|---|---|---|
| "There is no justification for my abusive, controlling or violent behaviours" | ||
| Strongly agree | 16% | 44% |
| Agree | 52% | 26% |
| Neither agree or disagree | 16% | 18% |
| Disagree | 12% | 9% |
| Strongly disagree | 4% | 3% |
| Responses | N=207 | |
| "My abusive, controlling and violent behaviours have had lasting effects on my family members" | ||
| Strongly agree | 13% | 38% |
| Agree | 51% | 29% |
| Neither agree or disagree | 26% | 22% |
| Disagree | 6% | 6% |
| Strongly disagree | 4% | 6% |
| Responses | N=212 | |
| "[Person who experiences violence] and I have discussed how my behaviour affects our children" | ||
| Strongly agree | 12% | 46% |
| Agree | 46% | 23% |
| Neither agree or disagree | 30% | 21% |
| Disagree | 7% | 4% |
| Strongly disagree | 5% | 6% |
| Responses | N=151 | |
Table 8-7 Outcomes data; case management - people who experience violence
| Entry | Exit | |
|---|---|---|
| "[Person who uses violence] tries to justify or make excuses for their abusive, controlling or violent behaviours" | ||
| Strongly agree | 15% | 15% |
| Agree | 50% | 38% |
| Neither agree or disagree | 15% | 24% |
| Disagree | 18% | 18% |
| Strongly disagree | 3% | 6% |
| Responses | N=34 | |
| "[Person who uses violence] understands the impact of their abusive, controlling and violent behaviours on family members" | ||
| Strongly agree | 0% | 3% |
| Agree | 32% | 26% |
| Neither agree or disagree | 32% | 29% |
| Disagree | 26% | 29% |
| Strongly disagree | 9% | 0% |
| Responses | N=34 | |
| "[Person who uses violence] and I have discussed how their behaviour affects our children" | ||
| Strongly agree | 4% | 4% |
| Agree | 46% | 50% |
| Neither agree or disagree | 25% | 25% |
| Disagree | 21% | 18% |
| Strongly disagree | 4% | |
| Responses | N=28 | 4% |
Limitation of our work
General use restriction
This report is prepared solely for the use of Family Safety Victoria. This report is not intended to and should not be used or relied upon by anyone else and we accept no duty of care to any other person or entity. The report has been prepared for the purpose set out in the PAS contract dated 5 September 2018. You should not refer to or use our name or the advice for any other purpose.