- Date:
- 31 Dec 2020
ISBN 978-0-7594-0859-3
List of figures
Figure 3.1: Enquiries through the information sharing reforms dedicated enquiry line (phone) and inbox (email).
Figure 3.2: Email enquiries in relation to online training through the LMS.
Figure 3.3: Proportion of workforces indicating their organisation had policies covering child information sharing prior to and following commencement of the CIS Scheme.
Figure 3.4: Workforce perceptions of information sharing policies.
Figure 3.5: Workforce attitudes towards information sharing.
Figure 3.6: Proportion of survey respondents by changes to organisational record keeping before and after implementation of the CIS Scheme.
Figure 5.1: Frequency of refusals of incoming requests to share information among prescribed workforces.
Figure 5.2: Reasons for refusals of incoming requests to share information among prescribed workforces.
Figure 5.3: Frequency of refusals of outgoing requests for information among prescribed workforces.
Figure 5.4: Reasons for refusals of outgoing requests for information among prescribed workforces.
Figure 5.5: Workforces’ perceived effectiveness of information sharing to support child wellbeing, before and after CIS Scheme.
Figure 5.6: Enhanced ability to promote child wellbeing.
List of tables
Table 2.1: CIS Scheme Two-Year Review data collection activities.
Table 3.1: Proportion of enquiry line contacts by area of enquiry.
Table C.1: Profile of respondents who answered 2019 and 2020 Phase One prescribed workforces surveys.
Table C.2: Roles of respondents who answered in both workforces survey 2019 and 2020.
List of boxes
Box 3.1: Key findings – CIS Scheme implementation.
Box 3.2: Case study in implementation – Department of Health and Human Services (DHHS).
Box 4.1: Key findings – implementation enablers and barriers.
Box 5.1: Key findings – achievement of outcomes.
Box 5.2: Case study – proactive information sharing.
Box 5.3: Case study – filling crucial information gaps.
Box 6.1: Key findings – unanticipated adverse impacts of the CIS Scheme.
Box 7.1: Key findings – prescription of phase one entities under the CIS Scheme.
Box 8.1: Key findings – impact of the CIS Scheme on diverse and disadvantaged communities.
Acknowledgements
We gratefully acknowledge the contribution to this review of key stakeholders who participated in data collection activities to determine the effectiveness of implementation of the Child Information Sharing Scheme. Insights and experiences with information sharing across a diversity of sectors were generously provided by workforces and senior representatives of prescribed organisations and services and related sector peak/lead bodies.
We also thank key informants representing partner government departments and agencies for information about policy, support and practice related to information sharing reforms from a state-wide perspective, and the Department of Education and Training, as the lead department for the child information sharing reforms, for the support provided to this review.
We especially acknowledge the cooperation of service providers during the latter phase of this review when child and family related services were experiencing the additional demands that accompanied the coronavirus pandemic and the workplace challenges of continuing to safely support their clients and communities.
Abbreviations and acronyms
| ACCOs | Aboriginal community controlled organisations |
| AHPRA | Australian Health Practitioner Regulation Agency |
| AOD | Alcohol and other drugs |
| CALD | Culturally and linguistically diverse |
| CCYP | Commission for Children and Young People |
| CIS Scheme | Child Information Sharing Scheme |
| DET | Department of Education and Training |
| DHHS | Department of Health and Human Services |
| DJCS | Department of Justice and Community Safety |
| FSV | Family Safety Victoria |
| FVIS Scheme | Family Violence Information Sharing Scheme |
| ISEs | Information sharing entities |
| ISMARAM | Information Sharing and Family Violence Multi-Agency Risk Assessment and Management Framework |
| IST | DHHS Information Sharing Team |
| LGBTIQ | Lesbian, gay, bisexual, trans, intersex and/or queer |
| LMS | Learning Management System |
| MARAM | Family Violence Multi-Agency Risk Assessment and Management Framework |
| MCH | Maternal and Child Health services |
| TPAG | Training and Practice Advisory Group |
| VicPol | Victoria Police |
Key findings
Implementation
- Initial state-wide roll out of an intensive training program for Phase One prescribed workforces related to the information sharing reforms was attended by approximately 2,000 participants and served to create an awareness of the reforms within three months of their commencement.
- Additional training was provided by relevant government departments tailored to their respective workforces.
- Follow up support for Phase One implementation is ongoing and includes a range of learning resources and an enquiry line. There have been more than 6,000 registrations for online training.
- Family Safety Victoria sector grants to relevant peak/lead bodies have been important to extending the reach and understanding of the information sharing reforms among diverse sectors and workforces with varying experience of child-focus practice.
- Stakeholder feedback suggests there is continuing need to upskill prescribed workforces in the legislative provisions and requirements of the Child Information Sharing (CIS) Scheme to support effective implementation across the information sharing entities.
- Further work is required to support a consistent and informed level of understanding of the threshold for application of the CIS Scheme.
- There is evidence of improved workforce attitudes to child information sharing since commencement of the CIS Scheme and preparedness to share information.
- While organisational policies are in place to support workforces in implementing the CIS Scheme, there may be a low level of compliance with the record keeping obligations in the Child Wellbeing and Safety (Information Sharing) Regulations 2018 and explained in the Ministerial Guidelines.
Enablers and barriers to implementation
- Stakeholders have identified enablers and barriers to implementation of the CIS Scheme that relate to issues such as the anxiety of workers around privacy and confidentiality concerns, translation of policy into practice and understanding of child-focus practice.
- Data on information sharing requests is thin and will need to improve for effective and ongoing monitoring of the child information reforms.
- A number of strategies have been adopted by prescribed organisations and services to target culture change in support of effective implementation of the CIS Scheme. There is opportunity to better disseminate these innovative approaches to the potential advantage of Phase One and Phase Two prescribed workforces.
- While there is a high level of understanding about the purpose of the CIS Scheme further work is required to embed practice.
Achievement of intended outcomes
- Among prescribed workforces surveyed, there was a perception that legal restrictions and organisational policies that inhibited information sharing had decreased since commencement of the CIS Scheme, and that they were less likely to refuse a request for information after the introduction of the CIS Scheme. Privacy was also less likely to be cited as a reason to be used for refusing requests for information but was still likely to be a factor when survey respondents’ requests for information were refused.
- Information sharing activity appears to have remained mostly the same since commencement of the CIS Scheme based on the results of the surveys of prescribed workforces, with some evidence pointing to a slight decline in the level of activity. Other evidence suggests that during the coronavirus pandemic there may be specific forms of information sharing activity that have increased while others have decreased.
- There is some evidence for a cultural shift towards early identification of supports for children, with some prescribed workforces appearing to have lower thresholds for seeking information.
- Prescribed workforces also appear to be considering a wider range of information sources when doing case planning for children.
- There is increased evidence of collaboration and coordination between sectors at various levels, including between peak bodies, individual services, and individual workers.
- Continued support and education is required to build on early signs of positive outcomes to ensure that these reforms are firmly embedded among information sharing entities.
Unintended adverse impacts
- The formalisation of information sharing practices among some information sharing entities has caused local relationships to decline as informal information sharing between local agencies has decreased. However, it is noted that previous options for information sharing may not have been appropriate and an objective of the CIS Scheme was to provide confidence around the legality of child information sharing.
- In some cases, the CIS Scheme has complicated information sharing procedures for information sharing entities that previously shared information through other mechanisms. Information sharing entities are preoccupied with thinking about whether the CIS Scheme can be used and neglected the fact that they previously shared information through other avenues.
Prescription of information sharing entities
- Alignment of implementation of the CIS Scheme with the Family Violence Information Sharing (FVIS) Scheme and Family Violence Multi-Agency Risk Assessment and Management Framework was seen by Phase One prescribed workforces as consistent with the integrated way in which these reforms were being operationalised in practice.
- Interface of the FVIS and CIS Schemes has highlighted practices that can be strengthened to ensure the successful implementation of the CIS Scheme that include reinforcing the importance of routinely gathering accurate information, formalising standards for information collection and developing processes for documenting information sharing occasions and outcomes.
- Improved sharing of information between secondary/tertiary and universal services was considered to be more likely to deliver the early intervention benefits intended for the CIS Scheme, and the opportunity to promote child wellbeing outside of family violence contexts.
- For some Phase One prescribed organisations and services, expanding the CIS Scheme under planned Phase Two will enable a whole of organisation approach to the CIS Scheme and collaboration with other internal services to be prescribed under Phase Two.
- Choice of information sharing entities for Phase One has been appropriate when reflecting on the scale of implementation and the training required. There is a continuing need to build child information sharing capacity among Phase One information sharing entities.
- The selection of Phase One information sharing entities has illustrated the breadth of service providers in contact with children directly or indirectly through a family context and supports provided to parents/carers, and the opportunities to build a wider network of services able to participate in promoting child wellbeing and safety.
Impacts on diverse and disadvantaged communities
- The continuing need to improve engagement of diverse population groups with support services will affect the extent of the impact of the CIS Scheme in this area.
- More robust data collection related to application of the CIS Scheme will be required to monitor and assess use and impact of the CIS Scheme with diverse communities.
Aboriginal and Torres Strait Islander communities
- Aboriginal communities continue to be hesitant about information sharing being unsafe as:
- the CIS Scheme is not perceived to have been developed by Aboriginal people
- distrust and fear of the removal of children persists
- There is support for development of Aboriginal community understanding about the CIS Scheme, and the development of culturally appropriate training and resource materials for prescribed workforces.
- Consistent with the broader investigation of approaches to improve access to, and participation in services by diverse population groups, an improved understanding of issues that could potentially jeopardise sharing of child information will be important to avoid undermining engagement with services.
Executive summary
Executive summary of the Child Information Sharing Scheme Two-Year Review report.
Background
Child Information Sharing Scheme
The Child Information Sharing Scheme (the CIS Scheme) expands the circumstances in which professionals and organisations can share information to promote the wellbeing and safety of children. The CIS Scheme was proclaimed in September 2018 under the Child Wellbeing and Safety Act 2005 to enable prescribed organisations and services (information sharing entities) to share confidential information in a timely and effective manner. The first phase of information sharing entities are specified by the Child Wellbeing and Safety (Information Sharing) Regulations 2018 and were proclaimed on 27 September 2018. Phase One is comprised of approximately 28,000 workers representing around 700 entities primarily within the secondary and tertiary sectors. Phase One information sharing entities generally had high level permissions to share information about children and families and, with exceptions such as services working predominantly with adults, the impact of extending these permissions under the CIS Scheme was expected to be minimal.
The CIS Scheme forms part of the child information sharing reforms, together with a web-based Child Link Register currently under development to streamline access to information about participation of children in government-funded programs. It is expected that these reforms will:
- improve early needs and risks identification and support for children and their families
- change a risk averse culture in relation to information sharing
- increase collaboration and integration between child and family services
- support children’s and their families’ participation in services to which they are entitled.
Ministerial Guidelines were developed to support implementation of the CIS Scheme providing more detailed information including about the legislative principles for the CIS Scheme and the threshold for determining use of the CIS Scheme.
The CIS Scheme operates alongside family violence prevention reforms introduced similarly to support effective sharing of information between authorised organisations and services. The Family Violence Information Sharing Scheme (the FVIS Scheme) enables information sharing to facilitate assessment and management of family violence risk to children and adults, and the Family Violence Multi-Agency Risk Assessment and Management (MARAM) Framework guides information sharing under both information sharing schemes where family violence is present. The majority of the Phase One information sharing entities are prescribed under both information sharing schemes and the MARAM Framework. Depending on the circumstances and authorisations, Phase One information sharing entities may use either of the schemes on their own or apply both schemes where family violence is present and there are wellbeing and other safety concerns for children.
Governance arrangements for the CIS Scheme reflects a multi-agency approach consistent with the legislative intent and responsibility for the information sharing reforms. The Department of Education and Training leads the child information sharing reforms in close partnership with Family Safety Victoria, Department of Health and Human Services, Department of Justice and Community Services and Victoria Police. In anticipation of a significantly expanded group of professionals and services with the commencement of Phase Two of the CIS Scheme in the first half of 2021, new governance arrangements provide a strengthened focus on CIS Scheme implementation.
Purpose of this review
An independent review of the operation of the CIS Scheme within two and five years of commencement is required under section 41ZN of the Child Wellbeing and Safety Act 2005. This review represents the two-year review of the CIS Scheme covering the period September 2018 to September 2020. The two-year review was required to:
- Determine to what extent the CIS Scheme has been implemented effectively.
- Identify key enablers and barriers to implementation.
- Determine to what extent the CIS Scheme is achieving its intended outcomes.
- Consider and identify any adverse impacts of the CIS Scheme.
- Assess the success of the prescription of Information Sharing Entities.
- Assess impacts on diverse and disadvantaged communities.
- Include recommendations (as necessary) on any matters addressed in the review.
The review report is structured around these key areas of inquiry.
An independent review of the FVIS Scheme overlapped with this review both in terms of timeframe and information sharing entities. The recommendations of the FVIS Scheme two-year review, tabled in Parliament in August 2020, address shared issues. The recommendations have subsequently been supported in full or in-principle by the Victorian Government.
Review approach
The review commissioned by the Department of Education and Training was conducted by ACIL Allen Consulting in partnership with Wallis Market and Social Research Centre (Wallis). A program logic developed for the CIS Scheme underpinned the guiding evaluation framework and the collection of qualitative and quantitative information from a variety of new and existing sources. Data collection focused on stakeholder engagement and occurred predominantly at two points in time commencing in July 2019 with follow up in June 2020.
Information gathering focused on establishing attitudes and practices of workforces of prescribed organisations and services (prescribed workforces) to information sharing, the support provided by peak/lead bodies to their respective sectors for effective implementation of information sharing reforms and the extent of change to organisational record keeping processes and systems to facilitate implementation of the CIS Scheme. Data collection methods included surveys, interviews, virtual workshops, document review and case studies.
Implementation of the Child information Sharing Scheme
Workforce training
Initial intensive, face-to-face training for workforces of the Phase One information sharing entities was conducted during October to December 2018. The training approach was informed by a needs analysis and the deliberations of a Child Information Sharing Working Group with membership from relevant areas of government, and consultations with a Training and Practice Advisory Group with expertise across relevant workforces. The training adopted an integrated approach covering content for both information sharing schemes and an introduction to the MARAM Framework. Training was attended by approximately 2,000 participants, 35% of whom attended regional sessions.
Lead agencies driving the reforms considered that the training had served to create an awareness of the CIS Scheme and related information sharing reforms and to inform refinement of the strategic approach to building capacity among the Phase One information sharing entities. Subsequent training developed by partner government departments was tailored to their workforces, and peak/lead bodies were supported to develop sector specific supporting materials and resources. Whole-of-Victorian Government implementation supports for the CIS Scheme are predominantly provided through a variety of platforms managed by the Department of Education and Training. These include eLearning modules, with over 6,000 enrolments to date, Ministerial Guidelines that are legally binding for information sharing entities explaining operation of the CIS Scheme and a dedicated Enquiry Line for queries related to the information sharing reforms.
Utilisation of the Enquiry Line over the 18-month period to June 2020 suggests a growing understanding of the reforms although decreased contacts may also reflect awareness about, and access to a wider range of guidance and learning resources. Approximately 60% of all queries were related to the CIS Scheme, suggesting that the Enquiry Line will be an ongoing valuable source of support for information sharing entities.
In addition, the Enquiry Line could be harnessed to provide a better understanding in ‘real time’ of the nature and proportion of enquiries related to the CIS Scheme and the category of information sharing entity seeking clarification. This information could inform monitoring of the implementation of the CIS Scheme and any gaps in understanding at workforce and service level that might warrant targeted or different support.
| Recommendation ES 1 Enquiry Line Data Collection |
|---|
| That operation of the Enquiry Line be funded to accommodate the expansion of information sharing entities under the information sharing reforms, and to facilitate the collection of ‘real time’ data to inform effective implementation of the child information sharing reforms. |
Sector Grants Program
The Family Safety Victoria Sector Grants Program introduced in 2017-18 has provided sector implementation support funding to key representative and state-wide bodies for implementation of the information sharing and MARAM reforms. The Sector Grants Program focuses on implementation of the information sharing reforms in a family violence context. Whilst the activities supported by the Grants Program have benefited operation of the CIS Scheme, peak/lead bodies have not had the resources to bring a similar focus to the CIS Scheme and its wider application. Feedback from peak/lead bodies indicates that there is continuing work to successfully embed the CIS Scheme in prescribed organisations and services.
The Sector Grants Program has demonstrated the value of supporting targeted initiatives for key workforces in promoting effective implementation of reforms. There is opportunity to better leverage the support of peak/lead bodies in complimenting other efforts to promote early intervention and prevention through improved child information sharing. This support would be especially timely in also facilitating collaboration between peak/lead bodies representing sector workforces prescribed in Phase One of the CIS Scheme and proposed for Phase Two.
| Recommendation ES 2 Sector Support |
|---|
| That support be provided to sector peak/lead bodies, similar to the Family Safety Victoria sector grants, to strengthen the response to sector-specific needs of information sharing entities in understanding and applying the CIS Scheme in a range of circumstances and to promote cross sector collaboration and consistency. |
Perspectives of prescribed workforces
Feedback in 2020 through open-ended questions in the follow up 2020 workforces survey and workshops with prescribed organisations and services, suggests that CIS Scheme training and supporting resources continues to be a priority issue for prescribed organisations and services.
An area of continuing challenge for a number of information sharing entities has been interpretation of the concept of ‘wellbeing’ associated with use of the CIS Scheme which suggests a lack of confidence in the capacity for professional judgement in determining application of the CIS Scheme and highlights the varied familiarity of information sharing entities with child-focused practice frameworks. While universal services to be prescribed under Phase Two of the CIS Scheme are familiar with wellbeing frameworks, this is not the case for many Phase One prescribed workforces with a risk focus and adult user group. In addressing this concern, It was considered necessary to balance the original intent of the legislation regarding the importance of the breadth of circumstances relevant to wellbeing, while providing additional guidance to workforces on how they should assess and understand wellbeing for the purposes of the CIS Scheme.
| Recommendation ES 3 Assessing Threshold for ‘Wellbeing’ |
|---|
| That further guidance be provided for prescribed workforces regarding expectations associated with ‘promoting child wellbeing’ under the CIS Scheme. That this further guidance be informed by an audit of state-wide and sector specific resources with the aim of identifying guidance gaps, particularly in relation to promoting a shared understanding of child wellbeing and risk thresholds, and child and family service system roles and responsibilities in relation to child wellbeing. |
| Recommendation ES 4 Strengthening capacity of phase one workforces |
|---|
| That change strategies and ongoing training of information sharing entities related to the information sharing reforms continue to develop capacity among Phase One prescribed workforces and to facilitate integration of practice between Phase One and Phase Two prescribed workforces. This could be facilitated through workforce forums developed in collaboration with peak/lead bodies, and through support for local and place-based networks across sectors and promotion of local champions. |
Embedding the CIS Scheme in policies and guidelines
Given the complexity and legislative requirement for implementation of the CIS Scheme it has been important for prescribed organisations and services to ensure that internal policies and guidelines support their workforces in the appropriate sharing of information. Among prescribed workforces surveyed in 2019 who identified that their organisations did have policies on sharing child information prior to commencement of the CIS Scheme, there was mixed perceptions of the policies’ currency and value in enabling information sharing. Change at follow up survey in 2020, however, included a larger proportion of respondents reporting that the policies were up to date (85%, an increase from 65%), were sufficiently flexible and provided clear guidance on permission to share. There was a reduction in the perception that policies sometimes hinder early identification of needs or prevention of issues.
In relation to their understanding of how to share information, there was an increase in survey respondents who considered that they were aware of their legal responsibilities (from 74% prior to commencement of the scheme to 83% at follow up in 2020) and who knew where to go for guidance on information sharing (from 67% to 85% at follow up).
While there are positive indications of an improved level of workforce understanding of, and receptiveness to information sharing, there is a continuing conservative position regarding willingness to promote information sharing where it may be of benefit. This position supports stakeholder feedback about the evolving nature of the culture change that needs to occur and the further work to be done to embed the CIS Scheme in practice.
Information sharing entity systems and processes support monitoring of implementation of the CIS Scheme
Prescribed organisations and services were expected to leverage their existing systems to meet the record keeping requirements under the CIS Scheme. A selection of prescribed organisations and services were asked about whether there had been a need to make changes to their record keeping systems in anticipation of, and subsequent to introduction of the CIS Scheme.
Nearly three-quarters (74%) of organisations (n=54) indicated that changes had been made to record keeping arrangements in response to the CIS Scheme. Some of the changes made in preparation for the CIS Scheme included developing forms, improving and updating processes, updating client management systems, improving data protection processes, and developing spreadsheets to hold new information.
The Ministerial Guidelines[1] provide a list of required information for record keeping, which is set out in the Child Wellbeing and Safety (Information Sharing) Regulations 2018. Organisations surveyed in 2019 about their record keeping were asked about the extent to which they adhered to the list of required information in relation to each of the key activities in information sharing. Required information relating to the category of receiving a request had the highest rate of compliance with 74% of respondents reporting that all mandatory items were recorded. The remaining categories relating to information requirements for responding to a request, voluntary disclosure, and receiving and responding to a complaint, had an appreciably lower level of full compliance.
Required information for record keeping provides information sharing entities with an important source of internal monitoring of effective implementation of the CIS Scheme and an ability to assess any improved outcomes for children and their families. If capacity allows, the information collected by information sharing entities could potentially be aggregated by government to enable measurement of the contribution of the CIS Scheme to the intended outcomes, such as earlier intervention and prevention.
| Recommendation ES 5 Compliance with record keeping requirements |
|---|
| That CIS Scheme partner government departments work with information sharing entities in their respective sectors to promote compliance with the legislated record keeping obligations under the CIS Scheme, as explained in the Ministerial Guidelines. |
More recent feedback from prescribed organisation and services highlights ongoing refinement of processes and tools to support the information sharing entity’s commitment to taking responsibility for children. This has included amendment to intake forms for services that deal predominantly with adults to record any involvement of children and consent forms that raise client awareness of information sharing schemes.
A consistent conversation across services to ensure that service users are aware of and understand the information sharing reforms is important to effective implementation of the CIS Scheme and the ongoing process of engagement with service users and consumers (individuals, families and communities) more broadly.
| Recommendation ES 6 Service User Awareness |
|---|
| That training modules and templates identify information sharing entity responsibility for, and provide resources to support a consistent approach to service user awareness of the information sharing reforms and ensuring they understand their implications, the obligations of information sharing entities and the service user’s rights. |
There was little change reported by workforces in their perception of the level of effort needed to align their organisation’s practices, procedures and systems to the CIS Scheme over the period of the two workforces surveys. The average ranking of level of effort was 6.2 at baseline and 6.4 at follow up (0=very little effort and 10=extremely high level of effort; n=194). This result supports qualitative feedback from stakeholders that adjusting systems to the CIS Scheme has been ongoing in the period since commencement of the CIS Scheme, and that for many organisations, this has not been an inconsiderable effort.
Enablers and barriers to implementation
A wide range of enablers to effective implementation of the CIS Scheme through ensuring workforce skills and knowledge were cited by information sharing entities. These included:
- building workforce understanding of the legislative basis for information sharing to improve confidence in applying the CIS Scheme
- having an identified person with responsibility for implementation of the CIS Scheme
- translation of policy into practice including alignment with other policies, frameworks and guiding principles
- promotion of ongoing (experiential) learning through communities of practice.
Insights into barriers to effective implementation of the CIS Scheme because of a lack of workforce capability are provided by workforces surveyed in 2020 about the main reason for not requesting information. This largely derives from insufficient knowledge of the CIS Scheme. Other challenges experienced included:
- lack of practice in applying a child-focus
- lack of familiarity with the culture of other organisations
- privacy perceptions.
Activities delivered by information sharing entities to enable practice change
A range of innovative approaches have been developed by prescribed organisations and services to support practice change among their workforces. This has involved embedding training in relevant existing training programs, making the language around the CIS Scheme more accessible, enabling awareness of children in their work, and identifying professionals/leaders available for secondary consultations.
There should be a process for capturing and disseminating examples of approaches to supporting workforce practice change, such as the potential for proactive sharing. At a minimum, this could be demonstrated through a series of case studies that have regard for the structure, size and location of organisations and services.
| Recommendation ES 7 Disseminating approaches to practice change |
|---|
| That good practice case studies across a range of contexts be identified and shared through a variety of media, including through innovation workshops and published material. |
Achievement of intended outcomes
A number of positive outcomes were achieved in the implementation of the CIS Scheme. These included a perception among workforces that legal restrictions and organisational policies that inhibited information sharing had decreased, and that they were less likely to refuse a request for information after the introduction of the CIS Scheme. Privacy was also less likely to be cited as a reason to be used for refusing requests for information.
There were also early signs of cultural shift among workforces towards early intervention and prevention. Evidence provided by stakeholders indicated a greater willingness of their workforce to consider information sharing in cases which would have been perceived as not of sufficient concern to warrant information sharing prior to the CIS Scheme. Workforces were also beginning to look beyond their traditional sources of information to consider how other sources of information could supplement their case assessment and planning. However, these efforts were sometimes curtailed by the fact that workforces were not necessarily aware of who to seek information from, or with which services it would be appropriate to share information.
There was also evidence that workforces from different sectors were collaborating and coordinating better as a result of the CIS Scheme. Collaborative activities were evidenced at a broad range of levels, including between peak/lead bodies, leadership of individual prescribed organisations and services, and among individual workers.
It will be important to continue to enable Phase One secondary and tertiary services to actively seek opportunities to participate in child information sharing for purposes of promoting child wellbeing and safety. The implementation of Phase Two of the CIS Scheme should include strategies to strengthen existing and new efforts to leverage from the engagement with families and children of secondary and tertiary services, to optimise the extended support that might be available for shared clients.
| Recommendation ES 8 Role Clarity in collaborative practice |
|---|
| That the implementation of Phase Two of the CIS Scheme includes strategies to strengthen collaboration between universal, secondary and tertiary services (that is, Phase One and Phase Two information sharing entities) around a child, to optimise benefits for the child, and to reinforce the contribution of Phase One prescribed workforces. |
In relation to the level of information sharing activity, as there is no systematic reporting of information sharing activity, and there are numerous informal ways to share information, it was not possible to conclude at this time whether the implementation of the CIS Scheme had made an impact on the level of information sharing.
In relation to individual child outcomes, it was too early to say whether the CIS Scheme had made a significant impact. While there were some examples of good practice, the data available did not provide a clear indication of positive outcomes for individual children. However, stakeholders felt confident that the CIS Scheme provides a strong foundation for improved outcomes for child wellbeing and safety.
While the achievement of some early outcomes is promising, stakeholders also provided feedback that the CIS Scheme is not a simple implementation of a policy or program, but rather requires a paradigm shift in the way services consider the needs of the child in their everyday practice. Continued support and education will be necessary to achieve this cultural shift and embed child-focused practice across all sectors of service delivery.
Unintended adverse impacts
Stakeholders who participated in the data gathering activities occasionally raised unintended impacts of the CIS Scheme, which were predominantly either positive or neutral. There were a small number of unintended adverse impacts that relate to perceived disruption to previous workable arrangements for information sharing. Generally, however, the perceived impacts could be considered short term disruption to pathways for information sharing with a view to enhancing the quality and extent of information sharing through a more rigorous and transparent process.
Most stakeholders appreciated that the CIS Scheme augments the information sharing capabilities of information sharing entities. However, the fact that the CIS Scheme augments, rather than replaces, any existing information sharing processes or standards (such as the Child Safe Standards, Mandatory Reporting Requirements or Reportable Conduct Scheme) should continue to be reinforced through ongoing education and communications.
| Recommendation ES 9 Clarifying relationships to other legislation and standards |
|---|
| That consideration be given to providing material to reinforce how the CIS Scheme interacts with other existing legislation and standards, such as the Child Safe Standards, Mandatory Reporting Requirements and Reportable Conduct Scheme, and how these relate to information sharing entities in different sectors, to ensure adherence to the intent of mechanisms available to facilitate child information sharing. Such an approach can highlight where the CIS Scheme provides additional information sharing powers over existing legislation and standards, providing clarity on when and how to use the CIS Scheme. |
While the potential for inappropriate use of the CIS Scheme was a concern raised by stakeholders at commencement of the CIS Scheme, there were no examples of inappropriate use or complaints arising out of implementation of the CIS Scheme encountered during the data collection for this Review. Nonetheless, this continues to remain a risk and the potential for inappropriate use should be actively monitored at organisational and state-wide levels.
Success of prescription of information sharing entities
In considering the impact of the proposed information sharing reforms, it was intended that the phased implementation of the CIS Scheme would involve both government and non-government organisations and align to implementation of the FVIS Scheme to reduce any confusion amongst the workforce and community. The significant overlap of workforces prescribed under both information sharing schemes has provided a logical framework for integrated training but has also highlighted practices that can be strengthened to ensure the successful implementation of the CIS Scheme. Lessons identified by respondents to the follow up workforces survey include reinforcing the importance of routinely gathering accurate information, formalising standards for information collection and developing processes for documenting information sharing occasions and outcomes. Some respondents indicated that they would have liked prescription of information sharing entities to be broader to widen the opportunities for earlier intervention and prevention, however, there was recognition of the increased level of effort that would have been required and the potential for other barriers to have been created to effective implementation.
It could be expected that initial engagement of Phase One information sharing entities in the CIS Scheme will ensure that these services, acutely aware of how unsustainable downstream support is and the impact of entrenched and intergenerational disadvantage, can champion prevention and earlier intervention initially within secondary and tertiary services and ultimately among services operating across the continuum of care. Further support and time is required to ensure that Phase One information sharing entities fully operationalise the CIS Scheme and can work effectively with an expanded CIS Scheme to improve equity of outcomes for children and young people.
Impacts of the CIS Scheme on diverse and disadvantaged communities
The CIS Scheme forms part of a larger toolkit available to information sharing entities to promote the wellbeing and safety of all children in Victoria, with an emphasis on targeted supports for disadvantaged populations. There are a wide range of Commonwealth and Victorian policies, guidelines and frameworks that support the design of services, including workforce knowledge and skills, to respond to the needs of diverse populations with a view to improving access to specialist and mainstream services. Change through service provider policies and practices aims to reduce discrimination, embed cultural responsiveness, foster social inclusive practices, offer healing and trauma informed care and access to language services. It could be expected that the extent of the impact of the CIS Scheme on diverse and disadvantaged communities will be in part a measure of how well the CIS Scheme is utilised and in part reflective of how well services are engaging with diverse communities. The ability to monitor and evaluate the impact of the CIS Scheme on outcomes for diverse and disadvantaged communities will require a more rigorous approach to data collection.
| Recommendation ES 10 Measuring contribution of the cis scheme in responding to the needs of diverse and disadvantaged communities |
|---|
| That CIS Scheme partner government departments consider the adequacy of the current minimum record keeping requirements of the CIS Scheme, including as they inform the role of the CIS Scheme in responding to the needs of diverse population groups. |
| Recommendation ES 11 Engaging diverse and disadvantaged communities |
|---|
| That CIS Scheme partner government departments engage diverse and disadvantaged groups through sector and advocacy peak bodies and information sharing entities, to understand any specific barriers to the implementation of the CIS Scheme and use these findings to assist information sharing entities to overcome these barriers. |
Implementing the CIS Scheme for Aboriginal and Torres Strait Islander communities
While Aboriginal[2] stakeholders consulted as part of this project broadly expressed support for the CIS Scheme, a key issue reported in the successful implementation of the scheme for Aboriginal community controlled organisations (ACCOs) has been barriers related to lack of trust among community members because of the legacy and abiding harm of past experiences relating to child services. There is a need, therefore, to continually educate and reassure families and communities on the objectives and intended outcomes of the CIS Scheme. However, this requires a significant investment of time and effort from the ground up, beginning with the development of culturally appropriate resources for the CIS Scheme.
While stakeholders were cautious about the pace of implementation of the CIS Scheme among Aboriginal organisations and service providers, they were also confident that the CIS Scheme will lead to better outcomes for Aboriginal women and children.
| Recommendation ES 12 Cultural safety |
|---|
| That CIS Scheme partner government departments continue to work with and support the Aboriginal service sector to provide community engagement to ensure Aboriginal communities have a good understanding of the CIS Scheme, and to ensure that cultural safety is taken into account at all stages of using the CIS Scheme. |
| Recommendation ES 13 Culturally appropriate resources to support implementation of the CIS scheme in Aboriginal communities |
|---|
| That CIS Scheme partner government departments work with Aboriginal lead bodies to develop culturally appropriate training and support materials for the effective implementation of the CIS Scheme in Aboriginal communities, both by Aboriginal-specific and mainstream information sharing entities. |
[1] Child Information Sharing Scheme Ministerial Guidelines. Guidance for information sharing entities. State of Victoria, Department of Health and Human Services, September 2018. Available at www.infosharing.vic.gov.au
[2] Aboriginal and Torres Strait Islander people may be also referred to in this report as Aboriginal people
1. Introduction
Introduction to the Child Information Sharing Scheme Two-Year Review report.
1.1 Background
Accountability for child wellbeing and safety
Independent reviews and inquiries conducted in Victoria in the period 2011 to 2016 relating to child safety and wellbeing have consistently highlighted a lack of information sharing among service providers as a significant barrier to effective and timely support for vulnerable families, and especially children[3]. Issues identified have included:
- development of a risk-averse culture to sharing information fostered by the complexity of multiple legislative frameworks
- inability of professionals to obtain a full understanding of a child’s circumstances when information held by other service providers is not shared, potentially delaying a timelier intervention and the possibility of avoided need for secondary and tertiary services
- difficulty in knowing whether a child is participating in universal or targeted services because this information is not readily accessible.
The Victorian Royal Commission into Family Violence (2016) found that an uncoordinated approach to risk assessment and risk management of family violence cases had negative impacts that extended to women and their children. The Commission recommended a specific family violence information sharing scheme and the development of evidence-based risk factors specific to children for inclusion in a revised risk assessment framework.
At a national level, the Royal Commission into Institutional Responses to Child Sexual Abuse (2017) (the McLellan Royal Commission) also found that institutions with responsibilities for children’s safety and wellbeing did not share information with other institutions or organisations or failed to do so in a timely and effective manner. While existing legislation provided for a degree of information sharing to protect the safety of children, barriers to sharing information included complex rules and guidelines, concerns about privacy and confidentiality. A national information exchange scheme was recommended that provides for prescribed bodies to share information and included the establishment of an information sharing scheme within each jurisdiction. Victoria’s Child Information Sharing Scheme is modelled on the recommendations of the McLellan Royal Commission.
Policy context
Consistent with the recommendations of the Royal Commission into Family Violence, the first steps to build a better future for Victorian children, young people and families are set out in the Roadmap for Reform: strong families, safe children. The reforms seek to drive change in the child and family services system that emphasises early intervention, prevention and sharing responsibility. Information sharing is described as a key enabler for other reforms, including the identification of risk factors that are specific to children and the provision of specialist supports and services for children and young people. The Roadmap aims to create services that are coordinated and work together noting that:
…Child protection and family support services are not well connected to universal health and education services. Nor are they well connected to targeted adult services such as specialist family violence, mental health and drug and alcohol services. Poor communication between agencies delays active engagement of, and rapid responses to, families at risk..[4]
The Roadmap reforms complement other key policies in Victoria including the Education State reforms introduced in 2015. These reforms aim to develop a quality education system that is available to all students regardless of their background or circumstances. The Education State Early Childhood Reform Plan is providing targeted support to disadvantaged children in realising a more ‘equitable and inclusive’ early childhood system.
Child Information Sharing Scheme
There are a range of existing information sharing permissions and obligations relating to the safety of children. The CIS Scheme expands the circumstances in which professionals and organisations can share information relating to the wellbeing or safety of children. The CIS Scheme is mandated under Part 6A of the Child Wellbeing and Safety Act 2005 to enable prescribed entities to share confidential information in a timely and effective manner in order to promote the wellbeing and safety of children[5]. Part 6A was proclaimed in September 2018. Prescribed entities are referred to as information sharing entities[6] (ISEs) that are authorised organisations and services including authorised frontline practitioners, specified by the Child Wellbeing and Safety (Information Sharing) Regulations 2018.
Under the CIS Scheme, ISEs are authorised to request confidential information from another ISE, and to disclose information to another ISE, either voluntarily or in response to a request if in their professional judgement they identify that the CIS Scheme threshold is met. The threshold or legal requirements of the CIS Scheme is made up of three parts:
- confidential information is being requested or disclosed to promote the wellbeing or safety of a child or group of children
- sharing confidential information will assist in making a decision, assessment or a plan, and/or the conduct of an investigation, and/or providing a service, and/or managing any risk to a child or group of children
- information being requested or disclosed is not known to be ‘excluded information’ under the Child Wellbeing and Safety Act 2005 (and is not restricted from sharing by another law).[7]
ISEs must comply with requests for information that meet the three parts of the threshold.
Legislative principles in the Child Wellbeing and Safety Act 2005 provide guidance to ISEs in the application of the legislation. The principles include that ISEs should:
- give precedence to the wellbeing and safety of children over the right to privacy
- share information only to the extent necessary to promote the wellbeing or safety of a child, consistent with their best interests
- work collaboratively and respect the functions and expertise of other ISEs
- seek to maintain constructive and respectful engagement with children and their families.
Ministerial Guidelines relating to the operation of the CIS Scheme include how the principles are to be applied in practice by an ISE.
Child information[8] sharing reforms also provide for the establishment of a web-based Child Link Register under Part 7A of the Child Wellbeing and Safety Act 2005, proclaimed in February 2019. The Register is currently under development and will streamline access by authorised professionals to information about participation in government-funded programs of children born in or resident of Victoria.
It is expected that the child information sharing reforms will[9]:
- Improve early needs and risks identification and support, by permitting professional and respectful sharing of information early
- Change a risk averse culture in relation to information sharing, in part by simplifying the legislation
- Increase collaboration and integration between child and family services, promoting shared responsibility across organisations that provide services to children and families
- Support children’s and their families’ participation in services to which they are entitled.
The CIS Scheme operates alongside family violence prevention initiatives introduced for a similar purpose of supporting effective sharing of information between organisations. The Family Violence Information Sharing Scheme (the FVIS Scheme) and the Family Violence Multi-Agency Risk Assessment and Management Framework (MARAM) are provided for under the Family Violence Protection Act 2008. The FVIS Scheme enables information sharing to facilitate assessment and management of family violence risk to children and adults, and the MARAM guides information sharing under both information sharing schemes where family violence is present. Where family violence is believed to be present and a child is at risk, information sharing entities will use the FVIS Scheme to assess and manage family violence risk to both children and adults, as well as the CIS Scheme to share information to promote the child’s wellbeing and/or other aspects of their safety.
Consistent with the recommendation of the McLellan Royal Commission, a phased approach has been adopted to introduction of the CIS Scheme with the intention of minimising the burden of organisational change and maximising organisational readiness. The first tranche of workforces prescribed under the CIS Scheme was proclaimed on 27 September 2018, referred to as Phase One, and comprised approximately 28,000 workers representing around 700 entities primarily within the secondary and tertiary sectors[10]. Phase One information sharing entities generally already had high level permissions to share information about children and families and the impact of extending these permissions under the CIS Scheme was expected to be minimal. Exceptions included services working predominantly with adults such as statutory mental health services, alcohol and other drugs services and housing. Phase Two will extend the CIS Scheme to key primary and universal services in education, health and justice sectors and will commence on 19 April 2021. As for Phase One, this next phase will include information sharing entities prescribed under both information sharing schemes. The Phase Two expansion is estimated to involve an additional 370,000 workers in 7,500 prescribed entities[11].
Governance arrangements for the CIS Scheme reflects a multi-agency approach consistent with the legislative intent and responsibility for the suite of information sharing reforms. Initial oversight for the implementation of the reforms, including the CIS Scheme was provided by the Information Sharing and MARAM Framework (ISMARAM) Steering Committee supported by an Interdepartmental Committee and a Working Group. New governance arrangements came into effect in July/August 2020 disbanding the ISMARAM Steering Committee and establishing the Child Information Sharing Scheme (CISS) Steering Committee. Representation on the CISS Steering Committee, convened by DET, includes DHHS, FSV, DJCS, VicPol, Courts Victoria, Department of Treasury and Finance and Department of Premier and Cabinet. The new arrangement provides a strengthened focus on CIS Scheme implementation for a significantly expanded group of professionals and services in 2021. With disbandment of the ISMARAM Steering Committee, Family Safety Victoria (FSV) has established the MARAM and Workforce Directors Group.
1.2 Purpose of this review
An independent review of the operation and any adverse impacts of the CIS Scheme within two and five years of commencement is required under section 41ZN of the Child Wellbeing and Safety Act 2005. This review represents the two-year review of the CIS Scheme covering the period September 2018 to September 2020.
The two-year review was required to:
- Determine to what extent the CIS Scheme has been implemented effectively.
- Identify key enablers and barriers to implementation.
- Determine to what extent the CIS Scheme is achieving its intended outcomes.
- Consider and identify any adverse impacts of the CIS Scheme.
- Assess the success of the prescription of Information Sharing Entities.
- Assess impacts on diverse and disadvantaged communities.
- Include recommendations (as necessary) on any matters addressed in the review.
1.3 Baseline report
As part of the Two-Year Review, a baseline report was produced for the purposes of assessing any change in information sharing attitudes and practices associated with implementation of the CIS Scheme in the first two years of operation. The baseline report, compiled in the latter half of 2019 and delivered in December 2019, focused on the extent of information sharing among prescribed workforces[12] related to the wellbeing and safety of children and young people prior to introduction of the CIS Scheme. It also considered record keeping systems in place for information sharing and the implementation support provided to prescribed workforces by peak/lead bodies.
As the CIS Scheme had been in operation for approximately 12 months at the time of collecting baseline information, stakeholders were also given the opportunity to provide feedback on their early experience of adjusting to the CIS Scheme.
The key points from the baseline report are provided at Appendix A.
Analysis of data collection from prescribed workforces obtained in the latter half of 2020 focuses on feedback from those who also completed the baseline data collection enabling an understanding of how sentiments and attitudes changed following commencement of the CIS Scheme. Perceived progress, new developments, and any continuing issues for Phase One prescribed entities was also obtained from follow-up consultation with peak/lead sector bodies and key informant government agencies. Further information about the review methodology is provided in Chapter 2.
1.4 Impact of COVID-19
The coronavirus pandemic and associated restrictions to manage the transmission of the virus in Victoria coincided with the final round of data collection for this review. The impact on the community and service providers has been profound affecting service delivery and placing significant pressure on many of the secondary and tertiary services involved in operation of the CIS Scheme that are in the health, human services, justice and police sectors. The review methodology was adapted to accommodate the changed circumstances and the need for a longer research period to enable stakeholder engagement. These changes minimised the impact on engaging stakeholders in the review, with the exception of young people.
However, there has been disruption to initiatives to continue to embed the information sharing reforms into organisations and services while other priorities have required attention[13]. This review also highlights sector concern that the health and economic impact of the pandemic is having a real impact on children and young people that will require a collective response to keep children safe.
1.5 Two-Year Review of the Family Violence Information Sharing Scheme
An independent review of the FVIS Scheme overlapped with this review of the CIS Scheme, both in terms of timing and prescribed organisations and services. The FVIS Scheme review covered the first two-years of operation of the FVIS Scheme which involved an Initial Tranche of entities prescribed in February 2018 and Phase One entities prescribed in September 2018. The review was tabled in Parliament in August 2020[14]. Many of the recommendations of the review, whilst seeking to ensure effective future expansion of the FVIS Scheme, resonate with findings of this review and could be expected to also benefit application of the CIS Scheme by both Phase One and the planned Phase Two prescribed organisations and services. These recommendations address shared issues such as:
- clarifying privacy issues
- monitoring impacts of the information sharing reforms on Aboriginal people to avoid any adverse effects
- providing additional support for the work of Aboriginal organisations to enable appropriate application of information sharing reforms
- ensuring timely delivery of quality training to workforces to be prescribed under Phase Two
- facilitating application of the information sharing reforms through use of case studies
- continuing the information sharing Enquiry Line and sector grants.
It is noted that all recommendations arising from the findings of the FVIS Scheme review have been supported in full or in-principle by the Victorian Government.[15]
Generally, where there was evidence that the subject of these recommendations have or are to be addressed (such as timing of training for workforces to be prescribed, improving understanding of privacy issues), they have not been pursued further in this report as specific recommendations.
1.6 Structure of this report
The review report is structured around the key areas of inquiry set out under the above section 1.2. A series of indicators provided the context for exploring these areas and were set out in an evaluation framework developed for the review. The context guiding discussion of each of the areas of inquiry introduces the relevant chapters.
[3] Includes reports from Victorian Auditor-General’s Office, Commission for Children and Young People and Coroners Court of Victoria
[4] Roadmap for Reform: strong families, safe children. State of Victoria, Department of Health and Human Services, April 2016. p.12
[5] ‘Child’ is defined as a person who is under the age of 18 years and an unborn child that is the subject of a report made under section 29 of the Children, Youth and Families Act 2005 or a referral under section 32 of that Act.
[6] Information sharing entities may also be referred to in this report as prescribed professionals and services, and prescribed workforces.
[7] Child Information Sharing Scheme Ministerial Guidelines. Guidance for information sharing entities. State of Victoria, Department of Health and Human Services, September 2018.
[8] In this report, reference to ‘child information’ is used in the context of sharing information to promote child wellbeing and safety. Information shared may be about an adult or a child.
[9] Child Information Sharing Reform Background and Overview. Department of Education and Training. Victoria State Government.
[10] Department of Education and Training (2019). Child Information Sharing Scheme Regulatory Impact Statement, Amendment Regulations 2020. Victoria State Government.
[11] Ibid
[12] For the purposes of this report, ‘prescribed workforces’ refers to workforces in agencies, organisations and services prescribed under the CIS Scheme
[13] Only 58% of prescribed workforces surveyed in 2020 responded that there was no change to child information sharing as a result of the COVID-19 pandemic.
[14] McCulloch J., Maher, J., Fitz-Gibbon, K., Segrave, M., Benier, K., Burns, K., McGowan, J. and N., Pfitzner. (2020) Review of the Family Violence Information Sharing Scheme Final Report. Report to Family Safety Victoria. Monash Gender and Family Violence Prevention Centre, Faculty of Arts, Monash University.
[15] The Victorian Government response is available at: https://www.vic.gov.au/government-response-review-family-violence-information-sharing-legislative-scheme
2. Methodology
Methodology of the Child Information Sharing Scheme Two-Year Review report.
2.1 Approach
A mixed method approach was applied to this review to obtain information from a variety of new and existing sources about operation of the CIS Scheme in the first two years since commencement of the whole-of-Victorian-government initiative. The review, commissioned by the Department of Education and Training (DET) as lead agency for the CIS Scheme, was conducted by ACIL Allen Consulting in partnership with Wallis Market and Social Research (Wallis).
The approach to the review was underpinned by development of a program logic for the CIS Scheme providing an overview of the key inputs, outputs and expected outcomes of the CIS Scheme (see Appendix B). Alignment of the program logic and the key areas of inquiry for the review underpinned the research questions in the evaluation framework that has guided this review. The framework identified measures and potential sources of information to inform a response to each of the research questions.
Data collection was undertaken predominantly at two points in time with the first commencing in July 2019 (providing input to the Baseline Report) and the second in June 2020. Information gathering focused on establishing attitudes and practices of prescribed workforces to information sharing, the support provided by peak bodies to their respective sectors for effective implementation of information sharing reforms and the extent of change to organisational record keeping processes and systems to facilitate implementation of the CIS Scheme.
Ethics and other research approvals were obtained for engagement with prescribed workforces and planned consultation with young people accessing services provided by information sharing entities under the CIS Scheme. Accessing the views of young people supported by information sharing entities is discussed under section 2.3 relating to limitations of the review.
2.2 Review inputs
Data collection methods included surveys, interviews, virtual workshops, document review and case studies illustrating aspects of implementation of the CIS Scheme. Tools developed for the review included questionnaires, discussion guides and background material to facilitate workshop discussion.
A summary of data collection activities is provided in the following table. A profile of respondents to the workforces surveys is provided at Appendix C. Copies of data collection tools are provided at Appendix D.
| Activity | Stakeholder | Purpose | Participation |
|---|---|---|---|
| 2019 data collection (Wave 1) to inform the Baseline Report | |||
| Surveys | Phase One prescribed ISE workforces drawn from ‘sharers’ and ‘leaders’ who attended training | To explore attitudes and practices related to information sharing prior to commencement of the CIS Scheme | 319 survey respondents |
| Phase One prescribed ISE organisations | To assess the extent of organisational change to systems and processes to enable operation of the CIS Scheme | Senior representatives responding on behalf of 76 government and non-government ISEs providing services in Phase One under the CIS Scheme | |
| Interviews | Key informants | To obtain background about departmental/agency roles and responsibilities in relation to the CIS Scheme |
Department of Education and Training (DET) Department of Health and Human Services (DHHS) Family Safety Victoria (FSV) Department of Justice and Community Safety (DJCS) Victoria Police (VicPol) Court Services Victoria (CSV) |
| Peak/lead bodies | To investigate support for sector implementation of the CIS Scheme and explore sector feedback on information sharing reforms |
Centre for Excellence in Child and Family Welfare Commission for Children and Young People Victorian Council of Social Services Victorian Aboriginal Child Care Agency Cooperative Ltd Council to Homeless Persons Domestic Violence Victoria Victorian Alcohol and Drug Association |
|
| Phase One prescribed ISE workforces | In-depth follow up on questions raised in the workforces survey | 15 respondents, drawn from those who participated in the survey | |
| 2020 follow-up data collection (Wave 2) to inform the Two-Year Review | |||
| Survey | Phase One prescribed ISE workforces | To explore attitudes and practices related to information sharing after commencement of the CIS Scheme |
244 survey respondents of whom 194 participated in the 2019 survey |
| Interviews | Key informants | To obtain an update on departmental/agency roles and responsibilities in relation to the CIS Scheme | DET / DHHS / FSV / DJCS / VicPol / CSV |
| Peak/lead bodies | To update support for sector implementation of the CIS Scheme and sector feedback on information sharing reforms | As for 2019 data collection | |
| Virtual workshops | Phase One prescribed ISE organisations and services | To share experiences of implementing the CIS Scheme, discuss the outcomes and benefits of the CIS Scheme and explore future collaboration to further strengthen implementation of the CIS Scheme | Two workshops attended by a total of 19 participants from two government organisations (representing five different business units) and representatives from 11 non-government organisations delivering government funded services across both regional and metropolitan locations. Services represented included Child Protection, out-of-home care, integrated family services, Child FIRST, Maternal and Child Health, mental health, alcohol and other drugs services, homelessness services, specialist family violence services, victim support services, youth justice and Births, Deaths and Marriages |
Source: ACIL Allen Consulting 2020
To the extent appropriate, quotations used in this report and drawn from qualitative feedback provided as part of the surveys of prescribed workforces may include identification of the respondent’s workforce category to provide additional context.
2.3 Limitations
The review methodology has been adapted to accommodate scheduling changes related to roll out of the CIS Scheme and the impact of the coronavirus pandemic on Phase One prescribed organisations and services.
Establishing a baseline
A key component of establishing a baseline related to information sharing was the survey of prescribed workforces. Recruitment of workforces to this research was linked to their online registration for initial training related to the information sharing reforms. Workforces were surveyed for baseline attitudes and practices approximately 10 months after the CIS Scheme had been proclaimed, in part due to a delay in commencement of training. To accommodate this timing, survey respondents were asked to consider their attitudes and practices to information sharing 12 months previously, prior to introduction of the CIS Scheme.
Workforce survey sample
There are two possible areas of limitations caused by bias in the sample of workforces participating in the 2019 and 2020 surveys, namely non-response bias among the survey sample and sample bias. Non-response bias, where those responding to the survey invitation fundamentally differed from the overall population, is likely to have been mitigated as a serious source of bias by the relatively high response rates achieved and the use of the multi-modal approach (option for participants to complete the survey by telephone or online). In relation to sample bias, as the sample of workforces opted in to the research, they could be considered more engaged with the CIS Scheme. While the likelihood of this phenomenon occurring has not been measured, it is expected that it would be limited in nature.
Progressive feedback from prescribed organisations and services
Early feedback on implementation of the CIS Scheme was intended to be captured late in 2019 through roundtables involving prescribed organisations and services, including representation from those entities expected to have been prescribed under Phase Two. Other priority consultation on the information sharing reforms at that time and deferral of prescription of Phase Two entities until 2021 due to the coronavirus pandemic made this approach impracticable. Consequently, it was agreed that the planned workshops in 2020 would be augmented to provide increased opportunity for Phase One prescribed organisations and services to access this review. In the event, the impact of the coronavirus pandemic influenced stakeholder ability to participate and required the conduct of virtual workshops. Three workshops were offered and two were conducted in early August 2020.
Including the views of young people
Attempts as part of this review to provide an opportunity to hear from young people about their experiences of sharing their information were unsuccessful. This included a direct approach to eligible ISEs in the 2019 data collection period and an approach through the Centre for Excellence on Child and Family Welfare’s sector e-newsletter inviting services to obtain further information should they be willing to assist in the recruitment of young people for the 2020 data collection. The lack of response from ISEs can in part be attributed to the demands on sector resources, which were intensified in the latter part of the review during the coronavirus pandemic, and a reluctance to engage their clients in research activity.
While it has not been possible to include the voice of the young person in this research, some of the emerging benefits of the CIS Scheme are illustrated.
However, a focus on the experiences and perspectives of children and young people is even more appropriate for the subsequent five-year review of the CIS Scheme when it has become better embedded in workforce practice and its potential to support earlier intervention and prevention is realised. Future consideration could be given to support for collaboration with a selection of prescribed organisations and services and the independent reviewer for annual consultation with young people through focus groups or interview about the way in which they experience information sharing and any ways in which this experience might be improved. There may also be potential to identify ISEs who are implementing or who would agree to implement good practice record keeping (as described in the Ministerial Guidelines) when disclosing information by recording additional details about what the views of the child and/or relevant family member were about information sharing. With appropriate research approvals, this information could be reviewed for any common themes.
3. Implementation of the Child Information Sharing Scheme
This chapter addresses the following research question:
How effectively has the CIS Scheme been implemented to date?
In determining effectiveness of implementation, consideration has been given to:
- greater clarity about the circumstances in which child information can be shared
- legislative requirements for the CIS Scheme are embedded in the guidelines and processes of ISE organisations and services
- ISE workforces are prepared to consider opportunities to share child information
- ISE organisational systems facilitate retrieval, storing and recording of information under the CIS Scheme
- ISE systems and processes support monitoring of implementation of the CIS Scheme
Box 3.1 Key findings – CIS Scheme Implementation
Workforce capability
- Initial state-wide roll out of an intensive training program for Phase One prescribed workforces related to the information sharing reforms was attended by approximately 2,000 participants.
- The initial training served to create an awareness of the reforms within three months of their commencement.
- Additional training was provided by relevant government departments tailored to their respective workforces.
- Follow up support for Phase One implementation is ongoing and includes a range of learning resources and an enquiry line. There have been more than 6,000 registrations for online training.
- FSV grants to relevant peak/lead bodies have been important to extending the reach and understanding of the information sharing reforms among diverse sectors and workforces with varying experience of child-focus practice.
- Stakeholder feedback suggests there is continuing need to upskill prescribed workforces in the legislative provisions and requirements of the CIS Scheme to support effective implementation across the information sharing entities.
Consistent practice
- Further work is required to support a consistent and informed level of understanding of the threshold for application of the CIS Scheme.
- There is evidence of improved workforce attitudes to child information sharing since commencement of the CIS Scheme and preparedness to share information.
Record keeping
- While organisational policies are in place to support workforces in implementing the CIS Scheme, there may be a low level of compliance with the record keeping obligations in the Child Wellbeing and Safety (Information Sharing) Regulations 2018 and explained in the Ministerial Guidelines.
Source: ACIL Allen Consulting 2020
3.1 Greater clarity about when child information can be shared
3.1.1 Phase One prescribed workforces
As indicated at Appendix E, the majority of the Phase One organisations and services are prescribed under both information sharing schemes and the MARAM Framework. Depending on the circumstances, Phase One prescribed workforces may use either of the information sharing schemes on their own or apply both schemes where family violence is present and there are wellbeing and other safety concerns for the child/children.
As discussed under section 1.1, under the relevant information sharing scheme, prescribed workforces are authorised to request and voluntarily disclose confidential information from another prescribed entity where thresholds are met, and are required to disclose confidential information in response to a request from another prescribed entity where thresholds are met.
3.1.2 Workforce training
Impact of initial state-wide face-to-face training
Initial training related to implementation of the CIS Scheme was conducted for Phase One prescribed workforces over a ten-week period during October – December 2018. Development and delivery of the training was overseen by FSV and DET, with DET as lead. The training approach was informed by a needs analysis and the deliberations of a Child Information Sharing Working Group with membership from relevant areas of government, and consultations with a Training and Practice Advisory Group (TPAG) with expertise across relevant workforces. DHHS was part of the initial training development work and played a critical part in the TPAG. A set of principles were established for the design of the training including the adoption of an integrated approach that would cover content for both information sharing schemes and an introduction to the MARAM Framework. The training was developed by DET and FSV with support from Swinburne University and delivery across Victoria of the two-day face-to-face training was led by Box Hill Institute. The purpose of the initial training was to establish a minimum level of capability related to the information sharing reforms across workforces, coinciding with commencement of the schemes.[16]
A total of 35 training sessions were conducted across 25 locations in metropolitan and regional areas of Victoria. The training was attended by just under 2,000 participants, 35% of whom attended regional sessions. Highest attendance came from the areas of Family Services, Alcohol and Other Drugs Services, Maternal and Child Health and Mental Health Services, representing 43% of participants. Based on a workforce needs analysis a training target for Phase One information sharing entities had been estimated at approximately 4,000 workers.[17] Unmet demand was met by tailored partner departmental training programs and online training registrations. For example, training created by DHHS to meet demand amongst the DHHS workforces commenced in May 2019 and trained over 1,000 people by October 2019.
An evaluation of the initial state-wide training approach included a post survey (response rate of approximately 73%) of the impact of training on participant understanding of, and confidence to implement the information sharing reforms. As set out in the Training Evaluation Report, key findings of the evaluation and key learnings included:
Key findings (based on the post training evaluation survey)
- The training overall was rated from Medium to High by 77% of respondents with a further 7% rating it as Very High. 11% of respondents rated the training as Low.
- Following the training:
- a majority of respondents rated their understanding of the CIS Scheme as High (51%) to Very High (8%) with a further 35% recording a rating of Medium
- a majority of respondents rated their confidence to share child information under the CIS Scheme as High (45%) to Very High (10%) with a further 35% recording a rating of Medium
- these ratings were highly consistent with those given to their understanding of, and confidence to share under the FVIS Scheme.
Key learnings
- participants valued:
- the opportunity to develop their understanding of how to collaborate with other sectors
- contextual detail to support following the Ministerial Guidelines for the information sharing schemes
- practical application of the reforms
- issues identified by participants included:
- time spent covering information that could have been prescribed as pre-reading
- a preference for more time spent on case studies, role playing and networking
- a lack of information about ongoing support to reduce any anxiety about implementation in practice, such as links to resources and change management plans for specific workforces.implementation support for Phase One prescribed workforces
Ongoing implementation support for Phase One prescribed workforces
Government support for implementation
While participants expressed mixed views about the extent to which the initial training met their expectations, lead agencies driving the reforms considered that the initial intensive training had served to create an awareness of the CIS Scheme (and related reforms) within three months of its launch. DET and partner government departments were able to build on this awareness and refine the strategic approach to building capacity among the Phase One prescribed workforces. This included the development of training by relevant government departments that were tailored to their workforces, and support for peak bodies to develop sector specific supporting materials and resources to facilitate effective implementation of the information sharing schemes.
A range of other supports to guide practice and enable self-directed learning relating to the CIS Scheme have been progressively developed and enhanced, generally through an integrated approach. This approach reflects the overlap of workforces prescribed under the information sharing schemes, the potential for both schemes to be applied in individual circumstances and the need for a clear understanding of the different purposes of the schemes. Whole-of-Victorian Government implementation supports for the CIS Scheme that are available to Phase One prescribed workforces are provided predominantly through a variety of DET platforms and include:
- eLearning modules available as online courses, with over 6,000 enrolments to date
- dedicated child information sharing website with online resources including checklists, factsheets and templates
- Ministerial Guidelines that are legally binding for prescribed entities and explain how confidential information should be handled under the CIS Scheme and the legislative principles that underpin operation of the Scheme
- ISE list on a searchable database that assists ISEs to identify other organisations prescribed to share information under the schemes in compliance with their legislative responsibility
- dedicated Enquiry Line and email Inbox for child information sharing queries
- email inbox for queries related to the whole-of-government Learning Management System (LMS) that hosts the online training for information sharing
The Enquiry Line and inbox have been open to Phase One prescribed organisations and services since commencement of the CIS Scheme in September 2018. This is a shared resource available also to respond to queries related to the FVIS Scheme and MARAM. The following figure presents the number of all enquiries through both telephone and email from January 2019 to October 2020.
Figure 3.1 Enquiries through the Information Sharing Reforms dedicated enquiry line (phone) and inbox (email)
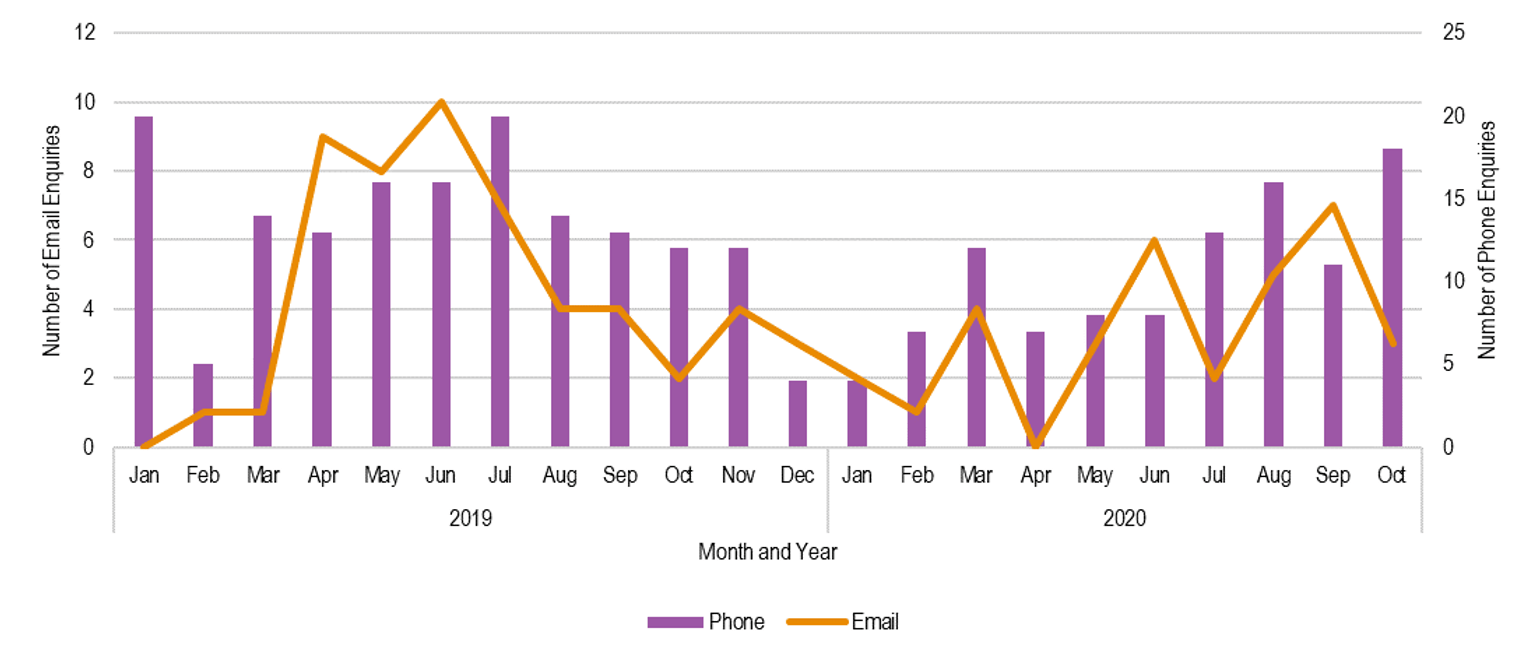
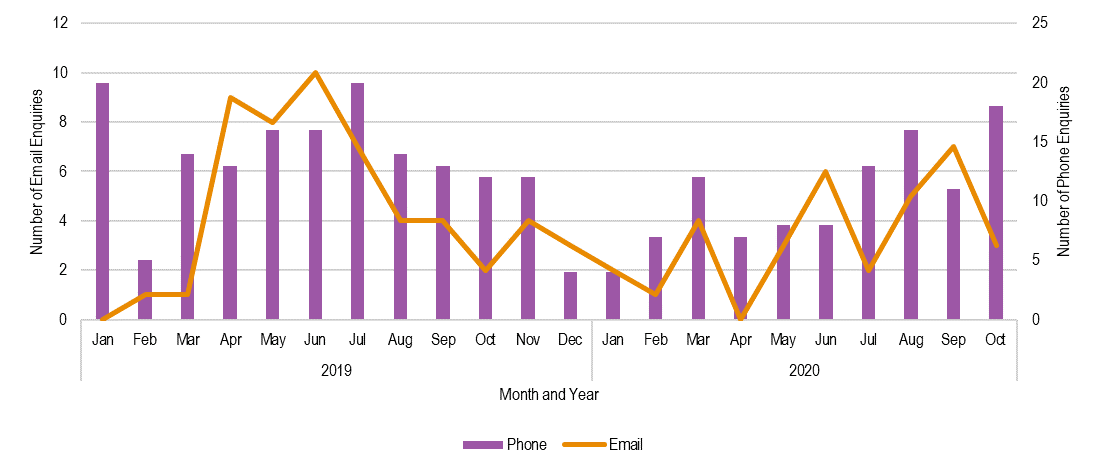{kind=link}
Based on data collected about telephone calls and emails to the Enquiry Line over this period, the average number of monthly contacts decreased after a peak in July 2019 and remained relatively steady until the middle of 2020, most notably for telephone calls. This trend suggests that Phase One ISEs have an increasing understanding of the information sharing schemes but may also be a response to awareness of, and access to a wider range of resources. Over the period January 2019 to June 2020, enquiries have most commonly (92%) sought information to verify ISEs, seek policy guidance, access training or resources and seek practice guidance. Enquiries categorised as policy questions have related to obtaining consent to share, who information can be shared with and sharing of perpetrator information. Practice guidance has related to assistance in determining threshold for sharing information, extent of information sharing and action available when a request to share is refused.
From mid-2020, there has been an increase in contact to the Enquiry Line across both mediums (see Figure 3.1). Anecdotal evidence from DET suggests that this increase has been related to Phase One ISEs seeking information on the timing and scope of Phase Two implementation and how they may have to respond to that implementation. Approximately 60% of all queries related to the CIS Scheme, suggesting that the Enquiry Line will continue to be a valuable source of support for ISEs. The following table provides a breakdown of the queries by area of enquiry (see Table 3.1).
| Area of enquiry | Proportion of enquiries (%) |
|---|---|
| Both CIS and FVIS Schemes | 39% |
| FVIS Scheme only | 29% |
| CIS Scheme only | 11% |
| CIS Scheme, FVIS Scheme and MARAM | 10% |
| MARAM only | 7% |
| Other | 3% |
| Does not add to 100% due to rounding | |
| Source: ACIL Allen Consulting 2020, based on data provided by Department of Education and Training Jan 2019-June 2020 | |
In addition, there is a dedicated inbox for queries in relation to the whole-of-government LMS. The following figure presents the trends in relation to queries regarding access to online training through the LMS.
Figure 3.2 Email enquiries in relation to online training through the LMS
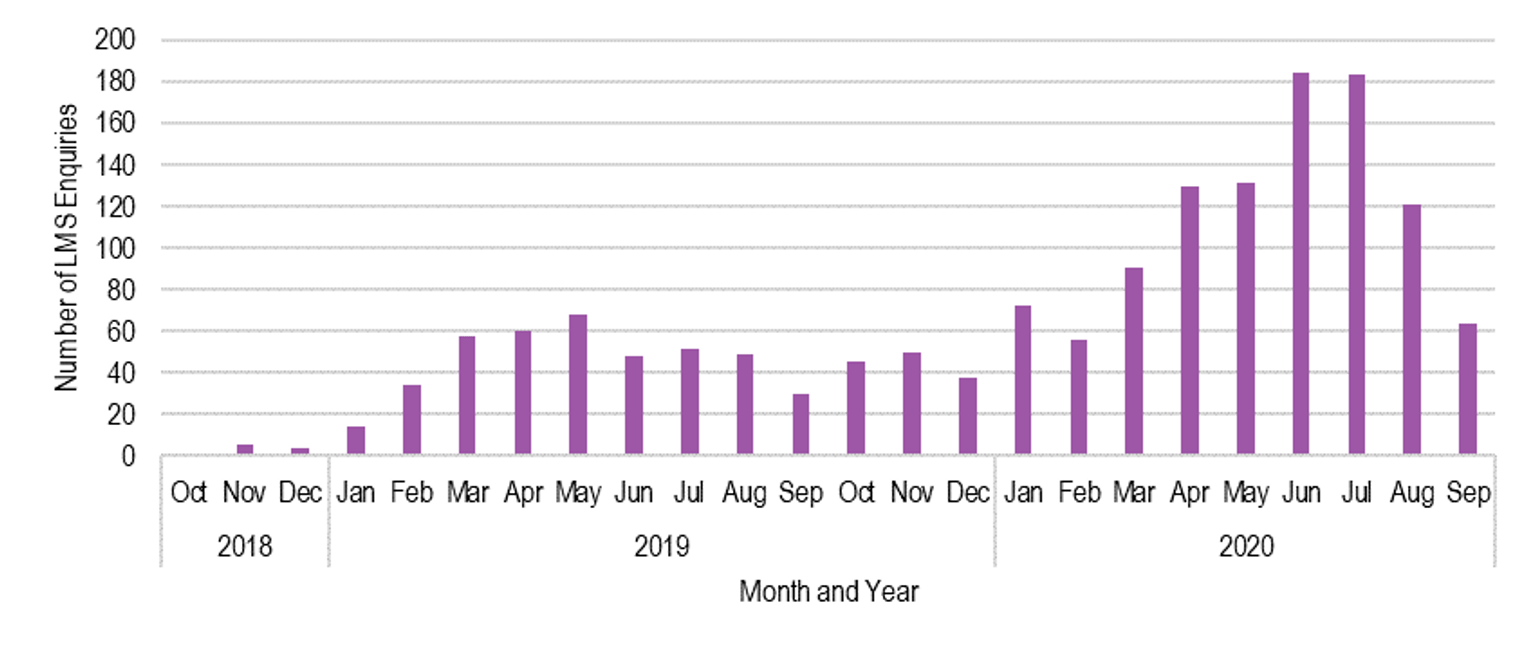
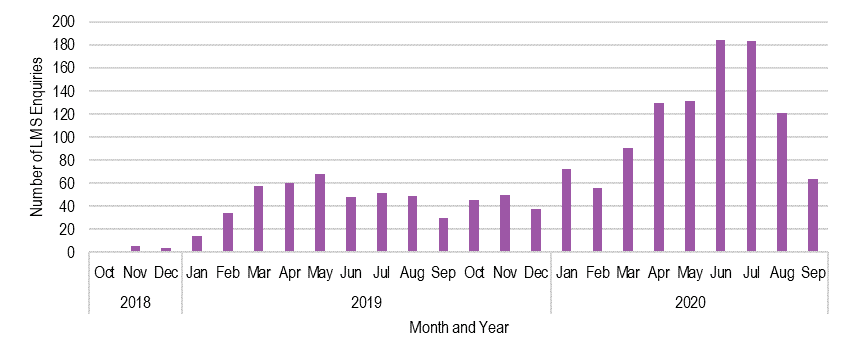{kind=link}
Enquiries in relation to online training peaked in the middle of 2019 and remained steady until March 2020, where it increased more than threefold, peaking in June and July 2020 before declining (see Figure 3.2). This increase, according to other data provided by DET, reflected a similar doubling in the number of registrations for online training. It is likely that this increase in online training was due to workforces who were required to work from home during the coronavirus pandemic restrictions having more time to participate in training.
Enquiry Line and LMS inbox will continue to be available to Phase Two workforces when they are prescribed in 2021. Given the recent increases in 2020, it may be important to understand the capacity of the team to handle enquiries as Phase Two is implemented, as it appears both Phase One and Two workforces require assistance to implement Phase Two of the CIS Scheme. It is noted that the Two-Year Review of the Family Violence Information Sharing Scheme recommended that the hours of operation of the Enquiry Line be extended and that it be fully resourced for at least two years following commencement of Phase Two of the information sharing schemes.
In addition, the DET Enquiry Line could be harnessed to provide a better understanding in real time of the nature and proportion of enquiries related to the CIS Scheme and the category of information sharing entity seeking clarification. This information could inform monitoring of the implementation of the CIS Scheme and any gaps in understanding at workforce and service level that might warrant targeted or different support.
| Recommendation 1: Enquiry line data collection |
|---|
| That operation of the Enquiry Line be funded to accommodate the expansion of information sharing entities under the information sharing reforms, and to facilitate the collection of ‘real time’ data to inform effective implementation of the child information sharing reforms. |
Sector Grants Program
The FSV Sector Grants Program, introduced in 2017-18 has provided sector implementation support funding to key representative and state-wide bodies for implementation of the information sharing and MARAM reforms. In 2020-2021, grant funding of $1.5 million was allocated to projects delivering tailored initiatives to key workforces relating to all three reforms. Suggested targeted areas for project proposals had included awareness raising, practice guidance and up-skilling of information sharing and family violence risk assessment and management change champions within organisations[18]. Sector Grants have been accessed by peak/lead bodies including the Centre for Excellence in Child and Family Welfare, Municipal Association of Victoria, Council to Homeless Persons, Victorian Alcohol and Drug Association and the Victorian Aboriginal Child Care Agency. There has also been collaboration across peak bodies to address the need for a common language to facilitate clarity around information sharing requests. The work of the peak/lead bodies has been an important avenue for promotion of the information sharing schemes and specifically for addressing the level of change needed in some sectors and programs where there has been little exposure to accounting for the wellbeing of children. Peak bodies are well placed for engaging their respective sectors in the development of resources that draw from the experiences of service providers and facilitating cross-sector collaboration.
The Sector Grants Program focuses on implementation of the information sharing reforms in a family violence context. Whilst the activities supported by the FSV grants have benefited operation of the CIS Scheme, peak/lead bodies have not had the resources to bring a similar focus to the CIS Scheme and its wider application. Feedback from peak bodies indicates that there is continuing work to successfully embed the CIS Scheme in prescribed organisations and services, including current planned activity. While the immediate priorities of the coronavirus pandemic have interrupted some of this work, the present and predicted health and economic consequences of the pandemic have highlighted the importance of services having the tools to enable best practice in acting early to foster the wellbeing and safety of children.
… Living through a pandemic has required us to change and adapt to challenging circumstances. For those of us working in the child and family services sector, it has meant being innovative in the ways we work with families to keep children visible and safe.
… this pandemic has thrown a spotlight onto current stressors and weaknesses in our service responses and on existing social and structural inequalities and disadvantage. What is clear is that we have a steadily growing group of children and families that need help.
… This means changing our focus from a crisis response to a whole-of-family approach that works to support families to keep children safe and to access the services they need…
Child Protection Week, Let’s not ignore the long term impact of COVID-19 on children. Deb Tsorbaris, CEO Centre for Excellence in Child and Family Welfare. September 2020
The FSV Sector Grants Program has demonstrated the value of supporting targeted initiatives for key workforces in promoting effective implementation of reforms. There is opportunity to better leverage the support of peak/lead bodies in complimenting other efforts to promote early intervention and prevention through improved child information sharing. This support would be especially timely in also facilitating collaboration between peak/lead bodies representing sector workforces prescribed in Phase One of the CIS Scheme and proposed for Phase Two. A similar model to that implemented by FSV for promoting sector capacity building through the formation of working groups in which sector grants recipients are expected to participate could be considered for CIS Scheme sector capacity building[19].
| Recommendation 2: Sector support |
|---|
| That support be provided to sector peak/lead bodies, similar to the Family Safety Victoria sector grants, to strengthen the response to sector-specific needs of information sharing entities in understanding and applying the CIS Scheme in a range of circumstances and to promote cross sector collaboration and consistency. |
Perspectives of prescribed workforces
Feedback in 2020 through open-ended questions in the follow up workforces survey and workshops with prescribed organisations and services, suggests that CIS Scheme training and supporting resources continues to be a priority issue for prescribed organisations and services.
While many organisations have developed training for staff that links to changes to policies and procedures aligned to the requirements of the CIS Scheme, there are a range of challenges to effective implementation of the CIS Scheme that include:
- Not all staff within information sharing entities have been trained potentially limiting operation of the CIS Scheme as intended and achieving the aims of extending permissions and supporting early intervention.
As an organisation it is taking time for us to develop our internal documents/policies and for staff to have adequate time and support to implement the required changes in practice and recording. (Maternal and Child Health (MCH) workforces survey respondent).
Agencies need to continue to drive this over time, not a set and forget; would have more momentum in the beginning and now it seems to have slightly dropped off. Been more of a push with information and training posted online, need to leverage this to keep momentum going. (Workshop participant).
Requires a lot more persistence to embed these changes. (Workshop participant)
- Interactions with other information sharing entities has demonstrated a lack of understanding of the CIS Scheme which appears to reinforce the importance of training in both creating an awareness of the CIS Scheme and understanding of its provisions
We were advised by family services staff that they could not discuss any of their clients without seeking client permission. We find we are still needing to educate family services of the need to share information for the benefit of the carer and child. (MCH workforces survey respondent)
- Continuing challenges in interpretation of ‘wellbeing’ associated with use of the CIS Scheme which suggests a lack of confidence in the capacity for professional judgement in determining application of the CIS Scheme and highlights the varied familiarity of prescribed entities with child-focused practice frameworks.
Many workforces are uncomfortable with the breadth of the term ‘wellbeing’. There is a lack of a framework like MARAM for the FVIS Scheme to guide interpretation of wellbeing for the CIS Scheme. (Workshop participant)
The CIS Scheme Ministerial Guidelines provide guidance on determination of the threshold relating to promotion of child wellbeing and safety, recognising the practice and human rights frameworks that might influence decision making and identifying that the concept of wellbeing is broader than safety alone extending to support for good health, positive relationships and age appropriate learning and development. Feedback from key informants reinforces the importance for different workforces to respect and adapt to how other workforces perceived and understood wellbeing (consistent with the legislative principles for the CIS Scheme), particularly as it relates to early identification and intervention to improve the wellbeing of children. It was considered necessary to balance the original intent of the legislation regarding the importance of the breadth of circumstances relevant to wellbeing, while providing additional guidance to workforces on how they should assess and understand wellbeing for the purposes of the CIS Scheme. This may include developing additional material/guidance that may contribute to a professional’s understanding of the promotion of a child’s wellbeing without narrowing the definition of wellbeing.
While the workforces to be prescribed under Phase Two have a working familiarity with wellbeing frameworks in their capacity as wellbeing/child focused services, the same does not apply to Phase One prescribed workforces that operate primarily with a risk focus and an adult user group. The continuing concern of many Phase One prescribed workforces about the need for additional support in assessing the threshold for ‘wellbeing’ in the context of the CIS Scheme should be investigated in order to ensure a consistent interpretation that accords with the intent of the legislation and to remove any barrier to effective implementation. Other strategies to build professional skills and confidence in this area might also be considered as part of cultural change to improve child information sharing including sectoral and organisational leadership on ‘professional judgement’.
| Recommendation 3: Assessing threshold for ‘wellbeing’ |
|---|
| That further guidance be provided for prescribed workforces regarding expectations associated with ‘promoting child wellbeing’ under the CIS Scheme. That this further guidance be informed by an audit of state-wide and sector specific resources with the aim of identifying guidance gaps, particularly in relation to promoting a shared understanding of child wellbeing and risk thresholds, and child and family service system roles and responsibilities in relation to child wellbeing. |
There is support for ‘refresher learning’ to maintain momentum and consolidate learning and knowledge to support implementation of the CIS Scheme. There is also recognition of the value of extending lessons from Phase One collaboration to facilitate operation of the CIS Scheme with the broader cohort of information sharing entities to be included in Phase Two:
Prescribed workforces from Phase One may need a top-up of training to deal with different types of organisations in Phase Two that have a different way of working. (Workshop participant)
| Recommendation 4: Strengthening capacity of Phase One workforces |
|---|
| That change strategies and ongoing training of information sharing entities related to the information sharing reforms continue to develop capacity among Phase One prescribed workforces and to facilitate integration of practice between Phase One and Phase Two prescribed workforces. This could be facilitated through workforce forums developed in collaboration with peak/lead bodies, and through support for local and place-based networks across sectors and promotion of local champions. |
3.2 Embedding CIS Scheme in polices and guidelines
Given the complexity and legislative requirement for implementation of the CIS Scheme it has been important for prescribed organisations and services to ensure that internal policies and guidelines support their workforces in the appropriate sharing of information. Workforces responding to both the 2019 and 2020 survey of attitudes and practices related to the CIS Scheme indicated that for a large majority (84%) their organisation had policies covering the sharing of children’s information with external organisations at the time of the follow up survey in 2020 (see Figure 3.3). This represented an increase from 68% of this cohort who reported in the baseline survey about information sharing policies in place prior to commencement of the CIS Scheme.
Figure 3.3 Proportion of workforces indicating their organisation had policies covering CIS prior to and following commencement of the CIS Scheme
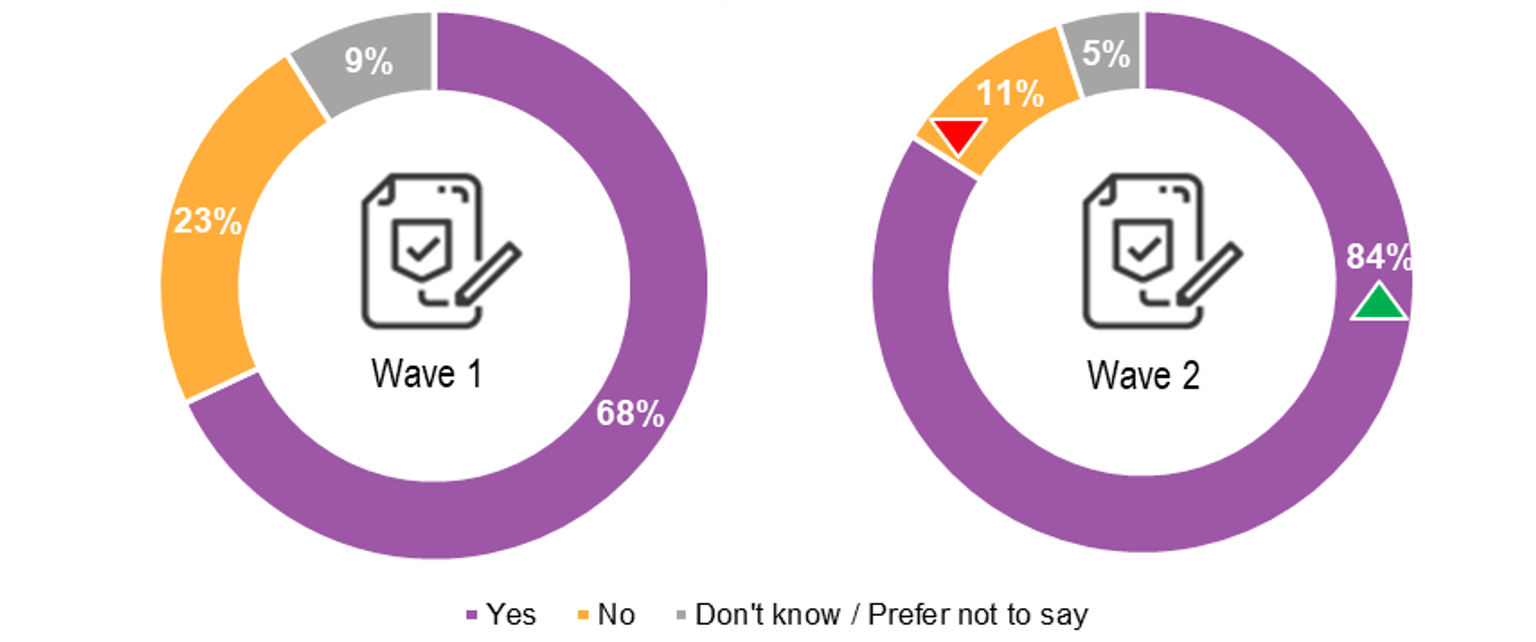
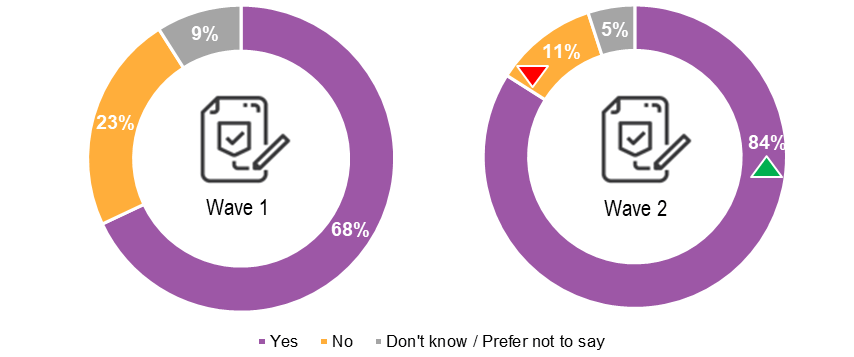{kind=link}
Looking at how the organisational policies changed after the implementation of the CIS Scheme, there is generally an improvement in workforce perceptions of the policies. Among those survey respondents who identified that their organisations did have policies on sharing child information prior to commencement of the CIS Scheme (2019 baseline), there was mixed perceptions of the policies’ currency and value in enabling information sharing (see Figure 3.4). Change at follow up, however, included a larger proportion of respondents reporting that the policies were up to date (85%, an increase from 65%), are sufficiently flexible and provide clear guidance on permission to share. There is a reduction in the perception that policies sometimes hinder early identification of needs or prevention of issues. Curiously, there is a small decrease in the proportion of respondents who perceive that policies are adhered to by relevant staff suggesting that further work is required to ensure all relevant staff have the knowledge and skills for child information sharing.
Figure 3.4 Workforce perceptions of information sharing policies
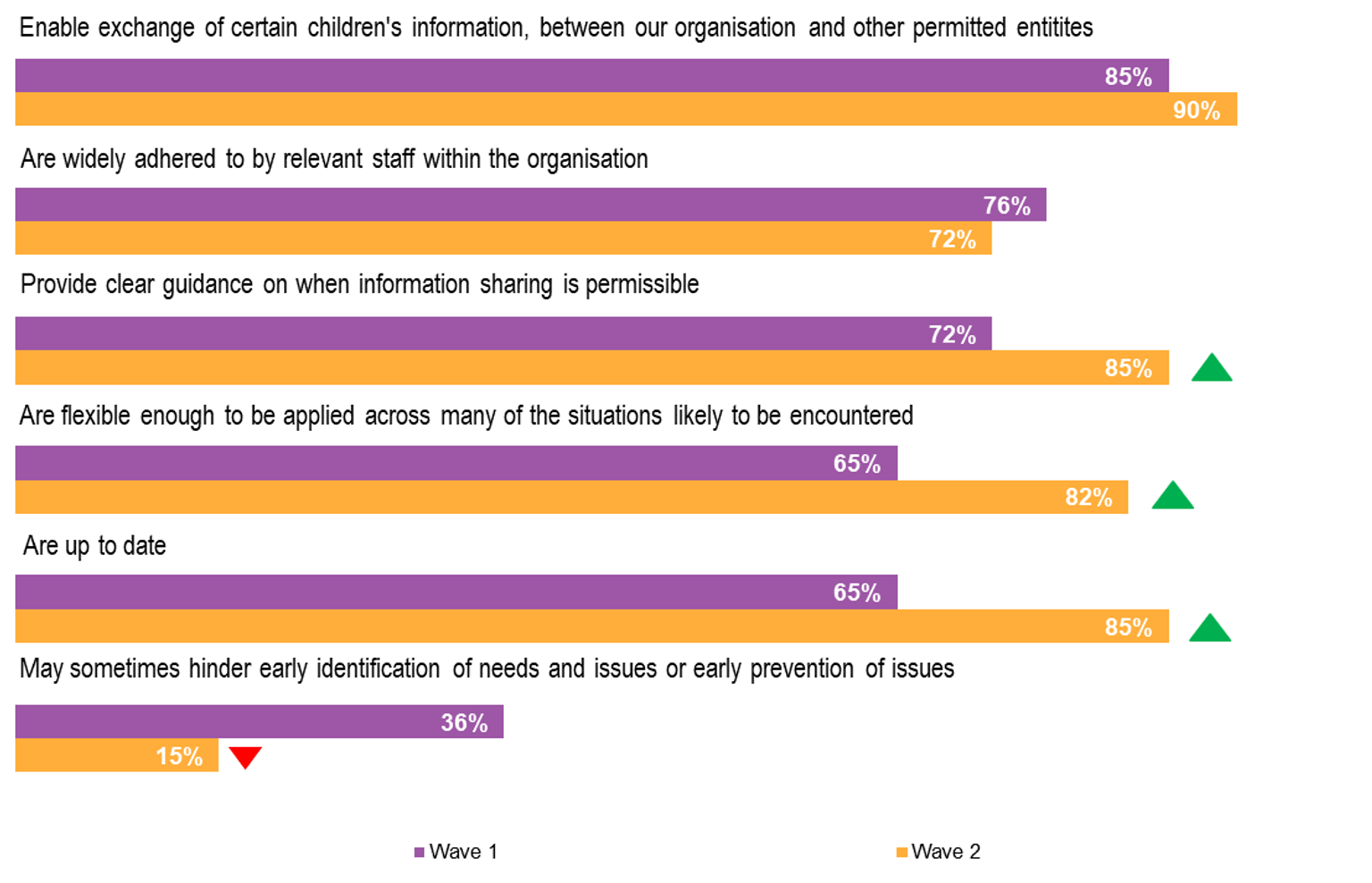
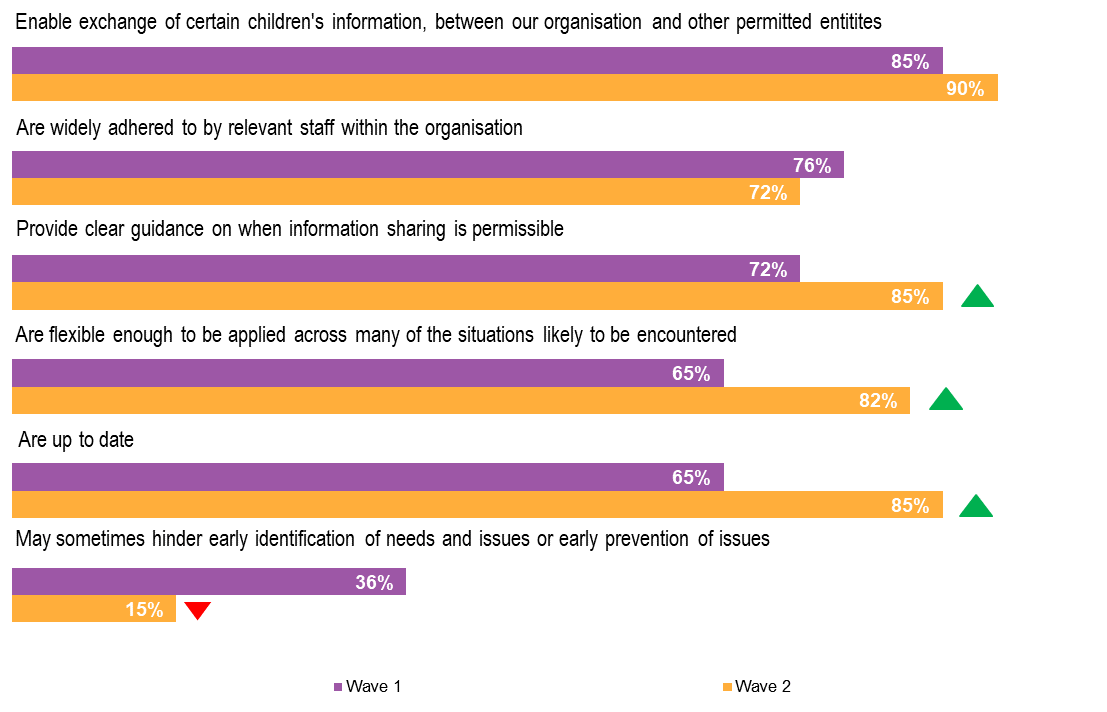{kind=link}
Comparing the results of those who answered in the 2020 follow up survey only (n=50) and those who answered in both 2019 and 2020 surveys (n=194), while not significantly different, there were fewer respondents in the follow up survey only (68% compared to 82%) who agreed that the policies ‘were flexible enough to be applied across many of the situations likely to be encountered’.
3.3 Preparedness to consider opportunities for child information sharing
Asking workforces how they perceived staff attitudes at their organisation in the 12 month period up until the commencement of the CIS Scheme in September 2018, while the majority (83%) felt that their organisations were generally open to sharing information with other agencies within the legal frameworks and that the organisations understood how information sharing could benefit children (89%), this increased after the implementation of the CIS Scheme to 90% and 91% respectively (see Figure 3.5).
Similarly, while prior to commencement of the CIS Scheme 74% of survey respondents reported that they were aware of their legal responsibilities and even fewer, 67%, knew where to go for guidance on how to share information, at follow up this had increased to 83% who were now aware of their legal responsibilities and 85% who now knew where to go for guidance.
Prior to the implementation of the CIS Scheme, only 27% of respondents felt that there was reluctance in the organisation to share information. After the implementation of the Scheme, fewer (21%) respondents felt this way. The response from workforces who completed the survey in 2020 only was more marked with only 10% feeling reluctant to share information because they may be doing the wrong thing.
Figure 3.5 Workforce attitudes towards information sharing
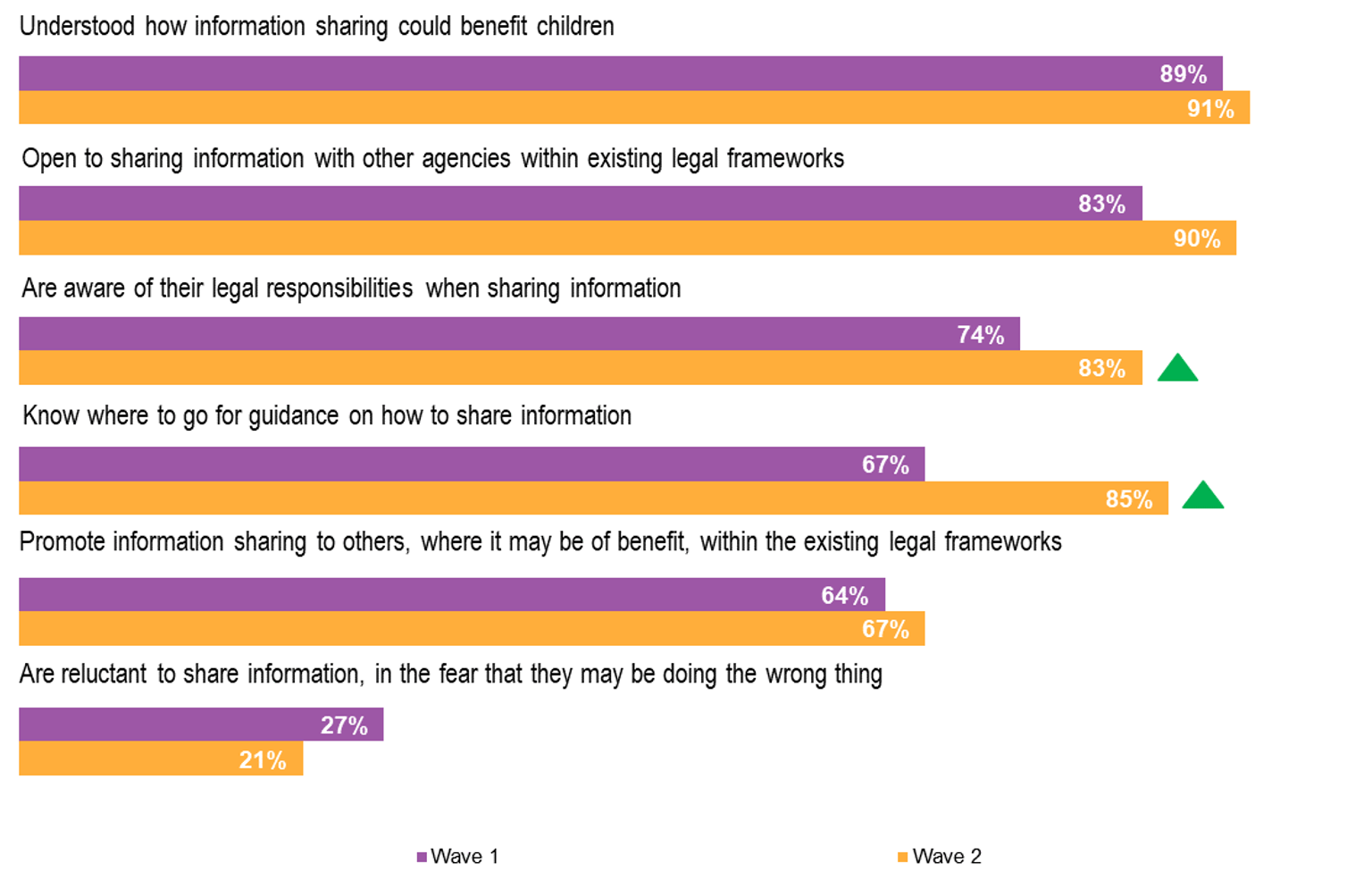
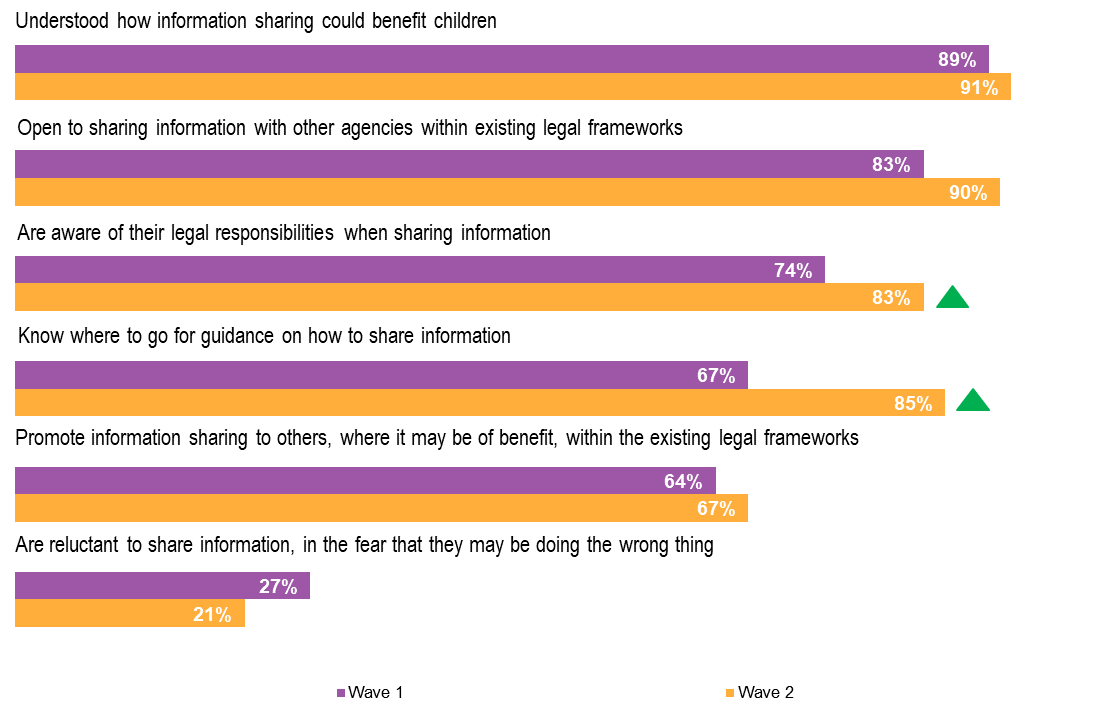{kind=link}
While there are positive indications of an improved level of workforce understanding of, and receptiveness to information sharing, there is a continuing conservative position regarding willingness to promote information sharing where it may be of benefit. This position supports stakeholder feedback about the evolving nature of the culture change that needs to occur and the further work to be done to embed the CIS Scheme in practice. (Also see section 4.3 and section 5.2.)
3.4 ISE systems and processes support monitoring of implementation of the CIS Scheme
Information sharing entities were expected to leverage their existing systems to meet the record keeping requirements under the CIS Scheme. A selection of prescribed organisations and services were asked about whether there had been a need to make changes to their record keeping systems in anticipation of, and subsequent to introduction of the CIS Scheme.
Nearly three-quarters (74%) of organisations (n=54) indicated that changes had been made to record keeping arrangements in response to the CIS Scheme (see Figure 3.6). This was made up of over one-third of organisations who indicated that changes to processes had been made both before and after the introduction of the CIS Scheme, while a smaller proportion had made changes only before or only after implementation.
For some organisations, changes made in anticipation of the CIS Scheme were ongoing after introduction of the CIS Scheme. For other organisations additional changes were made following introduction of the Scheme.
Figure 3.6 Proportion of survey respondents by changes to organisational record keeping before and after implementation of the CIS Scheme
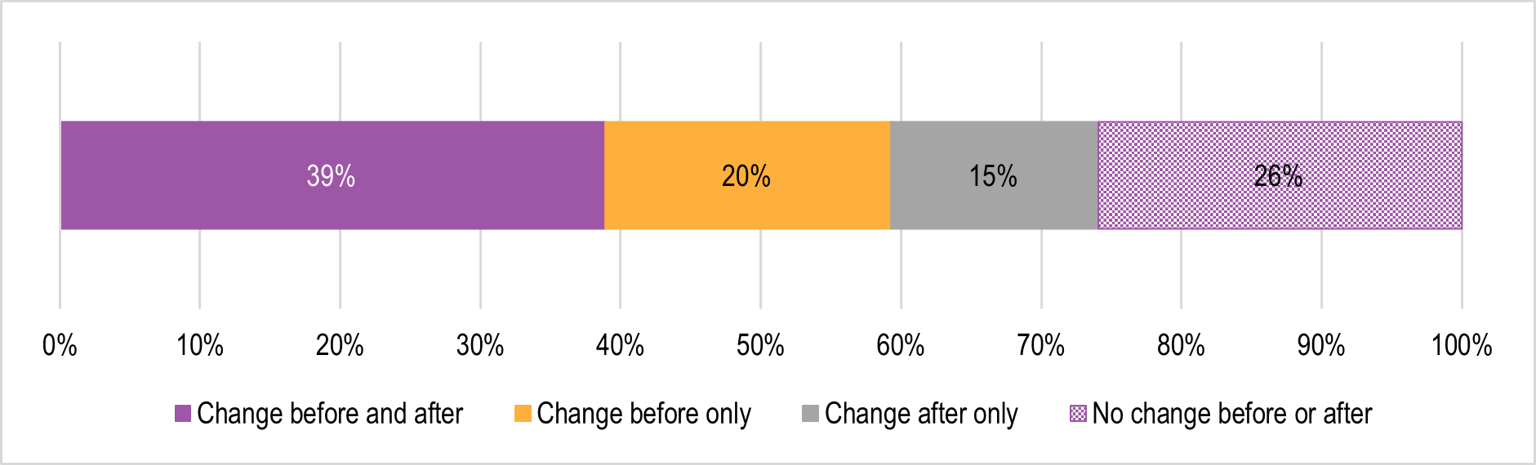
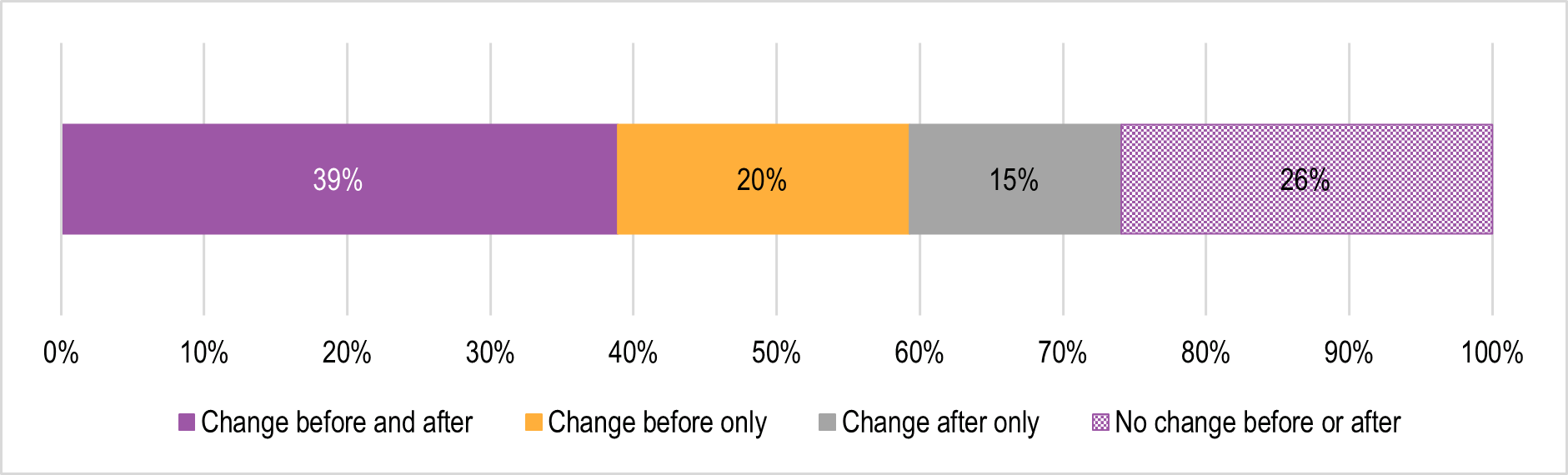{kind=link}
Some of the changes made in preparation for the CIS Scheme included developing forms, improving and updating processes, updating client management systems, improving data protection processes, and developing spreadsheets to hold new information.
Changes made following the implementation of the CIS Scheme included additional items such as adapting tools and processes based on feedback since implementation and conduct of reviews of existing record keeping systems.
The Ministerial Guidelines[20] provide a list of required information for record keeping, which is set out in the Child Wellbeing and Safety (Information Sharing) Regulations 2018. Organisations surveyed in 2019 about their record keeping were asked about the extent to which they adhered to the list of required information in relation to each of the key activities in information sharing. Required information relating to the category of receiving a request had the highest rate of compliance with 74% of respondents reporting that all mandatory items were recorded. While noting that this category has the smallest number of required items, the remaining categories relating to information requirements for responding to a request, voluntary disclosure, and receiving and responding to a complaint, had an appreciably lower level of full compliance.
Required information for record keeping provides information sharing entities with an important source of internal monitoring of effective implementation of the CIS Scheme and an ability to assess any improved outcomes for children and their families. If capacity allows, the information collected by information sharing entities could potentially be aggregated by government to enable measurement of the contribution of the CIS Scheme to the intended outcomes, such as earlier intervention and prevention.
| Recommendation 5: Compliance with record keeping requirements |
|---|
| That CIS Scheme partner government departments work with information sharing entities in their respective sectors to promote compliance with the legislated record keeping obligations under the CIS Scheme, as explained in the Ministerial Guidelines. |
More recent feedback from prescribed organisation and services highlights ongoing refinement of processes and tools to support the service’s commitment to taking responsibility for children. This has included amendment to intake forms for services that deal predominantly with adults to record any involvement of children and consent forms that raise client awareness of information sharing schemes.
[addressing the] Attitudes of staff who feel sharing information may impact on their relationship with the adult who is usually their client. [ensuring they] Know how to record/store shared information when it relates to a person who is not our direct client. Reminding our staff that we need to know there are children involved and therefore ask clients if they have children and keep those records up to date. We are changing forms to make this easier. (Workforce survey respondent)
A challenge is consumer anxiety about what information is being shared about you and your family and how well it is explained to the family and how well it is communicated to them about what information is shared by clinicians. (Workforce survey respondent)
Frontline staff - how to change consent forms so that staff can build these schemes into conversations with clients so that there are no surprises for clients down the road (Workshop participant)
A consistent conversation across services to ensure that service users are aware of and understand the information sharing reforms is important to effective implementation of the CIS Scheme and the ongoing process of engagement with service users and consumers (individuals, families and communities) more broadly.
| Recommendation 6: Service user awareness |
|---|
| That training modules and templates identify information sharing entity responsibility for, and provide resources to support a consistent approach to service user awareness of the information sharing reforms and ensuring they understand their implications, the obligations of information sharing entities and the service user’s rights. |
Organisations have also spoken about approaches to improve sharing of information through documentation of refusals to share as a means of prompting further consideration of the request.
Use of documentation regarding requests that have been knocked back to ensure that all organisations are clear of the consequences of not sharing the information; allowing them to escalate the issue where necessary. (Workshop participant)
Some organisations have implemented centralised systems for information sharing under the CIS Scheme. This has the advantage of a more streamlined, consistent and systematic response with the ability for continuous monitoring of the organisation/service’s performance. An illustration of this process and its impact on the best interests of the child is provided in Box 3.2. Note that potential unintended consequences of a centralised system are discussed in Chapter 6.
Box 3.2 Case study in implementation – Department of Health and Human Services (DHHS)
Situation and context
DHHS has established a central unit, the Information Sharing Team (IST). The IST is responsible for responding to requests for information from prescribed ISEs that request details of the Department’s Child Protection actions where there is no current Child Protection involvement (i.e. historical involvement only). Requests for current Child Protection information are triaged and where an open child protection case is identified, referred to the allocated Child Protection Practitioner There is a degree of interplay between the Child Protection Intake team and the IST, where there can be internal referrals to each other based on an assessment of the risks faced by the child.
In one situation, a request for information was received from a mental health facility that was prescribed under both FVIS and CIS Schemes. The request sought information on historical family violence perpetrated by a father.
Action
The request was allocated within IST, and a search of the Child Protection electronic client database revealed there was no current involvement with Child Protection. However, IST identified significant Child Protection history for the father’s children. The most recent Child Protection involvement stipulated that all contact with the father should be supervised.
The request did not provide sufficient information regarding the purpose of the request. An advisor from IST phoned the requestor to discuss the request further, and it was revealed that the father was recently involuntarily admitted and that the children were having unsupervised contact at the time.
Outcome
IST shared the relevant information with the requestor, including the information that Child Protection stipulated that all contact with the father should be supervised. The IST advised the requestor that a new assessment by Child Protection Intake was required to ensure that the children would continue to be kept safe. The requestor agreed to report to Child Protection Intake that day. The following day the requestor phoned the IST to confirm they made a report and will continue to liaise with Child Protection to ensure appropriate arrangements for supervised contact be put in place prior to the father being discharged. The IST engaged with the requestor successfully, provided them with the relevant information and also supported them to share that information with other relevant organisations (Child Protection Intake).
While there may have been other avenues for the requestor to access information, it appears that they may not have done so without the ability to confirm any previous history through use of the CIS Scheme, highlighting the ability of the Scheme to bring providers together to discuss the best possible actions for the child’s safety and wellbeing.
Source: Based on material provided by Department of Health and Human Services 2020
There was little change reported by workforces in their perception of the level of effort needed to align their organisation’s practices, procedures and systems to the CIS Scheme over the period of the two workforces surveys. The average ranking of level of effort was 6.2 in the 2019 survey and 6.4 in the follow up 2020 survey (0=very little effort and 10=extremely high level of effort; n=194). This result supports qualitative feedback from stakeholders that adjusting systems to the CIS Scheme have been ongoing in the period since commencement of the CIS Scheme, and that for many organisations, this has not been an inconsiderable effort.
[16] Department of Education and Training (2019). Information Sharing and Introduction to MARAM Training. Evaluation Report. Victoria State Government.
[17] Ibid
[18] Information Sharing and Family Violence MARAM Framework sector implementation support funding 2020-2021. Project Proposal. Family Safety Victoria.
[19] FSV convenes the MARAMIS Sector Capacity Building Working Group and the MARAMIS Sector Capacity Building Aboriginal Working Group
[20] Child Information Sharing Scheme Ministerial Guidelines. Guidance for information sharing entities. State of Victoria, Department of Health and Human Services, September 2018. Available at www.infosharing.vic.gov.au
4. Enablers and barriers to implementation
Enablers and barriers to implementation in the Child Information Sharing Scheme Two-Year Review report.
This chapter considers the research question:
- What are the key enablers and barriers to implementation of the CIS Scheme?
in the following contexts:
- ISEs have the skills and knowledge to effectively implement the CIS Scheme
- ISEs demonstrate increased participation in child information sharing
- ISEs have delivered activities to enable practice change to appropriately share information under the CIS Scheme
- ISEs’ implementation is true to the intent of the legislation and design of the CIS Scheme.
Box 4.1 Key findings – implementation enablers and barriers
- Stakeholders have identified enablers and barriers to implementation of the CIS Scheme that relate to issues such as the anxiety of workers around privacy and confidentiality concerns, translation of policy into practice and understanding of child-focus practice.
- Data on information sharing requests is thin and will need to improve for effective and ongoing monitoring of the child information reforms.
- A number of strategies have been adopted by prescribed organisations and services to target culture change in support of effective implementation of the CIS Scheme. There is opportunity to better disseminate these innovative approaches to the potential advantage of Phase One and Phase Two prescribed workforces.
- While there is a high level of understanding about the purpose of the CIS Scheme further work is required to embed practice.
Source: ACIL Allen Consulting 2020
4.1 Workforce skills and knowledge
Enablers
A wide range of enablers to effective implementation of the CIS Scheme through ensuring workforce skills and knowledge were cited by information sharing entities. These included:
- Building workforce understanding of the legislative basis for information sharing to improve confidence in applying the CIS Scheme.
Legislation is the great enabler - the kind of thing that would give confidence to people to share; it needs to be emphasised more to cut through issues of privacy and consent to make things happen. Central experts to help but if you have quality managers to champion this change across the organisation it would be useful. Cultural shift to a default to share rather than think of privacy as the first concern. 'Can-do' approach - take the first step to share and work out what is necessary to be done. (Workshop participant)
Addressing existing ingrained attitudes to privacy and reassuring workers not only of their responsibilities but also their protection in relation to CIS Scheme. (Homelessness Services workforce survey respondent)
Learning to overcome the privacy and confidentiality principles. Trusting that all organisations are acting within the child’s best interests. (Homelessness Services workforce survey respondent)
Alignment of confidentiality policies to the CIS scheme and understanding when this applies. (Out-of-Home Care workforce survey respondent)
- Having an identified person with responsibility for implementation of the Scheme (also see Box 3.2).
Allocated/dedicated person in charge of implementation - consistent information and useful to push the organisation. (Workshop participant)
- Translation of policy into practice including alignment with other policies, frameworks and guiding principles.
Relationship between policy and practice areas within an organisation - ensuring that other relevant policies sit well with the CIS Scheme, e.g. Child safety policy. Translation of policy into practice manuals and documents that guide operations. (workshop participant)
- Promotion of ongoing (experiential) learning through communities of practice.
Communities of practice for FVIS Scheme have been invaluable - how might this look for CIS Scheme or be used to promote ongoing education for CIS Scheme? (Workshop participant)
Barriers
Conversely, insights into barriers to effective implementation of the CIS Scheme because of a lack of workforce capability are provided by prescribed workforces responding to the follow up survey in 2020 about the main reason for not requesting information. This largely derives from insufficient knowledge of the CIS Scheme, and includes:
Unsure about the correct way to do so [apply the CIS Scheme]. (MCH workforce survey respondent)
Staff had still not participated in the training. (MCH workforce survey respondent)[21]
Agencies understanding of obligations. (Family Services workforce survey respondent)
Practice based skills development and confidence [needed]. Multiple workforces are still struggling to effectively implement CIS Scheme. (Alcohol and other Drugs (AOD) workforce survey respondent)
Please support and request that prescribed organisations develop their own practice-based workforce development strategy to promote embedding into practice; this is severely lacking across the board. (AOD workforce survey respondent)
Reminding other agencies that they can share. (MCH workforce survey respondent)
Other challenges experienced included:
- lack of practice in applying a child-focus
The challenges include professional discomfort in information disclosure and the fear of legal repercussions for such newly required practice. The organisation, itself, has been challenged by the requirement to be involved in the scheme when its identity has historically been that of an adult patient facility. A very small number of families have been affronted by what they have seen as a betrayal of professional confidentiality. (Workforce survey respondent – ‘Other’-health related organisation)
There was a culture of protecting information, especially health information. Education was needed to change the culture from protecting the subject of the information to protecting the child by sharing information. (Workforce survey respondent – ‘Other’-justice related organisation)
- lack of familiarity with the culture of other organisations
Understanding what to ask in a way the other organisation’s culture understands. (Workforce survey respondent - Family Violence Therapeutic Responses and Counselling)
- privacy perceptions (also discussed under ‘Enablers’)
Literacy about the Scheme, and how it relates to other Schemes (FVIS Scheme) and Acts (Children Youth and Families Act 2005, Mental Health Act 2014, and privacy legislation). (Workforce survey respondent – Mental Health Services)
Needs work with AHPRA (psychologists and psychiatrists) regarding patient confidentiality legislation and policy. (Workshop participant)
Another limitation in supporting their workforce was the inability of organisations to track completion of the eLearning modules, only access to the external links as the information sharing eLearning was not embedded within the organisation’s own learning management system.
4.2 Increased participation in child information sharing
The extent to which prescribed organisations and services are actively participating in child information sharing is considered based on July 2020 reporting to the ISMARAM Steering Committee on monitoring of information sharing. The reporting is not consistent across departments but does provide some evidence of the implementation of the information sharing schemes by government services and funded organisations.
- Department of Health and Human Services, Information Sharing Team (responsible for requests for information where there is no current Child Protection involvement)
- A total of 603 information requests in 2019. This included 119 under the CIS Scheme, and 78 where requests were made under both the FVIS and CIS Schemes. This compares to 406 requests under the FVIS Scheme only for the same period.
- A total of 516 requests in the first six months of 2020 with 119 requests under the CIS Scheme and 212 requests made under both the FVIS and CIS Schemes. This compares to 185 requests under the FVIS Scheme only.
- The subject of most information requests related to a child victim survivor.
- Victoria Police
- Since implementation of the respective information sharing schemes, there has been 2,179 requests for information under the CIS Scheme and 4,372 under the FVIS Scheme.
- Not all requests were shared. In some instances, voluntary shares were made in the context of an existing request.
- Department of Justice and Community Safety, Justice Health
- Where requests have been identified by information sharing scheme, numbers reported since implementation predominantly relate to sharing under the FVIS Scheme with a very small number of requests relating to the CIS Scheme. For example, for Justice Health, a total of 69 requests of which 6 related to the CIS Scheme and a further 15 related to requests under both the FVIS and CIS Schemes. Low numbers are not indicative of overall sharing activity and Justice Health continues to respond to requests for health information under a range of different legislative vehicles (including the Privacy and Data Protection Act 2014, the Health Records Act 2001 and the Children, Youth and Families Act 2005).
There is no benchmark for the expected use of the CIS Scheme, however, based on the relatively crude measure[22] of the information requests reported, with the exception of requests for Victoria Police to share, the volume of CIS Scheme requests suggest there is opportunity for improved application of the CIS Scheme in the interests of the wellbeing of the child. A ramping up of information sharing under the CIS Scheme may be evident in the information requests reported by DHHS IST for the first half of 2020, noting that this has predominantly been in a family violence context. Stakeholder feedback also suggests that there will be increased opportunity for sharing by Phase One prescribed workforces under the CIS Scheme with the prescription of Phase Two universal services (see section 5.1.3). It is expected that the Monitoring and Reporting Framework under development for the child information sharing reforms will enable better capture of information about implementation of the CIS Scheme and the extent to which the objectives of the CIS Scheme are being met.
This section supports the earlier recommendation for improved record keeping with the potential also to contribute to measurement of the achievements of the CIS Scheme (see section 3.4).
4.3 ISEs have delivered activities to enable practice change to appropriately share information under the CIS Scheme
A range of innovative approaches have been developed by prescribed organisations and services to support practice change among their workforces. This has involved embedding training in relevant existing training programs, making the language around the CIS Scheme more accessible, enabling awareness of children in their work, and identifying professionals/leaders available for secondary consultations.
We are integrating the information sharing schemes into the broader privacy and consent training for new staff. (Workshop participant)
We are supporting our workforce by deciphering the enormous amount of legislation and putting it into plain language for the staff to understand. Addressing staff attitudes and understanding of what exactly they can share, and ensuring they understand the legal obligations of sharing. Minimising the staff concerns around legal accountability for "oversharing". Managing the influx of information requests as external agencies realise what a resource our workforce is to them. (MCH workforce survey respondent)
Educating staff about CIS Scheme has enabled us to have conversations about the wellbeing of children and the need to keep them in focus. It has enabled us to update forms and incorporate the need to be aware of children in procedures. We have implemented a Dependent Care Plan for use for all clients who have dependent children. (Workforce survey respondent – Mental Health Services)
We have implemented training and set up key child safe officers across the organisation for secondary consults. (AOD workforce survey respondent)
Our organisation has clearly identified leadership team responsible for all related schemes, helpful for people in the organisation to have someone to go to. (Workshop participant)
There should be a process for capturing and disseminating examples of approaches to supporting workforce practice change, such as the potential for proactive sharing. At a minimum, this could be demonstrated through a series of case studies that have regard for the structure, size and location of organisations and services.
| Recommendation 7 Disseminating approaches to practice change |
|---|
| That good practice case studies across a range of contexts be identified and shared through a variety of media, including through innovation workshops and published material. |
4.3 ISE implementation is true to the intent of the legislation and design of the CIS Scheme
Sector understanding of the intent of the CIS Scheme legislation and how this should be reflected in implementation emphasises the importance of collaboration and expanded networks in the interests of the child. However, there is also a caution that implementation of information sharing schemes ensure that the needs of diverse and marginalised groups are addressed.
We need to shift from a risk averse info sharing culture to one that is more proactive, collaborative and appropriately balanced. (MCH workforce survey respondent)
[the legislation] supports the notion that ‘protecting children is everyone’s responsibility’; not just that of DHHS and police. It has led to more emphasis on early intervention and prevention through increased collaboration, and has removed information sharing obstacles, thereby reducing risk of harm to children. (MCH workforce survey respondent)
[the challenges of the CIS Scheme for my organisation are to] Ensure prescribed entities and workers know the scheme and their responsibilities. Improve processes for requesting and responding to request for information under the CIS Scheme and the FVIS Scheme. Improve methods to identify outcomes from sharing of information. Ensure best practice principles are enacted, children and young people are consulted re: sharing of sensitive and confidential information and people's legitimate rights to privacy are protected. Ensure the needs of diverse and marginalised communities i.e.CALD, LGBTIQ, disabled, rural, homeless, etc., are addressed and their increased vulnerability to violence, is addressed through the CIS Scheme and FVIS Scheme. (Workforce survey respondent - Specialist Victim Survivor Family Violence Service)
There would appear to be a high level of understanding amongst prescribed organisations and services about the purpose of the CIS Scheme. The challenge continues to embed the CIS Scheme in the tool kit for workforces to draw on where appropriate in ensuring that consideration is given to the wellbeing and safety of children based on the best available information and at the earliest opportunity.
[21] It is noted that as of 20 July 2020, 556 users had enrolled in the MCH tailored information sharing eLearn that covers the CIS and FVIS Schemes.
[22] Noting that the FVIS Scheme can be used where no children are present, Child Protection has other permissions to request information about child risk, and Justice Health is prescribed under the CIS Scheme only in relation to services to children in custody while the FVIS Scheme operates for their work in adult correctional facilities.
5. Achievement of intended outcomes
The following research questions are addressed in this chapter in considering the extent to which the CIS Scheme is achieving its intended outcomes:
To what extent has the CIS Scheme impacted the level and nature of relevant information sharing between prescribed information sharing entities?
In the context of the expectation that improved child information sharing supports better planning, service collaboration and earlier intervention.
To what extent has there been a positive impact on service provision in support of child wellbeing or safety?
In the context of the expectation that ISEs are enabled to identify and respond more appropriately to the wellbeing and safety needs of children through improved access to and quality of shared child information.
Box 5.1 Key findings – achievement of outcomes
Responding to a request to share information
- Among prescribed workforces, fewer perceive that there are legal restrictions or organisational policies that impede sharing information with other organisations or requesting information from other organisations.
- Prescribed workforces were less likely to refuse a request for information. Where there were refusals to share information, a clear reason for refusal was more likely to be provided than prior to the CIS Scheme.
- Privacy was significantly less likely to be a reason for refusing a request for information but was still likely to be a factor when workforce survey respondents’ requests for information were refused.
Information sharing activity
- Information sharing activity appears to have remained mostly the same since commencement of the CIS Scheme based on the results of the surveys of prescribed workforces, with some evidence pointing to a slight decline in the level of activity. Other evidence suggests that during the coronavirus pandemic there may be specific forms of information sharing activity that have increased while others have decreased.
Information sharing behaviour
- There appears to be some evidence for cultural shift towards early identification of supports for children, with some prescribed workforces appearing to have lower thresholds for seeking information.
- Prescribed workforces also appear to be considering a wider range of information sources when doing case planning for children.
- There is increased evidence of collaboration and coordination between sectors at various levels, including between peak bodies, individual services, and individual workers.
Embedding reforms
- Continued support and education is required to build on early signs of positive outcomes to ensure that these reforms are firmly embedded among information sharing entities.
Source: ACIL Allen Consulting 2020
5.1 Early identification and intervention to promote child wellbeing
5.1.1 Frequency of information sharing, and reasons for refusals to share information
Workforces from prescribed organisations and services were asked to reflect on the level of information sharing activity within their organisation in the 12 month period prior to and after commencement of the CIS Scheme.
The proportion of workforce respondents indicating that they had shared information (information going out) decreased marginally from 86% in the period before commencement of the Scheme to 83% following introduction of the Scheme with no change reported in the frequency of information sharing with other agencies following introduction of the CIS Scheme. Similarly, the proportion of workforces indicating that they had made requests for information remained the same at 70% both before and after introduction of the CIS Scheme, with a small decline indicated in the frequency of requests. Other evidence provided by the DHHS Information Sharing Team indicated an increase in information requests of 19% during the coronavirus pandemic period, which suggests that there may be specific forms of information sharing activity that have increased, while other types of requests have decreased.
However, while there was little change in what was already a relatively high level of reported child information sharing activity, prescribed workforces surveyed indicated in 2020 that they were less likely to refuse an incoming request for information after the implementation of the CIS Scheme suggesting that access to information has improved. Figure 5.1 shows how often prescribed workforces refused a request for information at baseline and follow-up surveys.
Figure 5.1 Frequency of refusals of incoming requests to share information among prescribed workforces
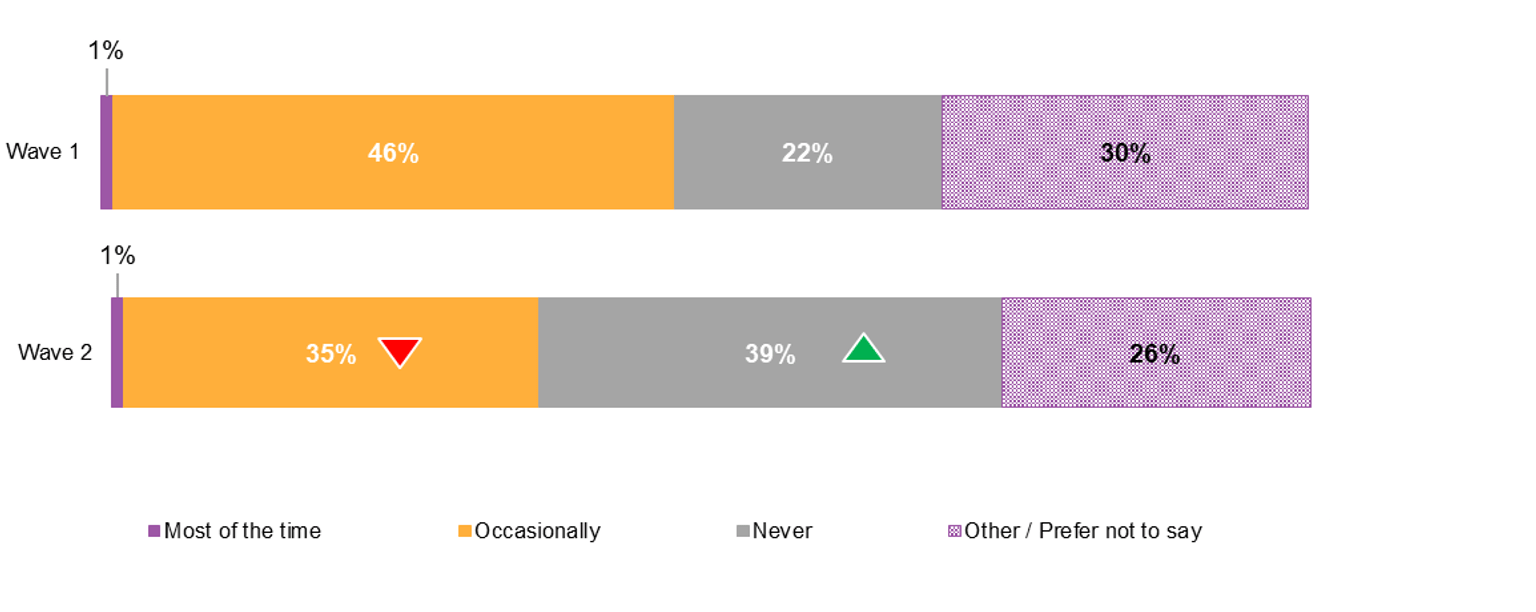
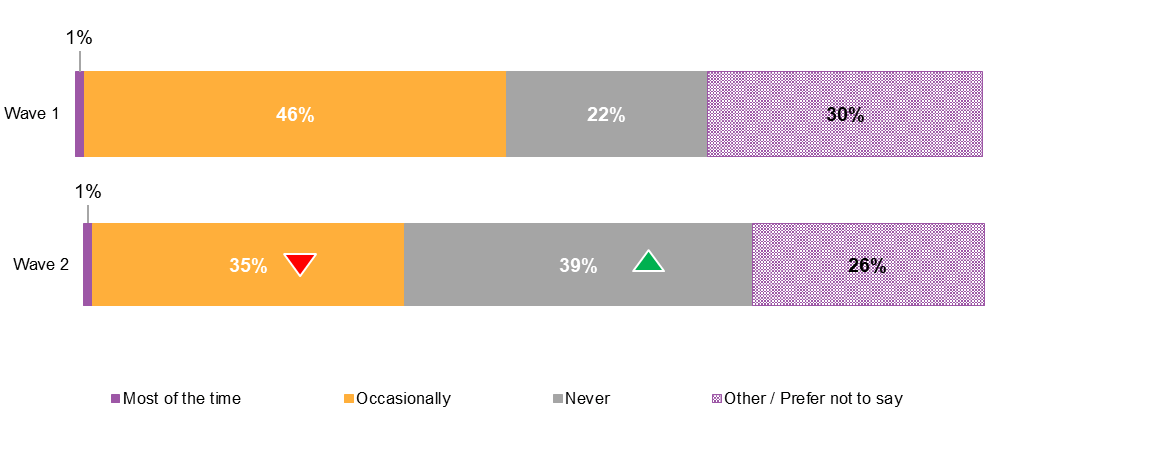{kind=link}
The proportion of prescribed workforces who indicated that they occasionally refused incoming requests for information decreased significantly by 11 percentage points, from 46% to 35%, and the proportion that indicated they never refuse incoming requests for information increased substantially by 17 percentage points, from 22% to 39%.
Figure 5.2 shows the commonly cited reasons for refusals of incoming requests for information.
Figure 5.2 Reasons for refusals of incoming requests to share information among prescribed workforces
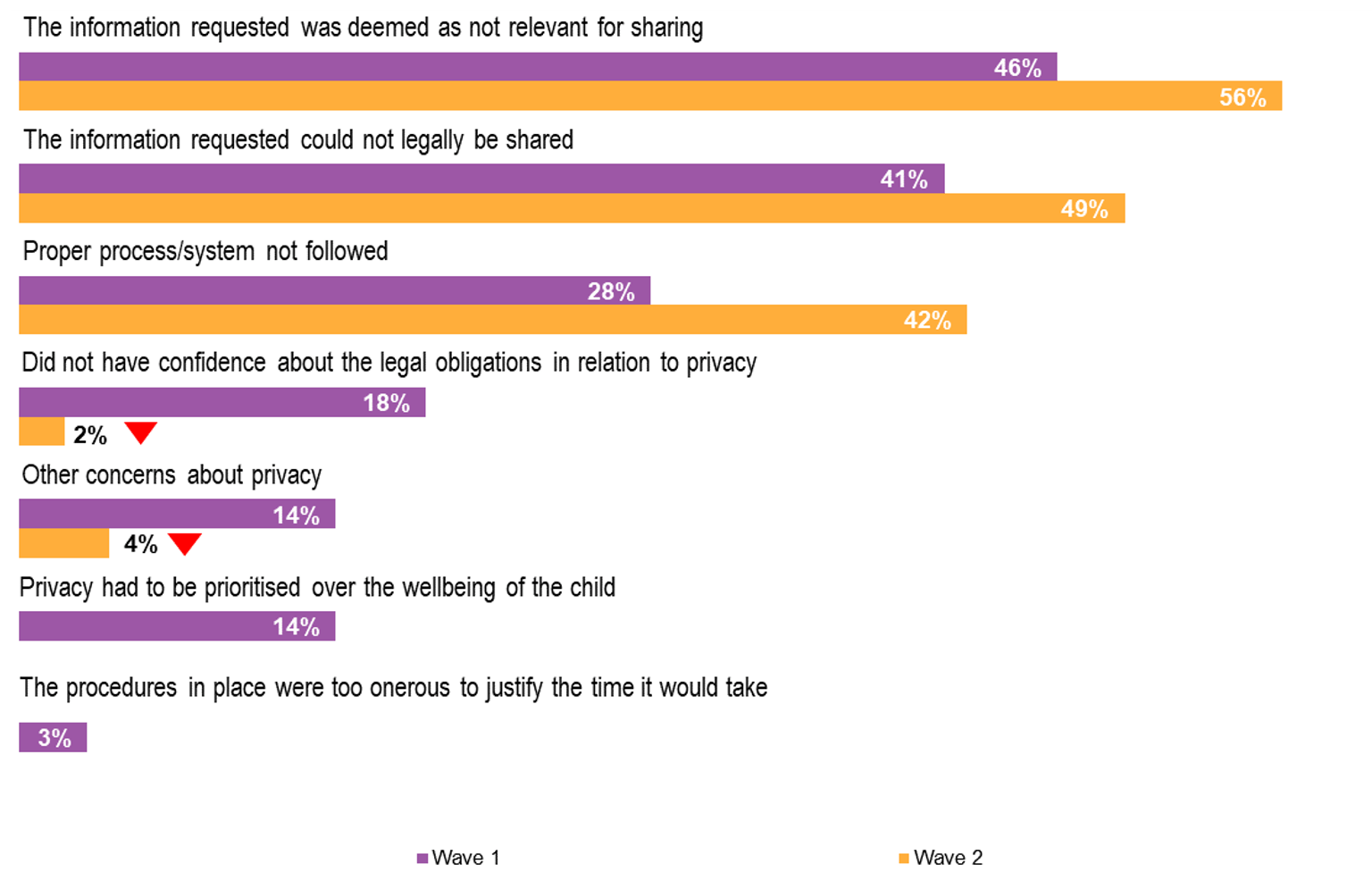
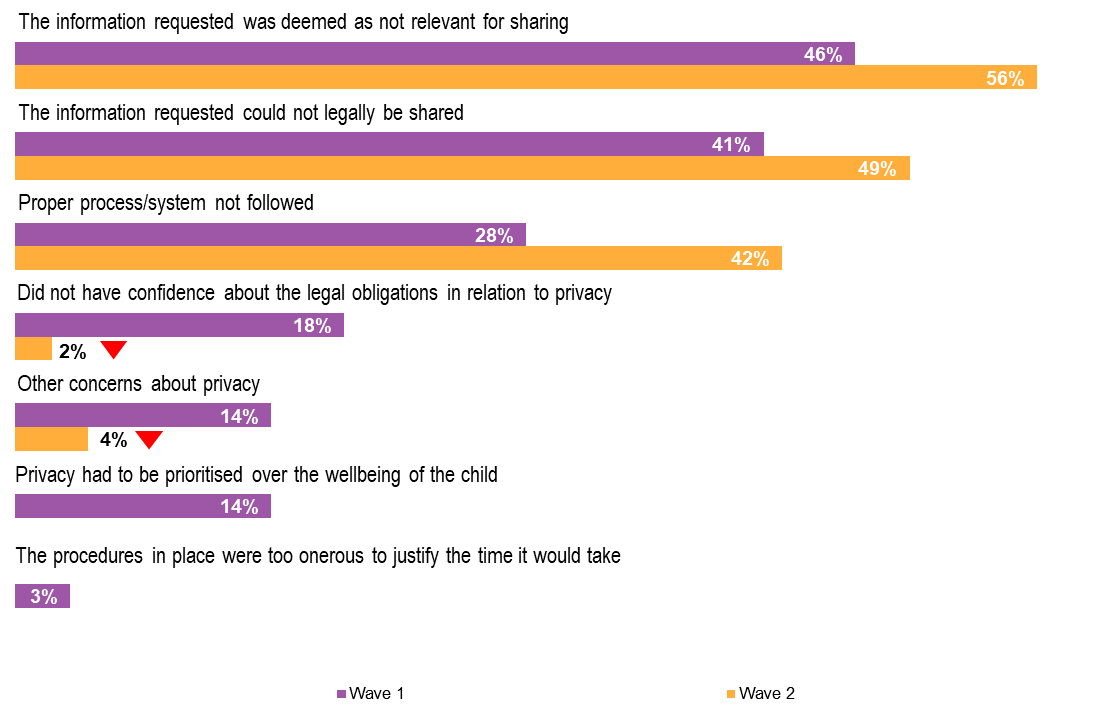{kind=link}
Reasons relating to the relevance and legality of information that had been requested had both increased slightly, suggesting that there is greater clarity in the assessment of incoming requests for information. This is supported by the change in reasons for refusal related to privacy which have all fallen sharply. Workforces who refused requests for information because they did not have confidence about their legal obligations in relation to privacy fell from 18% to 2%, while the proportion who had other concerns about privacy fell from 14% to 4%. There were no reports of respondents refusing a request for information because they had prioritised privacy over the wellbeing of a child
However, there was a substantial increase in incoming requests for information being refused for not following proper processes or systems, from 28% to 42%. While lack of conformity to ‘processes and systems’ will impact timeliness of access to information, it might be expected that this issue could be addressed, resulting in the successful sharing of information between ISEs, and that over time, familiarity with proper/preferred processes of other entities will streamline access to information.
In relation to outgoing requests for information, the frequency with which outgoing requests for information were refused is provided in Figure 5.3.
Figure 5.3 Frequency of refusals of outgoing requests for information among prescribed workforces
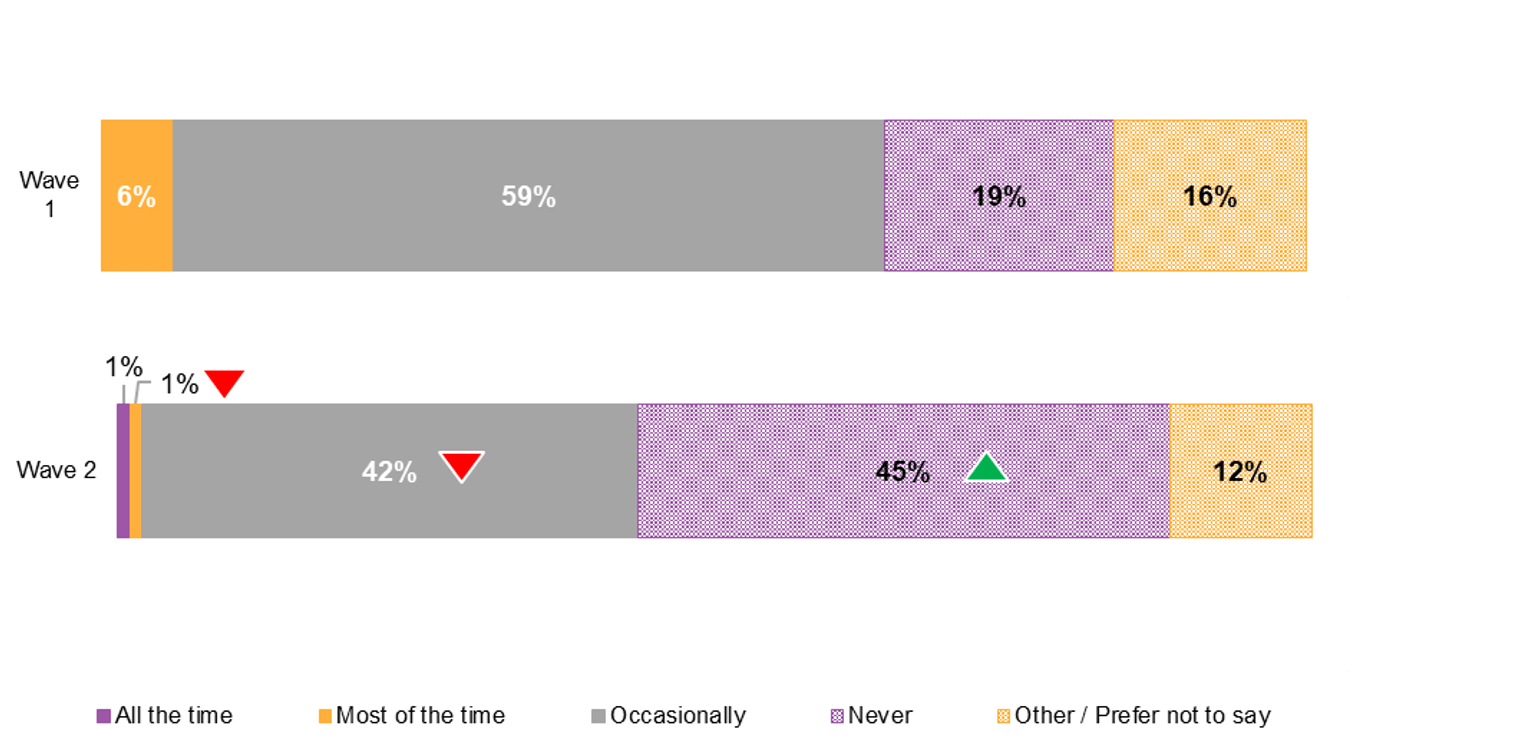
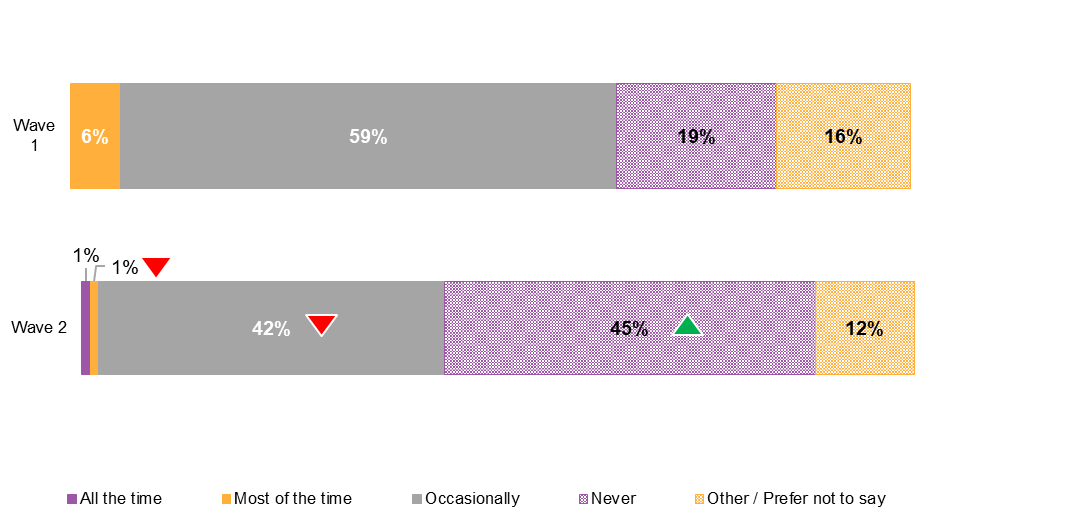{kind=link}
The frequency of refusals of outgoing requests for information among prescribed workforces has also declined. There was a significant increase of 26 percentage points in workforces reporting that their requests for child information were never refused in the 12 month period following commencement of the CIS Scheme, changing from 19% prior to introduction of the Scheme to 45%. A corresponding decrease in occasional refusals of outgoing requests was reported reducing by 17 percentage points from 59% to 42%.
Although there was little experience of outgoing requests for child information being refused most of the time prior to the CIS Scheme, this had also improved falling from 6% to 1% following introduction of the CIS Scheme.
The distribution of the most commonly cited reasons for why an outgoing request for information was refused is provided in Figure 5.4.
Figure 5.4 Reasons for refusals of outgoing requests for information among prescribed workforces
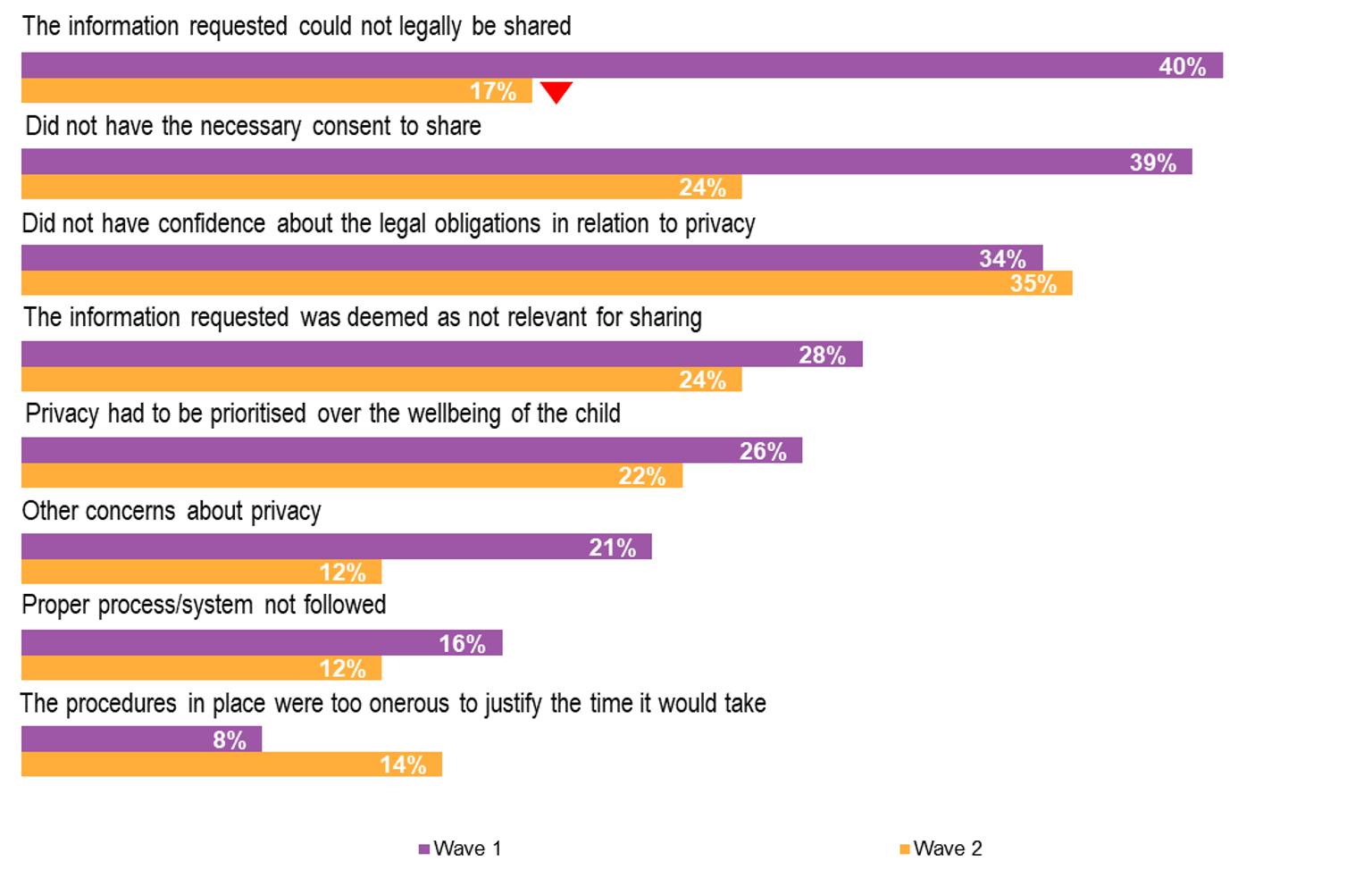
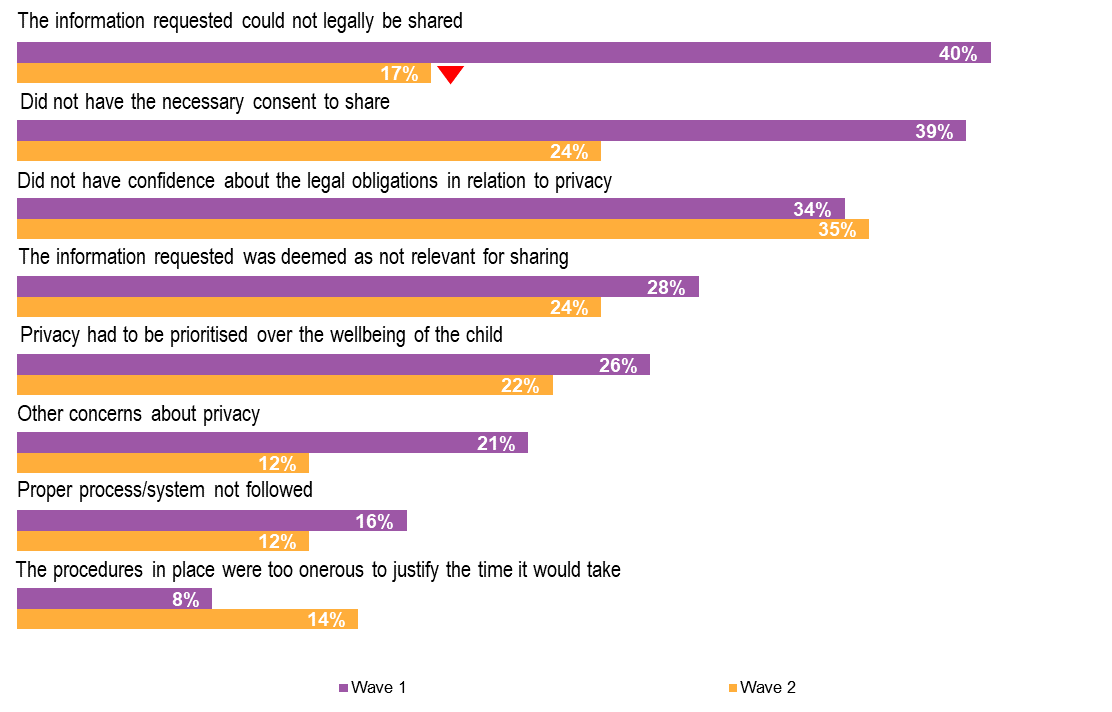{kind=link}
Prior to introduction of the CIS Scheme, the most commonly cited reasons for why outgoing requests for child information had been refused related to the legality of sharing the requested information and having the necessary consent to share. In the follow-up survey of workforces, there was a substantial reduction in the proportion of respondents attributing refusals to these reasons, strongly endorsing the purpose of the legislated CIS Scheme.
However, about one third of respondents continued to report that they had been refused a request for information because of a lack of confidence about the legal obligations in relation to privacy, and around one quarter that privacy had been prioritised over the wellbeing of the child. The continuing concerns about privacy as a reason for being refused a request for information to be shared appears to support stakeholder feedback about the ongoing need to educate other organisations/workforces about the provisions of the CIS Scheme. For the cohort of respondents to the workforces surveys, privacy concerns no longer feature as a common reason for them to refuse an incoming request for information (see Figure 5.2) suggesting that in this respect the cohort may have a better understanding of the operation of the CIS Scheme, and potentially an improved appreciation of the circumstances for sharing information more generally.
Approximately one quarter of workforces surveyed continued to report that outgoing information was refused because it was deemed not relevant to share. The issue of relevance is especially highlighted as the most common reason for refusal of incoming requests. It could be expected that a deeper understanding of how information held by other organisations will contribute to a better understanding of a child’s circumstances will improve the perception of relevance and practice of effective information sharing.
5.1.2 Effectiveness of child information sharing
On the matter of how effective organisations are in sharing child information, prescribed workforces perceived that practices in both sharing and requesting information had improved (see Figure 5.5), further supporting earlier evidence of improved access to information.
Figure 5.5 Workforces’ perceived effectiveness of information sharing to support child wellbeing, before and after CIS Scheme
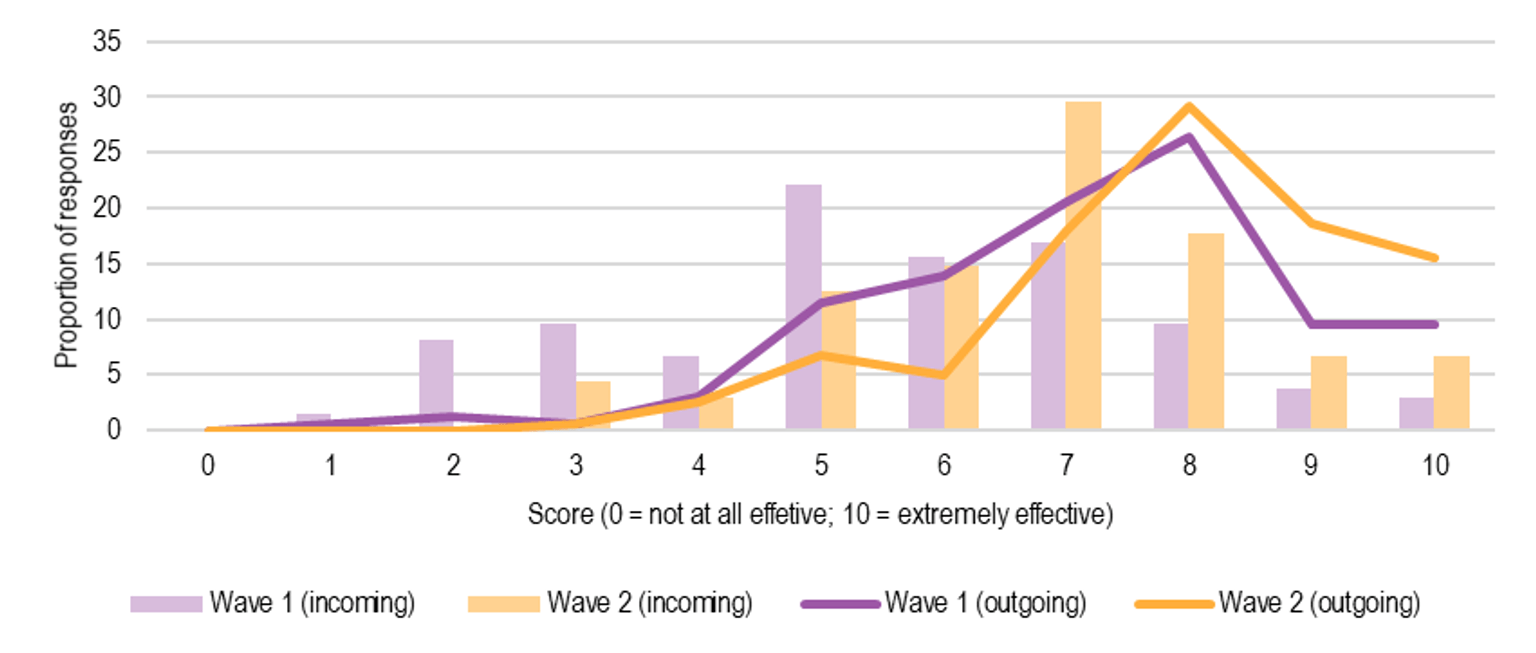
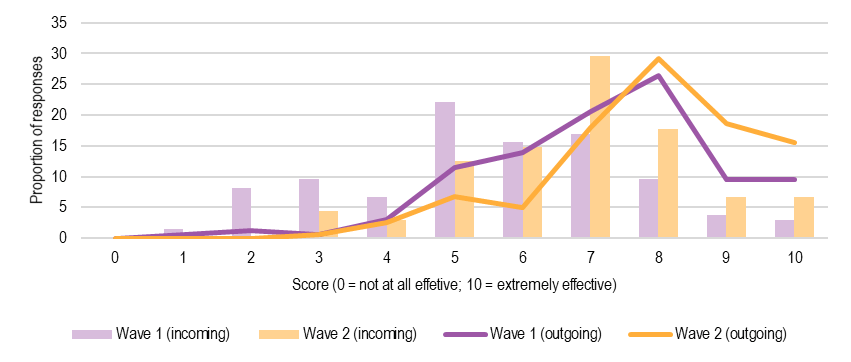{kind=link}
While prescribed workforces surveyed indicated that the level of information sharing activity had not changed since introduction of the CIS Scheme, respondents did feel that the capacity of their organisation and that of other organisations to share child information had improved following operation of the CIS Scheme. The average score given to perception of the effectiveness of their organisation in providing information (outgoing) increased from 7.2 prior to the CIS Scheme to 7.9. Similarly, while the capacity of other organisations to share information (incoming) was not ranked as highly, their effectiveness in sharing was felt to have significantly improved from a score of 5.5 to 6.8 following operation of the CIS Scheme.
5.1.3 Promotion of child wellbeing
Enabling policy and legislative environment
Based on the survey of prescribed workforces, in the period following commencement of the CIS Scheme, there were fewer encounters of a situation where a worker felt there was a need to provide information to promote the wellbeing of a child but was unable to act because of legal restrictions or organisational policies (see Figure 5.6).
Figure 5.6 Enhanced ability to promote child wellbeing
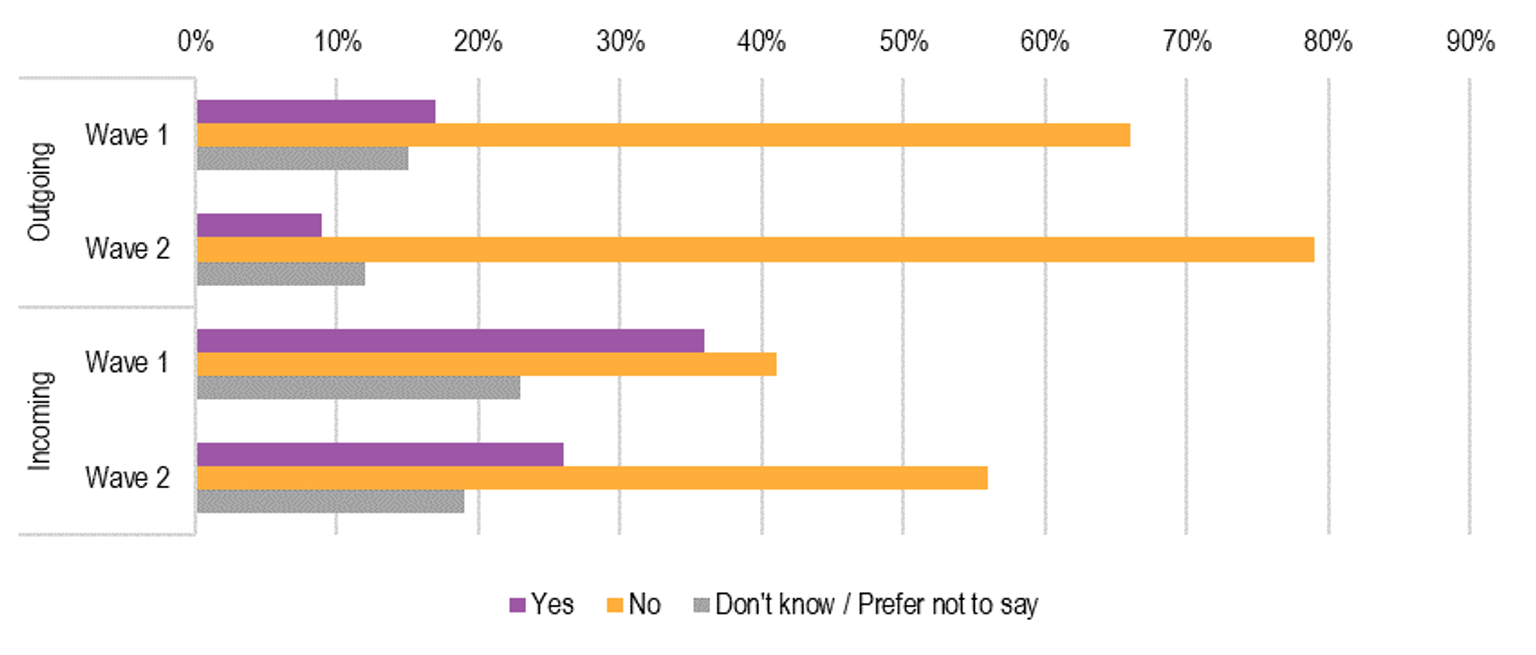
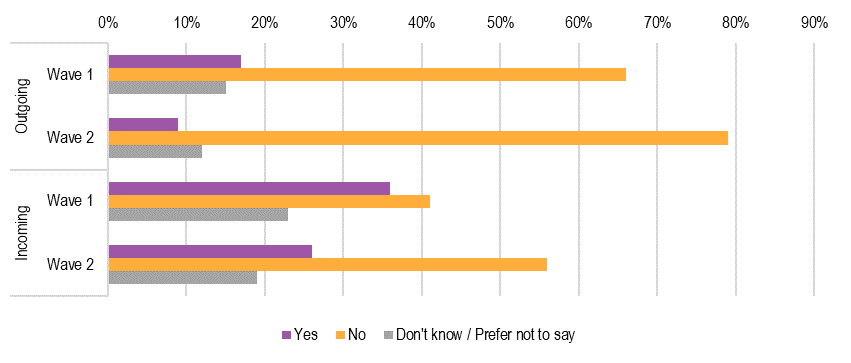{kind=link}
Reports of encounters where promotion of child wellbeing was impeded reduced significantly by eight percentage points from 17% to 9% where information had been requested (outgoing) by other organisations. Consistent with this improvement, reports of never encountering legal or policy impediments in relation to outgoing information improved by 13 percentage points from 66% to 79%.
Similar restrictions experienced on the ability of prescribed workforces to act on promotion of child wellbeing were reported when requesting information (incoming). A greater proportion of workforce respondents indicated that they had encountered legal or policy restrictions in seeking child information from other organisations and this remained relatively high following introduction of the CIS Scheme (Figure 5.6 also refers). About one third of respondents indicated that they had encountered this situation where acting on promoting child wellbeing had been impeded in the period before the CIS Scheme came into effect and this reduced to approximately one quarter of respondents following introduction of the CIS Scheme. There was a significant increase to just over half of respondents who had not encountered these restrictions on requests for information to enable them to act to promote child wellbeing, increasing by 15 percentage points from 41% prior to the CIS Scheme to 56% at follow up.
Threshold for information sharing
Evidence from multiple sources of data collected suggests that there has been a positive impact of the CIS Scheme in early identification and intervention of child wellbeing issues. The survey of workforces shows an increased ability to act on promotion of child wellbeing and workforces appear to be more effective at sharing information. There is also an indication that information sharing is now being used for cases where the risks are not as severe, compared to prior to implementation of CIS Scheme. This suggests a cultural shift towards earlier identification and intervention.
There appears to be a lowering of thresholds before staff think about seeking information – staff are beginning to request information even when circumstances are not severe or dire, or when they are not really serious or extreme. (Workshop participant)
Comprehensive assessment
In addition, there was feedback that the CIS Scheme has helped prescribed workforces have a better understanding of the different types of information that are held by different ISEs, and therefore a greater appreciation of how that information might assist in developing a more comprehensive and thorough assessment of risks and needs.
Within our staff their practice has been to expand their data sources when doing assessment and planning. The increased quality of assessment and planning is down to having more information from different sources to paint a more complete picture. (Workshop participant)
Prescribed workforces surveyed about the agencies with whom they most often share child information reported that while Child Protection remains the most commonly cited agency that information was shared with and requested from, there has also been increased engagement with Family Services and Specialist family violence services since operation of the CIS Scheme.
Role clarity
However, there were a number of other stakeholders who felt that the nature of their work and/or their organisations meant that it was difficult to consider early identification and intervention to improve the wellbeing of children. Such prescribed organisations and services were typically those operating at the crisis end of the service spectrum, such as domestic and family violence crisis services. Workers from these services are typically presented with issues of immediate risk and safety, and their role in early intervention and prevention is less clear.
Often by the time they get here (family violence service) it is not early intervention, and child-related issues are reported under mandatory reporting. Early identification and intervention are part of the CIS Scheme but it seems quite difficult to apply to the family violence sector. (Peak/lead body)
Risk and safety tends to be more of a concern for frontline services, and wellbeing is an afterthought for many of these workers. (Workshop participant)
A number of stakeholders also held the belief that early identification and intervention would be more applicable for universal services, as the nature of their interactions with children meant that they would be involved with children at a stage where promoting wellbeing was a focus. They therefore held the view that early identification and intervention would likely achieve its full effect after Phase Two of the CIS Scheme was implemented.
Universal services are more likely to operate from a wellbeing framework…schools, for example, are far more involved in the early intervention, prevention and support of children, so the true benefits will be seen in Phase Two. Organisations that don’t operate in the family violence space at all will be more likely to use the CIS Scheme. (Peak/lead body)
Overall, it appears that Phase One ISEs that have a component of child-focused practice have been able to use the CIS Scheme to improve their approach to early identification and planning through obtaining information from a wider variety of sources. However, it should be noted that tertiary services, with a greater focus on crisis response, have an important role in promoting child wellbeing. This can be seen, for example, in the application of the MARAM framework ensuring that the child is not overlooked in a family violence context, and through Child Protection referrals to Child FIRST alerting family support services to potentially vulnerable children. This illustrates the potential for tertiary services to be engaged in early intervention, and the importance of enabling the concept of a shared responsibility across the continuum of care.
It will be important to continue to enable Phase One secondary and tertiary services to actively seek opportunities to participate in child information sharing for purposes of promoting child wellbeing and safety. The implementation of Phase Two of the CIS Scheme should include strategies to strengthen existing and new efforts to leverage from the engagement with families and children of secondary and tertiary services, to optimise the extended support that might be available for shared clients.
| Recommendation 8: Role clarity in collaborative practice |
|---|
| That the implementation of Phase Two of the CIS Scheme includes strategies to strengthen collaboration between universal, secondary and tertiary services (that is, Phase One and Phase Two information sharing entities) around a child, to optimise benefits for the child, and to reinforce the contribution of Phase One prescribed workforces. |
5.2 Increased shared responsibility for child safety and wellbeing
Awareness of responsibility
In terms of shared responsibility for child safety and wellbeing, there appear to be some signs of positive impact. Overall, there has been a cultural shift among many information sharing entities, demonstrating that there is at least an improvement in the awareness of shared responsibility for child safety and wellbeing. This has led to an increased willingness to work together with other organisations and services to improve child safety and wellbeing.
There is an increased willingness for different parts of the organisation to work together…including people in different sectors understanding why child safety is important. (Workshop participant)
Where there was a pre-existing awareness of shared responsibility for child safety and wellbeing, the implementation of the CIS Scheme has reinforced this awareness and provided the opportunity for prescribed workforces to operationalise this shared responsibility.
Child safety is everyone’s business – this is becoming embedded more thoroughly than before. (Workshop participant)
Capacity to share
However, being able to act on this shared responsibility still required work to enable effective sharing of information.
Wellbeing is not considered sufficiently or uniformly…organisations that work with children or youth may not have a good understanding of how to record information robustly so that it can be shared with other organisations. (Peak/lead body)
The CIS Scheme has significantly influenced the attitudes of workforces and increased the awareness and understanding of shared responsibility for child wellbeing and safety, but increased efforts are needed to ensure that prescribed organisations and services have the capability and capacity to put this into practice.
Organisations have shifted in culture, but we need to drive the practice uplift more – people want to share but don’t know how to share, or how to share properly and well. (Workshop participant)
Proactive information sharing
The practice of proactive sharing or volunteering of information is also supported by the CIS Scheme and forms an important part of enabling earlier intervention. Some stakeholders believed that, as the CIS Scheme matures and workforces become increasingly familiar with the work that other organisations do, proactive information sharing will become an increasingly common practice.
Also, as their (workforces) skills mature in CIS Scheme they will probably increase in proactive sharing. (Key informant)
One example of how this has been effectively applied is illustrated in Box 5.2. For the Commission for Children and Young People, the CIS Scheme has met a gap in their powers to volunteer child information when considered appropriate. Being able to proactively share has provided staff with an additional avenue for supporting the wellbeing and safety of the child, as well as educating other organisations about the value of the CIS Scheme. (Also see section 3.3 and section 4.3.)
Box 5.2 Case study – proactive information sharing
Situation and context
The Commission for Children and Young People (CCYP) is an independent statutory body responsible for promoting improvement in policies and practices affecting the safety and wellbeing of children and young people, with a particular focus on vulnerable children and young people.
CCYP have existing powers to request information through the Commission for Children and Young People Act 2012 and the Child Wellbeing and Safety Act 2005.
Actions
CCYP’s existing legislative powers to request information are sufficiently broad and meet their needs, particularly in the investigation of child deaths and in operating the reportable conduct scheme. However, these powers are generally one-way and there is no capacity for CCYP to proactively share information with other organisations. There are also rare occasions where their powers cannot enable sufficient information sharing. These gaps have been addressed through the introduction of the CIS Scheme. CCYP have developed their own templates to assess the risks associated with disclosing information to others voluntarily and how to mitigate these risks.
Outcomes
CCYP now shares information with other ISEs voluntarily, while ensuring that these voluntary disclosures are appropriately assessed for their relevance and risks. In making these disclosures under the CIS Scheme, they have been able to educate other organisations and promote use of the CIS Scheme where relevant. Within CCYP, there has also been a cultural shift among staff where staff are thinking proactively of the CIS Scheme wherever their existing powers are not able to enable information sharing, and also thinking of opportunities to share information voluntarily.
Source: Based on information provided by Commission for Children and Young People. ACIL Allen Consulting 2020
5.3 Collaboration and coordination between services
There is strong evidence that there has been increased collaboration and coordination between information sharing entities as a result of the CIS Scheme. This has occurred at a number of levels.
Among the different peak bodies, their involvement in a joint working group has allowed them to forge new relationships and consider how they might work together to jointly and efficiently develop new resources to share with their respective workforces. For example, Domestic Violence Victoria indicated that they were working with the Council of Homeless Persons in developing animated case studies through funding provided by Sector Grants, which is likely to result in the development of inter-sectoral expertise within the family violence specialist and homelessness services. There were also plans over the next twelve months to work with No To Violence and the Centre for Excellence in Child and Family Welfare to develop collaborative risk management and a child-centred case management approach.
At an organisational level, there were examples of greater local collaboration as a result of implementing the CIS Scheme. For example, some organisations had implemented co-location to facilitate greater ease in information sharing but also to consider how best to implement information sharing between organisations and services that traditionally might not have worked together.
We had started to look at more co-location between organisations (e.g. one day a week) due to the increased information sharing activity prior to COVID-19, but this has since been put on hold. The co-location had been useful to understand other organisations and how different organisations can work better together. (Workshop participant)
Another avenue for coordination and collaboration has been through face to face training opportunities provided since the commencement of the CIS Scheme, which brought together participants from different organisations and sectors that were included in the prescription of Phase One information sharing entities. The structure of the training provided the opportunity for participants to interact with each other, allowing them to build relationships with people from different sectors. The activities as part of the training also allowed them to have greater insight into how different organisations and sectors might approach the same case differently.
The workshops allow them to break up into different groups to see the same case from the lens of different service providers and sectors…it really brings it home for the participants. (Peak/lead body)
While the coronavirus pandemic restrictions have meant that some of these activities (e.g. co-location and working together) have been interrupted, the gains in collaboration and coordination between services has continued through other activities. The training and workshops that are delivered virtually allow for significant levels of interaction between workforces from different sectors.
My experience is that COVID-19 pandemic restrictions have certainly disrupted direct client services, but it is also my experience that service collaboration and information sharing has increased. (Workforces survey respondent)
There was also feedback from peak/lead bodies that the increased capability generally and especially in regional organisations to communicate using virtual platforms had increased the capacity to deliver state-wide training/professional development more efficiently and with a greater level of participation from regional areas.
5.4 Supporting children’s access to and participation in services
The Review’s workforces survey findings indicated that the CIS Scheme has had a small impact on children’s access to and participation in services. At the baseline survey, 46% of participants responded positively to ‘increased safety/provision of services’ as a benefit of the CIS Scheme. At the follow-up survey of workforces, this had increased slightly to 55%.
While there was no other evidence of children’s increased access to and participation in services, a number of stakeholders indicated that there had been benefits in identifying children’s needs through an increased child focus as a result of the CIS Scheme. It could be expected that with consolidation of this increased awareness and understanding of children’s needs, increased opportunity will follow for more timely access to and participation in services.
A potential limiting factor raised by stakeholders is that many of the services that are involved in supporting children at an earlier stage are not yet prescribed. Examples were provided by MCH nurses, whose services are prescribed as part of Phase One of the CIS Scheme, wishing to work more collaboratively with other early childhood services. However, these early childhood services are not yet prescribed although planned for Phase Two.
As a result, it is likely that children’s access to and participation in universal services in particular, has not yet improved significantly but is likely to in the future. One example of how this could occur is illustrated in the following case study, which outlines how the CIS Scheme has enabled following-up of unregistered births, ensuring visibility and ability to provide a history of the child’s engagement with universal and other support services.
Box 5.3 Case study – filling crucial information gaps
Situation and context
The Registry of Births, Deaths and Marriages (BDM) is a business unit within the Victorian Department of Justice and Community Safety responsible for the registration and record keeping of significant life events for the Victorian community. These records allow accurate record keeping and serve important functions, such as proof of identity, tracing family history and providing important statistical data for research and government planning.
In particular, the registration of births is significant for children as it establishes a child’s legal identity, supports their ability to access vital services, and improves their visibility in the community. However, there are typically a number of unregistered births each year for various reasons.
Actions
BDM undertook a pilot process strategically aimed at using the CIS Scheme to support the performance of Registrar-prescribed functions that promote child wellbeing. The objective was for BDM to proactively request information from Maternal and Child Health (MCH) services to facilitate birth registration of a sample group of 16 children born in 2017 with unregistered births, where BDM had no other ability to contact the children’s mothers.
Outcomes
All 16 information requests across 12 local government areas were successfully shared and responded to, with new contact information for 14 mothers received. BDM was able to successfully contact five mothers, resulting in two birth registrations and a third pending registration requiring the father’s participation. The pilot provided valuable insight and actionable recommendations to enhance practices and communication tools in the future (such as development of a Birth Registration Online guide to assist MCH to support parents in registering births), as well as enhanced the relationship between BDM, MAV and local councils.
Source: Based on information provided by Registry of Births, Deaths and Marriages. ACIL Allen Consulting 2020
It could be expected that improved registration of births will also benefit the accuracy and value of the Child Link initiative currently under development.
6. Unintended adverse impacts
Unintended adverse impacts in the Child Information Sharing Scheme Two-Year Review report.
Consideration is given in this chapter to the following research question and the extent to which any adverse impacts of the CIS Scheme have been minimised by prescribed organisations and services:
- Have there been any unanticipated adverse impacts of the CIS Scheme and what has been the cause?
Box 6.1 Key findings – unanticipated adverse impacts of the CIS Scheme
-
The formalisation of information sharing practices among some information sharing entities has caused local relationships to decline as informal information sharing between local agencies has decreased. However, it is noted that previous options for information sharing may not have been appropriate and an objective of the CIS Scheme was to provide confidence around the legality of child information sharing.
-
In some cases, the CIS Scheme has complicated information sharing procedures for information sharing entities that previously shared information through other mechanisms. Information sharing entities are preoccupied with thinking about whether the CIS Scheme can be used and neglected the fact that they previously shared information through other avenues.
Source: ACIL Allen Consulting 2020
Stakeholders who participated in the data gathering activities occasionally raised unintended impacts, which were predominantly either positive or neutral. There were a small number of unintended adverse impacts that relate to perceived disruption to previous workable arrangements for information sharing. Generally, however, the perceived impacts could be considered short term disruption to pathways for information sharing with a view to enhancing the quality and extent of information sharing through a more rigorous and transparent process. Related discussion can be found in Chapter 7 and other areas of this report.
6.1 Formalisation of information sharing practices
A number of ISEs, particularly the large government departments such as DHHS and VicPol, have implemented centralised information sharing teams in their implementation of the CIS Scheme, developing formal information sharing processes, such as forms, procedures and protocols. These arrangements have led to more consistent information sharing practices and reduced the risks of information sharing without appropriate checks and balances. These arrangements have also provided dedicated resourcing so that operational frontline staff do not have to dedicate significant resources to meeting the information sharing requirements. However, stakeholder feedback suggests that an unintended adverse impact has been the erosion of local relationships between these agencies and local service providers.
Local pathways that allowed agencies to share information have been eroded, even though the schemes (both CIS and FVIS Schemes) had intended to further it. (Workshop participant)
It is noted that less formal arrangements prior to the CIS Scheme for sharing information may not have been an appropriate option, and that an objective of the reform was to provide confidence around the legality of child information sharing.
Another issue raised related to the formalisation of information sharing is that local workforces may not have the opportunity to operationalise the training that they receive, particularly in responding to requests for information. Feedback provided by stakeholders indicated that centralised teams have responsibility for closed or historical cases, while local DHHS and Victoria Police staff have responsibility for responding to requests for information where cases are active or open. There have been occasions where a request was passed to the central team when it should have been responded to by the local staff members, due to their unfamiliarity with the protocols and/or their lack of confidence in responding to requests. This may occasionally cause undue delays in preparing and providing a response.
Continued reinforcement from central information sharing teams about their role and that of local staff could be expected to overcome any confusion in the short term, and result in a more efficient sharing of information and allocation of resources.
6.2 CIS Scheme and other information sharing mechanisms
In most cases, where existing mechanisms for information sharing were being accessed, such as through the Children Youth and Families Act 2005 or other legislation or regulations, these arrangements have continued following the introduction of the CIS Scheme. However, stakeholders indicated that there were a small number of organisations or occasions where the CIS Scheme has caused confusion as workforces have tried to use the CIS Scheme to varying success while overlooking existing mechanisms.
Some people are really wary of using the scheme, but they’re forgetting that other avenues of information sharing already exist and have gone on for years. (Peak/lead body)
Most stakeholders appreciated that the CIS Scheme augments the information sharing capabilities of prescribed organisations. However, the fact that the CIS Scheme augments, rather than replaces, any existing information sharing processes or standards (such as the Child Safe Standards, Mandatory Reporting Requirements or Reportable Conduct Scheme) should continue to be reinforced through ongoing education and communications.
| Recommendation 9 Clarifying relationship to other legislation and standards |
|---|
| That consideration be given to providing material to reinforce how the CIS Scheme interacts with other existing legislation and standards, such as the Child Safe Standards, Mandatory Reporting Requirements and Reportable Conduct Scheme and, and how these relate to information sharing entities in different sectors, to ensure adherence to the intent of mechanisms available to facilitate child information sharing. Such an approach can highlight where the CIS Scheme provides additional information sharing powers over existing legislation and standards, providing clarity on when and how to use the CIS Scheme |
Another potential adverse impact of the CIS Scheme that was highlighted by stakeholders in the baseline report is inappropriate use of the CIS Scheme. While there were no examples of inappropriate use of the CIS Scheme or complaints arising out of implementation of the CIS Scheme encountered during the data collection for this Review, these continue to remain a risk. The potential for inappropriate use should be actively monitored at organisational and state-wide levels.
7. Prescription of information sharing entities
Prescription of information sharing entities in the Child Information Sharing Scheme Two-Year Review report.
This chapter addresses the following research question and includes consideration of the impact of the CIS Scheme on workforces including the interface of the CIS Scheme with the FVIS Scheme:
- How successful has it been to prescribe entities for child information sharing?
Box 7.1 Key findings – prescription of Phase One entities under the CIS Scheme
Integrated reforms
- Alignment of implementation of the CIS Scheme with the FVIS Scheme and MARAM framework was seen by Phase One prescribed workforces as consistent with the integrated way in which these reforms were being operationalised in practice.
- Interface of the FVIS and CIS Schemes has highlighted practices that can be strengthened to ensure the successful implementation of the CIS Scheme that include reinforcing the importance of routinely gathering accurate information, formalising standards for information collection and developing processes for documenting information sharing occasions and outcomes.
Phased introduction
- Improved sharing of information between secondary/tertiary and universal services was considered to be more likely to deliver the early intervention benefits intended for the CIS Scheme, and the opportunity to promote child wellbeing outside of family violence contexts.
- For some Phase One prescribed organisations and services, expanding the CIS Scheme under planned Phase Two will enable a whole of organisation approach to the CIS Scheme and collaboration with other internal services to be prescribed under Phase Two.
- Choice of information sharing entities for Phase One has been appropriate when reflecting on the scale of implementation and the training required. There is a continuing need to build child information sharing capacity among Phase One information sharing entities.
- The selection of Phase One information sharing entities has illustrated the breadth of service providers in contact with children directly or indirectly through a family context and supports provided to parents/carers, and the opportunities to build a wider network of services able to participate in promoting child wellbeing and safety.
Source: ACIL Allen Consulting 2020
In proposing a child information sharing scheme for Victoria it was intended that the model recognise the primacy of the principle of child wellbeing and safety, facilitate interagency collaboration in providing services to children, assist in identifying factors contributing to cumulative harm over time and improve the exchange of information between relevant government and non-government organisations. Prescribing information sharing entities would determine the scope and scale of reforms. It was also proposed that because of the significant overlap of family violence and child safety and wellbeing reforms, activities to support the reforms would be rolled out together to reduce any confusion amongst the workforce and community.[23]
In considering the impact of the proposed regulatory reform, the phased implementation of the CIS Scheme would involve both government and non-government organisations and align to implementation of the FVIS Scheme. Phase One prescription would focus on entities providing support for the most vulnerable children and who were considered to have a level of reform readiness.[24]
Feedback from Phase One information sharing entities suggest that the overlap in workforce responsibilities for CIS and FVIS Schemes has demonstrated the value of a more formalised approach to child information sharing and the importance of accurate recording of information. It has also highlighted for adult-focused services, the opportunity to improve consideration of child wellbeing and safety. In terms of intervening earlier, while Phase One information sharing entities understood this intent for the CIS Scheme, for some the current restriction on prescribed entities was seen as a limitation to achieving this aim. The planned introduction of Phase Two information sharing entities with a stronger emphasis on universal/upstream services was seen as offering the potential to engage a wider workforce in promotion of child wellbeing and safety.
Integrated package
Where there was feedback from stakeholders on the prescription of ISEs, there was generally acceptance or understanding of the overall policy direction – government was responding to the issues of both women and children, and therefore the implementation of the FVIS and CIS Schemes and MARAM framework together was perceived as a reasonable way to approach the reform.
I see them as part of an integrated package of keeping people safe. In practice FVIS and CIS Scheme sharing and coordination happens in an integrated way where there are children involved. (Workforces survey respondent)
Communication of the relationship between these reforms has improved over time, with stakeholders indicating that:
The messaging and rollout across government has become more sophisticated over time, it has been modified and tailored to better communicate in a more coherent manner for workforces. (Key informant)
The significant overlap of workforces prescribed under both the CIS and FVIS Schemes has provided a logical framework for integrated training but has also highlighted practices that can be strengthened to ensure the successful implementation of the CIS Scheme. Lessons for the CIS Scheme that have been drawn from among workforces responding to the follow up survey who were also working with the FVIS Scheme, include reinforcing the importance of routinely gathering accurate information, formalising standards for information collection and developing processes for documenting information sharing occasions and outcomes.
Qualitative feedback in relation to accuracy and comprehensiveness of records (respondents, follow-up workforces survey):
Continue to document case notes accurately.
Email requests; easier to action specifically what is required, by whom and for what purpose.
To have the accurate information is very crucial to be able to protect, help, planning and make the right decisions in keeping and monitoring children’s safety and assess their physical and mental needs.
Feedback in relation to systems and processes (respondents, follow-up workforces survey):
Develop internal program systems at worker level that includes formal information gathering/sharing as a standard part of risk assessment and safety planning is important.
Develop clear and consistent processes for reviewing, responding to requests and recording the outcomes.
There was also recognition among workforces that the CIS Scheme was supporting the greater awareness among family violence services of the need to consider the significant impact on the child of family violence and the often intersecting issues of mental health and alcohol and other drug use.
I think that it is important that the status of both schemes is held to be equal. This is an issue in an organisation that has adult clients who experience family violence, but the safety and wellbeing of the child is less obvious to nursing and medical staff. It has been the social work role to assess the risks and needs of the child even though they may be regarded as a secondary/indirect client in the eyes of the organisation. (Workforces survey respondent – ‘other’-health related organisation)
Phased prescription
There were a small number of stakeholder responses which indicated that they would have liked prescription of ISEs to be broader However, most of these stakeholders also reflected upon the implementation effort and were cognisant that broader implementation would have required even more effort and could have created other barriers to effective implementation.
One of the main reasons why these stakeholders would have liked a broader prescription of ISEs was related to the intent of the CIS Scheme. The focus for the CIS Scheme, particularly in relation to improving wellbeing, was on early identification and intervention. These stakeholders felt that ISEs in Phase One of the CIS Scheme were primarily working at the crisis end or where issues were severe and required significant intervention. These stakeholders, therefore, felt that universal services were really where the opportunity was for early identification and intervention. It could be expected that expansion of the CIS Scheme also will provide the opportunity to promote child wellbeing outside of family violence contexts.
Universal services will probably use the CIS Scheme better because they are more likely to think about wellbeing…an example being schools and how they work with Child Protection. Schools provide information to Child Protection but never receive information, which is important because they are so involved in early intervention, prevention, and support of children on a day-to-day basis. (Peak/lead body)
In some other cases, stakeholders indicated that prescription of only selected program areas or functions within an organisation created difficulties in establishing a whole-of-organisation approach in implementing the CIS Scheme. This included policies and procedures, case management systems, and operational workflows having to be split into CIS Scheme and non-CIS Scheme areas, which caused difficulties for some organisations. In addition, this prevented different service areas within the same organisation from potentially working together to create better outcomes for clients.
Parts of the organisation are in the Scheme and parts are not…we cannot develop an organisation-wide system or policy. The workarounds are that certain elements of information are not shared, and artificial blockages are being created. (Workshop participant)
Only a few of the programs within our organisation are prescribed services; it is hard to develop an organisational policy and procedure. (Workforces survey respondent - Family Violence Therapeutic Responses and Counselling)
Some workforces indicated that the non-prescribed program areas or functions of their organisation were already thinking about the potential benefits that could occur once they become prescribed as a part of Phase Two implementation. Knowing that they would be a part of Phase Two has also helped to temper their disappointment at not being prescribed as a part of Phase One.
Only MCH nurses are prescribed at the moment, but we expect that other early years’ services and educators are coming into the Scheme in the near future…we can then align the whole department’s[25] family and children services policies and procedures with the Scheme’s requirements. (MCH workforces survey respondent)
It could be expected that initial engagement of Phase One information sharing entities in the CIS Scheme will ensure that these services, acutely aware of how unsustainable downstream support is and the impact of entrenched and intergenerational disadvantage, can champion prevention and earlier intervention initially within secondary and tertiary services and ultimately among services operating across the continuum of care. The selection of Phase One information sharing entities has also served to illustrate the breadth of service providers in contact with children directly or indirectly through a family context and supports provided to parents/carers, and the opportunities to build a wider network of services able to participate in promoting child wellbeing and safety. As suggested elsewhere in this report, further support and time is required to ensure that Phase One information sharing entities fully operationalise the CIS Scheme and can work effectively with an expanded Scheme to improve equity of outcomes for children and young people.
[23] Children Legislative Amendment (Information Sharing) Bill 2017. Legislative Impact Statement.
[24] Regulatory Impact Statement. Child Wellbeing and Safety (Information Sharing) Regulations 2018.
[25] This use of ‘department’ by the stakeholder refers to the Child, Youth and Family Services department of a local council, as opposed to a government department elsewhere in the report.
8. Impacts of the CIS Scheme on diverse and disadvantaged communities
Impacts of the CIS Scheme on diverse and disadvantaged communities in the Child Information Sharing Scheme Two-Year Review report.
The following research question has been considered in this chapter in the context of ‘improved child information sharing facilitates improved identification of, and responses to, the needs of diverse and disadvantaged communities’:
- What has been the extent of the impact of the CIS Scheme on diverse and disadvantaged communities?
During this early period of implementation of the CIS Scheme, the major impacts of the CIS Scheme on diverse and disadvantaged communities have primarily been felt in Aboriginal and/or Torres Strait Islander communities. This chapter, therefore, incorporates relevant findings from other sources and considers how these lessons might impact the implementation of the CIS Scheme among diverse and disadvantaged communities, while providing a distinct discussion of the CIS Scheme’s impact on Aboriginal and/or Torres Strait Islander communities.
Box 8.1 Key findings – impact of the CIS Scheme on diverse and disadvantaged communities
Responding to diversity
- The continuing need to improve engagement of diverse population groups with support services will affect the extent of the impact of the CIS Scheme in this area.
- More robust data collection related to application of the CIS Scheme will be required to monitor and assess use and impact of the CIS Scheme with diverse communities.
Operation of the CIS Scheme in Aboriginal communities
- Aboriginal communities continue to be hesitant about information sharing being unsafe as:
- the CIS Scheme is not perceived to have been developed by Aboriginal people
- distrust and fear of the removal of children persists.
- There is support for development of Aboriginal community understanding about the CIS Scheme, and the development of culturally appropriate training and resource materials for prescribed workforces.
Identifying child information sharing issues
- Consistent with the broader investigation of approaches to improve access to, and participation in services by diverse population groups, an improved understanding of issues that could potentially jeopardise sharing of child information will be important to avoid undermining engagement with services.
Source: ACIL Allen Consulting 2020
Responding to diversity and disadvantage
The CIS Scheme forms part of a larger toolkit available to government and government funded service providers to promote the wellbeing and safety of all children in Victoria, with an emphasis on targeted supports for disadvantaged populations. There are a wide range of Commonwealth and Victorian policies, guidelines and frameworks that support the design of services, including workforce knowledge and skills, to respond to the needs of diverse populations with a view to improving access to specialist and mainstream services. Diversity encompasses Aboriginal and Torres Strait Islander communities, cultural and linguistic diversity, gender, disability, and people from lesbian, gay, bisexual, trans and gender diverse and intersex communities. [26] These guiding documents seek to promote equity of access and avoidance of disadvantage among diverse populations through organisational and workforce change that improves the quality of services and underpins standards such as access and participation. Change through service provider policies and practices aims to reduce discrimination, embed cultural responsiveness, foster social inclusive practices, offer healing and trauma informed care and access to language services.
Ensuring the most effective practices are in place to engage appropriately with these diverse groups is a continuing emphasis of government with implications for workforce structures and skills base. The extent to which this delivers improved practices over time also has implications for optimising the tools available to the workforce, such as the CIS Scheme, to promote the wellbeing and safety of children and young people. The findings of a recent parliamentary inquiry demonstrate this evolving understanding of diversity, barriers to accessing services and opportunities to improve outcomes for children [27]:
The Committee heard that people from culturally diverse backgrounds are underrepresented in early childhood services, such as Maternal and Child Health (MCH) and kindergarten, and face numerous barriers to engaging…[including] racism, limited awareness of services and their benefits, communication and language barriers, distrust of services, fear of being judged, and structural barriers.
Recommendations made by the Inquiry include addressing data gaps (largely through additions to the existing Child Development Information System) to enable accurate measurement of access to services of culturally diverse groups, and development of an early childhood workforce strategy setting out essential strategies and actions for effective engagement with culturally diverse children, families and communities.
It could be expected that the extent of the impact of the CIS Scheme on diverse and disadvantaged communities will be in part a measure of how well the CIS Scheme is utilised and in part reflective of how well services are engaging with diverse communities. While the following stakeholder feedback provides insights into challenges associated with use of the CIS Scheme to benefit Aboriginal and Torres Strait Islander communities, the ability to monitor and evaluate the impact of the CIS Scheme on outcomes for diverse and disadvantaged communities will require a more rigorous approach to data collection, further supporting the earlier recommendations relating to gathering data to improve information about practice (see section 3.1 and section 3.4). Should the data collection recommended by the Inquiry cited above be supported, data linkage within prescribed organisations would facilitate a robust understanding of the application of the CIS Scheme in relation to diverse and disadvantaged communities.
| Recommendation 10 Measuring contribution of the cis scheme in responding to the needs of diverse and disadvantaged communities |
|---|
| That CIS Scheme partner government departments consider the adequacy of the current minimum record keeping requirements of the CIS Scheme, including as they inform the role of the CIS Scheme in responding to the needs of diverse population groups. |
Application of the CIS Scheme in diverse and disadvantaged communities
Other stakeholder feedback in relation to diverse and disadvantaged communities was relatively minor and it was difficult, therefore, to draw further conclusions. A small number of stakeholders indicated that for specialist sectors (such as the disability sector) there is a need for training and resources to be particularly tailored to their work in order to assist in effective implementation.
While not a point that was explicitly raised by stakeholders within this project, the review of the FVIS Scheme noted feedback from one practitioner that the impact of the FVIS Scheme on the LGBTIQ community was difficult to understand given the limitations in obtaining cohort specific data. The FVIS Scheme review also noted that in some of these diverse communities, such as LGBTIQ communities, experiences were likely to spread quickly within their community and so it was important not to compromise the education and engagement with the community by delivering negative outcomes to these clients.[28]
| Recommendation 11 Engaging diverse and disadvantaged communities |
|---|
| That CIS Scheme partner government departments engage diverse and disadvantaged groups through sector and advocacy peak bodies and information sharing entities, to understand any specific barriers to the implementation of the CIS Scheme and use these findings to assist information sharing entities to overcome these barriers. |
Implementing the CIS Scheme for Aboriginal and Torres Strait Islander communities
While Aboriginal stakeholders consulted as part of this project broadly expressed support for the CIS Scheme, a well-documented complexity of historical and current issues, such as the Stolen Generation and over-representation in the criminal justice system and out-of-home care, affect how Aboriginal and Torres Strait Islander communities perceive and interpret government legislation and policy. A key issue reported in the successful implementation of the CIS Scheme for Aboriginal community controlled organisations (ACCOs) has been barriers related to lack of trust among community members because of the legacy and abiding harm of past experiences relating to child services.
There is still a lot of distrust and fear of children being removed as a result of information sharing. (Peak/lead body)
Similar feedback was provided to the Two Year Review of the FVIS Scheme in relation to the combined operation of the two information sharing schemes, although the opinions of Aboriginal organisations were reported to be divided[29]:
There was widespread concern that combined the FVISS and the Child Information Sharing Scheme could lead to an increase in the involvement of Child Protection and Aboriginal mother’s lives. For a minority, the Scheme (FVISS) created an opportunity for greater attention to children’s risk in the context of family violence and contributed towards building more collaborative relationships between child and family welfare agencies and specialist family violence services.
The CIS Scheme is specifically aimed at facilitating support to families and children at an earlier opportunity before matters escalate and, for example, lead to the involvement of Child Protection services. As such, there is a need to continually educate and reassure families and communities on the objectives and intended outcomes of the CIS Scheme and its value in a range of circumstances including in the context of family violence. However, this requires a significant investment of time and effort from the ground up, beginning with the development of culturally appropriate resources for the CIS Scheme. It is not apparent that the universal tools and materials developed for the CIS Scheme have been informed by consultation with Aboriginal people. Development of culturally appropriate resources appears to have been regarded as a task best left for the Aboriginal services sector, without strong leadership or direction from government. Some initiatives have been perceived positively and welcomed, such as the Aboriginal working group and communities of practice formed under FSV. Other areas, however, such as investment in the development of culturally appropriate resources, were perceived as lacking.
We are working on embedding it (CIS Scheme) in our organisation first; we haven’t done anything in the community so far. The funding has not been sufficient for our internal work, never mind external, and we have been putting in our own money (as other ACCOs are doing). (Peak/lead body)
While stakeholders were cautious about the pace of implementation of the CIS Scheme among Aboriginal organisations and service providers, they were also confident that the CIS Scheme will lead to better outcomes for Aboriginal women and children. It was also emphasised that sufficient care should be taken in implementation, as any negative experiences due to the CIS Scheme will be amplified in community and make it more difficult to implement the Scheme successfully. In this regard, it is noted that the Two Year Review of the FVIS Scheme recommended that an annual forum of key stakeholders be convened to consider any adverse impacts of the FVIS Scheme on Aboriginal people. Given the potential to use the CIS Scheme in conjunction with the FVIS Scheme, such a forum should provide an opportunity also to consider any adverse impacts of use of the CIS Scheme in the family violence context.
Some suggestions raised by stakeholders for further improvement in the implementation of the CIS Scheme include:
- providing dedicated training sessions for Aboriginal organisations and service providers, as staff can find it difficult to raise culturally relevant issues during training with mainstream service providers
- greater leadership from government agencies (e.g. Aboriginal Unit in FSV/DET) in development or adaptation of materials that are culturally appropriate
- continued investment in the implementation of the CIS Scheme, acknowledging that change will require greater time particularly for Aboriginal and/or Torres Strait Islander organisations and communities.
| Recommendation 12 Cultural safety |
|---|
| That CIS Scheme partner government departments continue to work with and support the Aboriginal service sector to provide community engagement to ensure Aboriginal communities have a good understanding of the CIS Scheme, and to ensure that cultural safety is taken into account at all stages of using the CIS Scheme. |
| Recommendation 13 Culturally appropriate resources to support implementation of the CIS Scheme in Aboriginal communities |
|---|
| That CIS Scheme partner government departments work with Aboriginal lead bodies to develop culturally appropriate training and support materials for the effective implementation of the CIS Scheme in Aboriginal communities, both by Aboriginal-specific and mainstream information sharing entities |
The Two-Year Review of the FVIS Scheme also raised the view that cultural safety and competence was not sufficiently embedded in mainstream organisations. Some other policy initiatives, such as the DHHS Aboriginal and Torres Strait Islander Cultural Safety Framework, could be leveraged to improve cultural competency among all ISEs, which will assist in ISEs being more likely to implement the CIS Scheme in a culturally appropriate manner, utilising culturally appropriate materials effectively.
[26] Key policies, guidelines and frameworks. Design for Diversity. State of Victoria, Department of Health and Human Services
[27] Inquiry into early childhood engagement of culturally and linguistically diverse communities. Legislative Assembly Legal and Social Issues, Parliament of Victoria. September 2020, p.xiii.
[28] McCulloch J., Maher, J., Fitz-Gibbon, K., Segrave, M., Benier, K., Burns, K., McGowan, J. and N., Pfitzner. (2020) Review of the Family Violence Information Sharing Scheme Final Report. Monash Gender and Family Violence Prevention Centre, Faculty of Arts, Monash University.
[29] Op Cit. Monash University, p.60.
9. Summary of recommendations
Summary of recommendations in the Child Information Sharing Scheme Two-Year Review report.
The following is a compilation of the thirteen recommendations made in this report based on the findings of the review of the first two years of operation of the Child Information Sharing Scheme (the CIS Scheme).
| Recommendation 1 Enquiry line data collection |
|---|
| That operation of the Enquiry Line be funded to accommodate the expansion of information sharing entities under the information sharing reforms, and to facilitate the collection of ‘real time’ data to inform effective implementation of the child information sharing reforms. |
| Recommendation 2 Sector support |
|---|
| That support be provided to sector peak/lead bodies, similar to the Family Safety Victoria sector grants, to strengthen the response to sector-specific needs of information sharing entities in understanding and applying the CIS Scheme in a range of circumstances and to promote cross sector collaboration and consistency. |
| Recommendation 3 Assessing threshold for 'wellbeing' |
|---|
| That further guidance be provided for prescribed workforces regarding expectations associated with ‘promoting child wellbeing’ under the CIS Scheme. That this further guidance be informed by an audit of state-wide and sector specific resources with the aim of identifying guidance gaps, particularly in relation to promoting a shared understanding of child wellbeing and risk thresholds, and child and family service system roles and responsibilities in relation to child wellbeing. |
| Recommendation 4 Strengthening capacity of Phase One workforces |
|---|
| That change strategies and ongoing training of information sharing entities related to the information sharing reforms continue to develop capacity among Phase One prescribed workforces and to facilitate integration of practice between Phase One and Phase Two prescribed workforces. This could be facilitated through workforce forums developed in collaboration with peak/lead bodies, and through support for local and place-based networks across sectors and promotion of local champions. |
| Recommendation 5 Compliance with record keeping requirements |
|---|
| That CIS Scheme partner government departments work with information sharing entities in their respective sectors to promote compliance with the legislated record keeping obligations under the CIS Scheme, as explained in the Ministerial Guidelines. |
| Recommendation 6 Service user awareness |
|---|
| That training modules and templates identify information sharing entity responsibility for, and provide resources to support a consistent approach to service user awareness of the information sharing reforms and ensuring they understand their implications, the obligations of information sharing entities and the service user’s rights. |
| Recommendation 7 Disseminating approaches to practice change |
|---|
| That good practice case studies across a range of contexts be identified and shared through a variety of media, including through innovation workshops and published material. |
| Recommendation 8 Role clarity in collaborative practice |
|---|
| That the implementation of Phase Two of the CIS Scheme includes strategies to strengthen collaboration between universal, secondary and tertiary services (that is, Phase One and Phase Two information sharing entities) around a child, to optimise benefits for the child, and to reinforce the contribution of Phase One prescribed workforces. |
| Recommendation 9 Clarifying relationship to other legislation and standards |
|---|
| That consideration be given to providing material to reinforce how the CIS Scheme interacts with other existing legislation and standards, such as the Child Safe Standards, Mandatory Reporting Requirements and Reportable Conduct Scheme, and how these relate to information sharing entities in different sectors, to ensure adherence to the intent of mechanisms available to facilitate child information sharing. Such an approach can highlight where the CIS Scheme provides additional information sharing powers over existing legislation and standards, providing clarity on when and how to use the CIS Scheme. |
| Recommendation 10 Measuring contribution of the CIS Scheme in responding to the needs of diverse and disadvantaged communities |
|---|
| That CIS Scheme partner government departments consider the adequacy of the current minimum record keeping requirements of the CIS Scheme, including as they inform the role of the CIS Scheme in responding to the needs of diverse population groups. |
| Recommendation 11 Engaging diverse and disadvantaged communities |
|---|
| That CIS Scheme partner government departments engage diverse and disadvantaged groups through sector and advocacy peak bodies and information sharing entities, to understand any specific barriers to the implementation of the CIS Scheme and use these findings to assist information sharing entities to overcome these barriers. |
| Recommendation 12 Cultural safety |
|---|
| That CIS Scheme partner government departments continue to work with and support the Aboriginal service sector to provide community engagement to ensure Aboriginal communities have a good understanding of the CIS Scheme, and to ensure that cultural safety is taken into account at all stages of using the CIS Scheme. |
| Recommendation 13 Culturally appropriate resources to support implementation of the CIS Scheme in Aboriginal communities |
|---|
| That CIS Scheme partner government departments work with Aboriginal lead bodies to develop culturally appropriate training and support materials for the effective implementation of the CIS Scheme in Aboriginal communities, both by Aboriginal-specific and mainstream information sharing entities. |
Appendix A: Key points from baseline report, Child Information Sharing Scheme Two-Year Review
Baseline Report, December 2019.
A.1 Baseline: Information sharing prior to commencement of the Child Information Sharing (CIS) Scheme
Attitudes
- A large majority of workforces surveyed believed that they understood the benefit to children of information sharing and were open to sharing information within the legal frameworks.
- A majority of workforces surveyed knew where to go for guidance when sharing information and promoted information sharing to others
- Just over one quarter of workforces surveyed reported that they had been reluctant to share information because they may be doing the wrong thing.
- Approximately two-thirds of workforce respondents reported that their organisation had policies covering sharing of information with external organisations.
- More than three-quarters considered these policies enabled exchange of information.
- Approximately one-third considered that these policies may sometimes have hindered early intervention.
Practice
- Most workforce respondents (83%) identified that their organisation shares information with other agencies but a smaller proportion (70%) requested information from other agencies.
- Where information sharing requests had been refused, the most common reasons were lack of necessary consent to share, information was not deemed relevant to share and information could not legally be shared.
A.2 Adjusting to the CIS Scheme
- Approximately three-quarters of organisations surveyed had made changes to their record keeping process and systems in anticipation of, and/or after introduction of the CIS Scheme.
- Most organisations surveyed are not currently recording all required information under the CIS Scheme.
- Workforce respondents’ perceived benefits of the CIS Scheme include transparency and easier sharing of information, better service delivery through increased safety/provision of services and to a lesser extent, services collaboration.
- Perceived challenges of the CIS Scheme relate to understanding of the Scheme, concerns about client privacy, and having sufficient resources to manage the Scheme or train staff.
A.3 Opportunities for improved implementation of the CIS Scheme
- Workforce respondents supported standardised templates for information sharing to address lack of consistency across departments and agencies, and streamlined training tailored to sectors.
- Sector peak/lead bodies advocated for clear, concise and practical resources for frontline staff, case studies to promote understanding of wellbeing and application of the CIS Scheme, and access to information describing the type of information held by organisations in different sectors.
Appendix B: Program logic model: Child Information Sharing Scheme
Appendix B for the Child Information Sharing Scheme Two-Year Review report.
B-1 Program logic model: Child Information Sharing Scheme
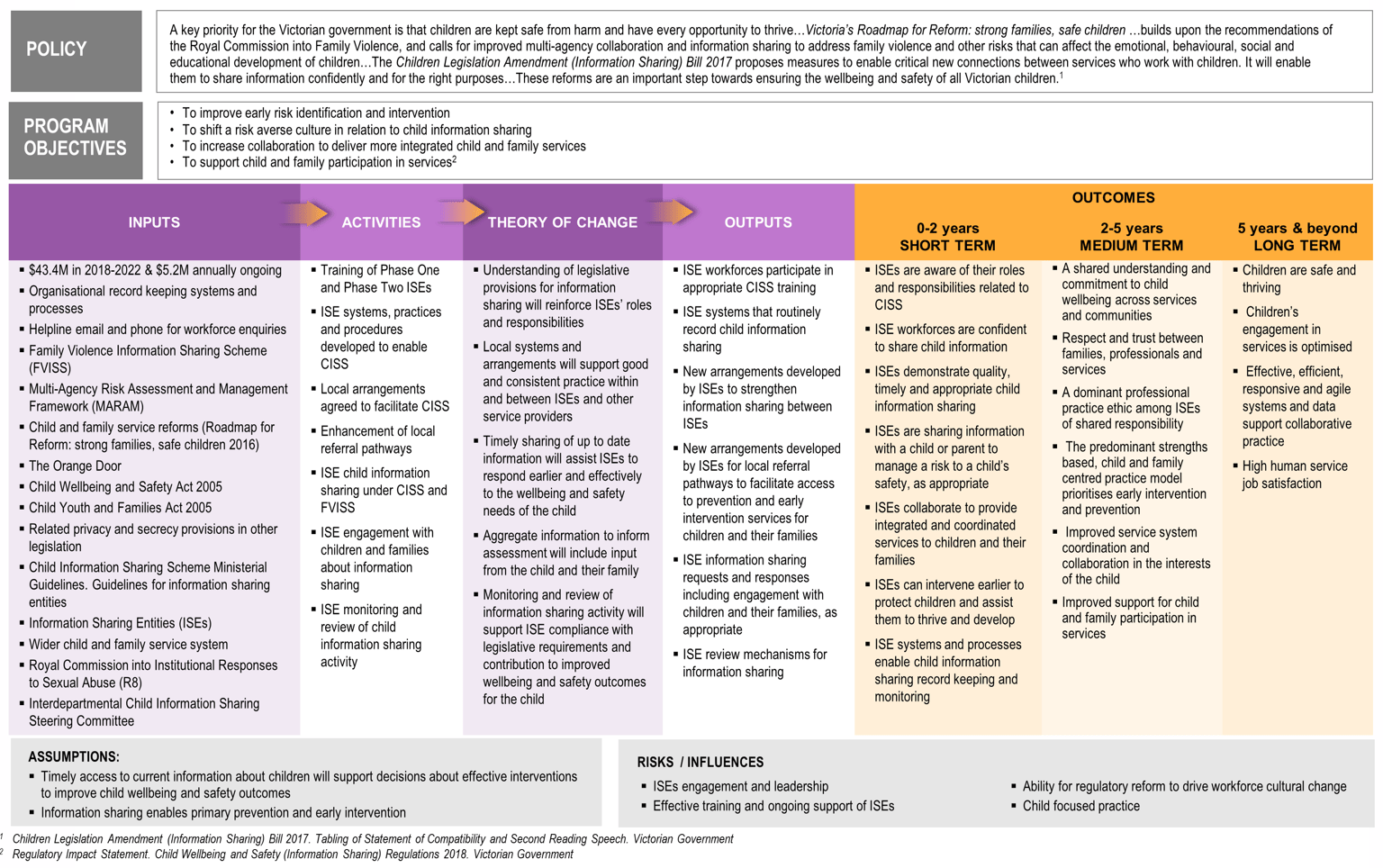
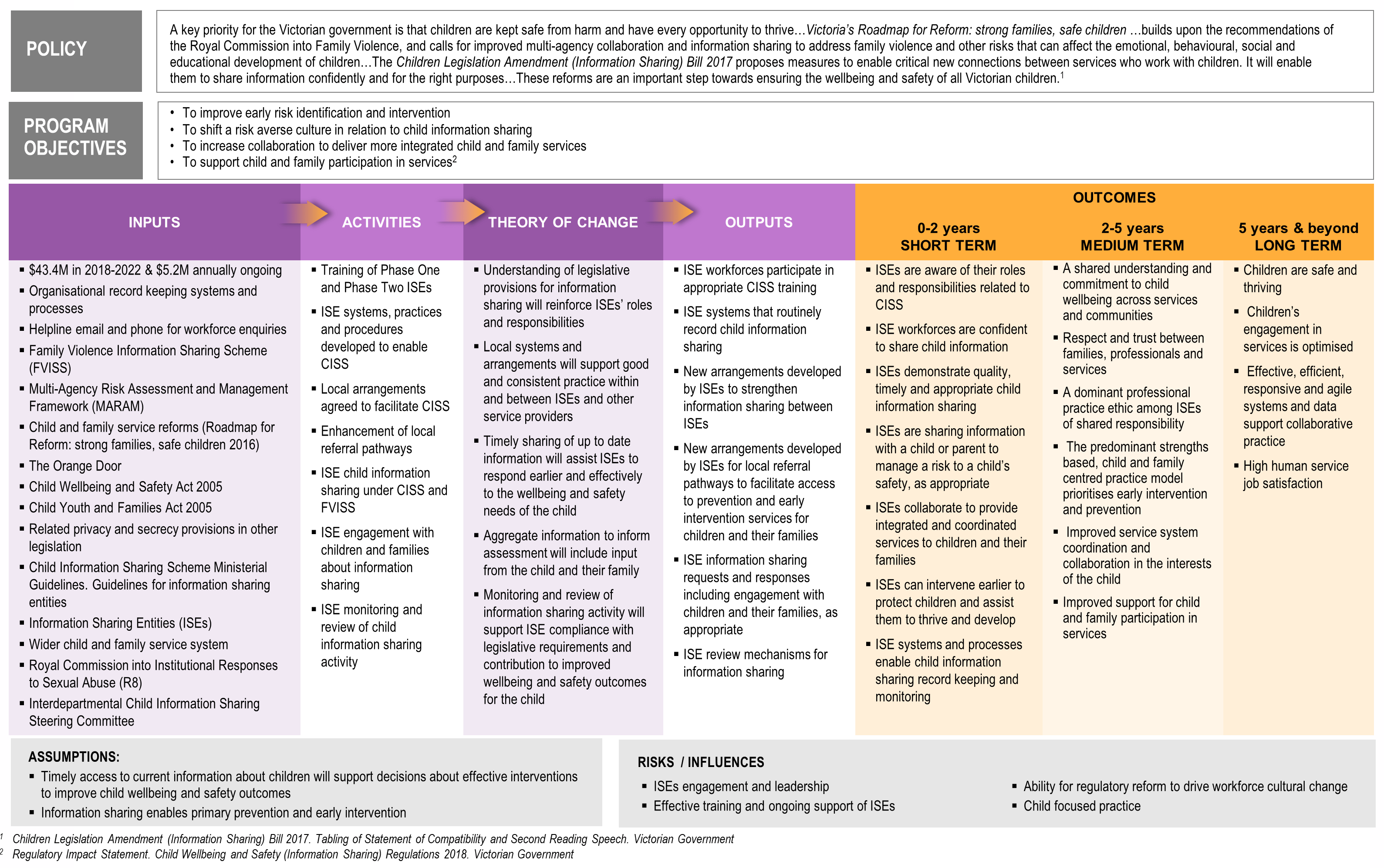{kind=link}
| Policy |
|---|
|
A key priority for the Victorian government is that children are kept safe from harm and have every opportunity to thrive…Victoria’s Roadmap for Reform: strong families, safe children …builds upon the recommendations of the Royal Commission into Family Violence, and calls for improved multi-agency collaboration and information sharing to address family violence and other risks that can affect the emotional, behavioural, social and educational development of children…The Children Legislation Amendment (Information Sharing) Bill 2017 proposes measures to enable critical new connections between services who work with children. It will enable them to share information confidently and for the right purposes…These reforms are an important step towards ensuring the wellbeing and safety of all Victorian children. [1] |
| Program objectives |
|---|
|
| Inputs | Activities | Theory of change | Outputs |
|---|---|---|---|
|
|
|
|
| Outcomes | ||
|---|---|---|
| 0-2 years SHORT TERM |
2-5 years MEDIUM TERM |
5 years & beyond LONG TERM |
|
|
|
|
Assumptions |
|---|
|
| Risks / influences |
|---|
|
[1] Children Legislation Amendment (Information Sharing) Bill 2017. Tabling of Statement of Compatibility and Second Reading Speech. Victorian Government
[2] Regulatory Impact Statement. Child Wellbeing and Safety (Information Sharing) Regulations 2018. Victorian Government
Appendix C: Prescribed workforces surveys: respondent profile
Appendix C for the Child Information Sharing Scheme Two-Year Review report.
| Profile Details | Repeat Respondents | New Respondents | ||
|---|---|---|---|---|
| n=194 | % | n=50 | % | |
| Age | ||||
| 21-39 years | 28 | 14% | 11 | 22% |
| 40-49 years | 63 | 32% | 14 | 28% |
| 50-59 years | 61 | 31% | 19 | 38% |
| 60+ | 33 | 17% | 3 | 6% |
| Prefer not to say | 9 | 5% | 3 | 6% |
| Gender | ||||
| Male | 26 | 13% | 6 | 12% |
| Female | 162 | 84% | 42 | 84% |
| Prefer not to say | 6 | 3% | 2 | 4% |
| Participated in the CISS training | 186 | 96% | 48 | 96% |
| In Person | 170 | 88% | 42 | 84% |
| Online | 8 | 4% | 3 | 6% |
| Other | 8 | 4% | 3 | 6% |
| Did not participate in the CISS training | 7 | 4% | 2 | 4% |
| Don’t know if they participated in the CISS training | 1 | 1% | 0 | 0% |
| Program Area | ||||
| Maternal & Child Health | 44 | 23% | 11 | 22% |
| Family Services | 33 | 17% | 12 | 24% |
| Alcohol and Other Drug Services | 23 | 12% | 3 | 6% |
| Mental Health Services | 21 | 11% | 3 | 6% |
| Family Violence Therapeutic Responses and Counselling | 10 | 5% | 3 | 6% |
| Specialist Victim Survivor Family Violence Service | 10 | 5% | 3 | 6% |
| Out of Home Care | 10 | 5% | 3 | 6% |
| Homelessness Services | 9 | 5% | 3 | 6% |
| Orange Door (Support and Safety Hub) | 7 | 4% | 1 | 2% |
| Other* | 23 | 14% | 8 | 16% |
| Unspecified | 4 | 2% | 0 | 0% |
| *’other’ includes health, human services justice, police and family violence program areas *because of rounding, percentages may not add up to 100% |
||||
| Role | % of respondents (repeat respondents n=194) |
|---|---|
| Manager / director | 29% |
| Team leader / practice leader | 18% |
| Coordinator | 10% |
| Other welfare or medical professional | 15% |
| Other care / support worker | 9% |
| Nurse | 6% |
| Case manager / case worker | 6% |
| Other | 5% |
| Unsure/rather not say | 3% |
| *because of rounding, percentages may not add to 100% | |
Appendix D: Data collection tools
Appendix D for the Child Information Sharing Scheme Two-Year Review report.
D.1 Phase One 2019 prescribed workforces survey (baseline)
Attitudes towards information sharing at your organisation
We are interested in the general attitudes of staff at your organisation. These questions refer to the 12 month period up until the commencement of the Child Information Sharing Scheme, 27 September 2018.
Q5 How strongly do you agree or disagree with the following statements?
Generally, staff at my organisation…
- were open to sharing information with other agencies within the legal frameworks prior to CISS
- were aware of their legal responsibilities when sharing information
- knew where to go for guidance on how to share information
- understood how information sharing could benefit children
- were reluctant to share information, in the fear that they may be doing the wrong thing
- promoted information sharing to others, where it may be of benefit, within the existing legal frameworks
Strongly agree / Agree / Neither agree nor disagree / Disagree / Strongly disagree / Prefer not to say
Q6 Up until October 2018, did your organisation have policies covering the sharing of children’s information with external organisations?
Yes / No / Prefer not to say
IF YES ASK Q7, ELSE SKIP TO DISQ8
Q7 How strongly do you agree or disagree with the following statements?
As at October 2018, my organisation’s policies governing the sharing of children’s information…
- were up to date
- provided clear guidance on when information sharing was permissible
- were flexible enough to be applied across many of the situations likely to be encountered
- enabled exchange of certain children’s information, between our organisation and other permitted entities
- were widely adhered to by relevant staff within the organisation
- may sometimes have hindered early identification of needs and issues or early prevention of issues
Strongly agree / Agree / Neither agree nor disagree / Disagree / Strongly disagree / Prefer not to say
Baseline: information sharing with other agencies
PREQ8 For these next few questions, we’d like you to explore the ways in which your organisation shared information about children with other agencies or individuals, either proactively, or in response to a request to share, up until October 2018.
This section does not cover other agencies sharing information with your agency. We will cover that in later sections of the survey.
Q8 Did you share information about children with other agencies or individuals in the 12 months to October 2018?
Yes / No / Prefer not to say
IF YES ASK Q8B, ELSE SKIP TO Q9
Q8B Was this sharing of information mostly on a proactive basis, or in response to requests from other agencies? Or was it an even mix of both?
Mostly proactive / Mostly in response to requests / Even mix of both / Prefer not to say
IF MOSTLY IN RESPONSE TO REQUESTS ASK Q9, ELSE SKIP TO DISQ19
Q9 What was the main reason for not sharing information
Verbatim / Prefer not to say / Don’t know
IF YES SELECTED AT Q8 ASK Q10, ELSE SKIP TO DISQ19
Q10 What type of agencies did you share information with?
Verbatim / Other / Prefer not to say
Q11 What type of information did you share and why?
Note, we are interested in the types of information you shared, not specific examples.
Verbatim / Prefer not to say / Don’t know
Q12 Which of the following communication methods did you most commonly use to share information?
Telephone / Electronic (email) / Face to face / Specific Form (hardcopy or email) / Other (Specify) / Prefer not to say
Q13 [IF MULTIPLE AT Q12] Of the communication methods that you used, which one is your preferred one?
Telephone / Electronic (email) / Face to face / Specific Form (hardcopy or email) / Other (Specify) / Prefer not to say
Q14 On average how frequently did you provide information to other agencies or individuals in the 12 months up until October 2018?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Other (Specify) / Prefer not to say / Don’t know
Q15 On a scale of zero to ten, where zero is ‘not at all effective’ and ten is ‘extremely effective’, overall, how effective do you feel your organisation was in providing information to support the wellbeing of children during the 12 month period up until October 2018?
0-10 / Prefer not to say (GO TO Q16A) / Don’t know (GO TO Q16A)
Q16 Why do you say that?
Verbatim / Prefer not to say / Don’t know
Q16A In the 12 month period up until October 2018, did you ever encounter a situation where you determined a need to provide information to promote the wellbeing of a child, but could not act on this due to legal restrictions or organisational policies?
Yes / No / Don’t know / can’t recall
If YES ASK Q16B, ELSE SKIP TO Q17
Q16B Approximately how often did this occur?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Other (Specify) / Prefer not to say / Don’t know
Q17 Approximately how often did your organisation refuse an external request for information sharing?
Never / Occasionally / Most of the time / All of the time / Other (Specify) / Prefer not to say
IF OCCASIONALLY, MOST OF THE TIME, ALL OF THE TIME, ASK Q18, ELSE SKIP TO PREQ19
Q18 What were the most common reasons for refusing a request to share information? [MR]
Proper process/system not followed / The information requested could not legally be shared / The information requested was deemed as not relevant for sharing / The procedures in place were too onerous to justify the time it would take to share information / Privacy had to be prioritised over the wellbeing of the child / Did not have the necessary consent to share / Did not have confidence about the legal obligations in relation to privacy / Other concerns about privacy / Other (Specify) / Prefer not to say / Don’t know
Baseline: other agencies sharing information with your organisation
PREQ19 For these next few questions, we’d like you to explore the ways in which other agencies shared information about children with your organisation, up until October 2018.
Q19 Did you request information about children from other agencies or individuals in the 12 months to October 2018?
Yes / No / Prefer not to say
IF NO ASK Q20, ELSE SKIP TO Q21
Q20 What was the main reason for not requesting information?
Verbatim / Prefer not to say / Don’t know
IF YES SELECTED AT Q19 ASK Q21, ELSE SKIP TO DISQ32
Q21 What type of agencies did you request information from?
Verbatim / Other / Prefer not to say
Q22 What type of information did you request and why?
Note, we are interested in the types of information you requested, not specific examples.
Verbatim / Prefer not to say / Don’t know
Q23 Through which of the following communication methods did you most commonly receive information you had requested?
Telephone / Electronic (email) / Face to face / Specific Form (hardcopy or email) / Prefer not to say
Q24 [IF MULTIPLE AT Q23] Of the communication methods which you received information from, which one is your preferred method?
Telephone / Electronic (email) / Face to face / Specific Form (hardcopy or email) / Prefer not to say
Q25 Approximately how frequently did you request information from other agencies in the 12 months up until October 2018?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Other (Specify) / Prefer not to say / Don’t know
Q26 On a scale of zero to ten, where zero is ‘not at all effective’ and ten is ‘extremely effective’, overall, how effective do you feel these other agencies were in providing information to support the wellbeing of children during the 12-month period up until October 2018?
IF 0 TO 10 AT Q26 ASK Q27, ELSE ASK Q27B
Q27 Why do you say that?
Verbatim / Prefer not to say / Don’t know
Q27b In the 12 month period up until October 2018, did you ever encounter a situation where you determined a need to request information to promote the wellbeing of a child, but you could not act on this or were denied access to the information due to legal restrictions or organisational policies?
Yes / No / Don’t know / can’t recall
IF YES ASK Q27C ELSE SKIP TO Q28
Q27c Approximately how often did this occur?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Other (Specify) / Prefer not to say / Don’t know
Q28 On a scale from zero to ten where zero means ‘totally inaccurate’ and ten is ‘totally accurate’, in your opinion, overall, how accurate is the information that you receive from other agencies or individuals?
0-10 / Prefer not to say / Don’t know
Q29 On a scale from zero to ten where zero means ’not at all relevant’ and ten is ’completely relevant’, in your opinion, overall, how relevant is the information that you receive from other agencies or individuals?
0-10 / Prefer not to say / Don’t know
Q30 Approximately how often were you refused a request for information by another agency or individual?
Never / Occasionally / Most of the time / All of the time / Other (Specify) / Prefer not to say
IF CODE OCCASIONALLY, MOST OF THE TIME, ALL OF THE TIME SELECTED AT Q30 ASK Q31, ELSE SKIP TO DISQ32
Q31 As far as you are aware, what were the most common reasons for refusing a request to share information?
Proper process/system not followed / The information requested could not legally be shared / The information requested was deemed as not relevant for sharing / The procedures were too onerous to justify the time it would take to share information / Privacy had to be prioritised over the wellbeing of the child / Did not have necessary consent to share / Did not have full confidence about the legal obligations in relation to privacy / Other concerns about privacy / Other (Specify) / Prefer not to say / Don’t know
Adjusting to the CIS Scheme
The CIS scheme has now been in effect since late 2018. These next few questions relate to your current experience, now that the scheme has been in place for some time.
Q32 As far as you are aware, do your current information sharing practices align with the requirements under the CIS Scheme?
Yes / No / Don’t know / Prefer not to say
Q33 Which processes/systems/attitudes have required the biggest changes to align with the CIS Scheme?
Verbatim / Prefer not to say / Don’t know
Q34 What, in your view, are the benefits of the CIS Scheme to your organisation, to prescribed service workers, and to children and families that receive your services?
Verbatim / Prefer not to say / Don’t know
Q35 What, in your view, are the challenges of the CIS Scheme for your organisation, for prescribed service workers and for the children and families that receive your services?
Verbatim / Prefer not to say / Don’t know
Q35b Have you observed any of those benefits or challenges playing out to date?
Yes / No / Don’t know / Prefer not to say
IF YES ASK Q35C ELSE SKIP TO Q36
Q35c Please describe any of these benefits and/or challenges that have played out for your organisation.
Verbatim / Prefer not to say / Don’t know
Q36 On a scale from zero to ten where zero means ‘very little effort’ and ten means ‘an extremely high level of effort’, overall, how much effort has your organisation needed to expend in aligning practices, procedures and systems to the CIS Scheme?
0-10 / Prefer not to say / Don’t know
The FVIS Scheme
Q37 Have you participated in the Family Violence Information Sharing Scheme (FVISS) Training?
Yes / No / Don’t know / Prefer not to say
IF YES ASK Q38, ELSE SKIP TO Q39
Q38 On average how frequently have you shared information with other agencies over the past six months, under the FVISS?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Never – have not shared information under the FVISS / Other (Specify) / Prefer not to say / Don’t know
Q39 Are there any lessons for the CIS Scheme that can be drawn from your experience of the FVISS?
Verbatim / Prefer not to say / Don’t know
Demographics
Now we have a few questions about yourself.
Q40 What is your age?
18-20 years / 21-29 years / 30-39 years / 40-49 years / 50-59 years / 60+ / Prefer not to say
Q41 Are you?
Male / Female / Prefer not to say
Recruitment permissions
Q42 Those were all the questions we have to ask you. Is there anything further you would like to add that has not been covered?
Verbatim / No
Q43 Finally, we’d like to invite you to participate in an additional interview. At this stage we are just asking survey participants from a selection of organisations if they would be prepared to take part. It would involve a simple telephone interview of about 30 minutes where we would have a conversation about your experiences with the Child Information Sharing Scheme in more detail. Your identity will be kept confidential.
Would you be willing to participate in this additional interview?
Yes / No
Close
Thank you for your time. This market research is carried out in compliance with the Privacy Act, and the information you provided will be used for research purposes only.
We will be in touch with you (or your organisation) again in 2020 to conduct a short follow-up survey.
If you have any questions related to prescription, the Child Information Sharing Scheme has an enquiry line that you can call on 1800 549 646 which operates Monday to Friday 10am to 2pm. Alternatively, the team can be reached at childinfosharing@edumail.vic.gov.au.
If you require any further information about the study or if you’d like to find out how we manage your personal information, you can call Wallis on 1800 113 444 or view the Wallis Privacy Policy on at www.wallisgroup.com.au/privacy-policy/.
Just to re-iterate, approval for this research project has been gained through the Human Research Ethics Committee at the University of Queensland (Approval Number: 2018002181).
D.2 Phase One 2020 prescribed workforces survey (follow-up)
Towards information sharing at your organisation
We are interested in the general attitudes of staff at your organisation now that the Child Information Sharing Scheme has been implemented for more than a year.
Q5 How strongly do you agree or disagree with the following statements?
Generally, staff at my organisation…
- are open to sharing information with other agencies within the existing legal frameworks
- are aware of their legal responsibilities when sharing information
- know where to go for guidance on how to share information
- understand how information sharing could benefit children
- are reluctant to share information, in the fear that they may be doing the wrong thing
- promote information sharing to others, where it may be of benefit, within the existing legal frameworks
Strongly agree / Agree / Neither agree nor disagree / Disagree / Strongly disagree / Prefer not to say
Q6 Does your organisation have policies covering the sharing of children’s information with external organisations?
Yes / No / Prefer not to say
IF YES ASK Q7, ELSE SKIP TO QCOV
Q7 How strongly do you agree or disagree with the following statements?
Currently, my organisation’s policies governing the sharing of children’s information…
- are up to date
- provide clear guidance on when information sharing is permissible
- are flexible enough to be applied across many of the situations likely to be encountered
- enable exchange of certain children’s information, between our organisation and other permitted entities
- are widely adhered to by relevant staff within the organisation
- may sometimes hinder early identification of needs and issues or early prevention of issues
Strongly agree / Agree / Neither agree nor disagree / Disagree / Strongly disagree / Prefer not to say
Follow-up: information sharing with other agencies
Q_COV This next section of the survey will explore the ways in which your organisation has shared information about children. But firstly, we understand that the COVID-19 pandemic will have disrupted the way many services are operating.
Please can you describe any impact on the sharing of information about children, as a result of changed practices due to the Coronavirus?
Verbatim / No changes to information sharing as a result of the COVID-19 pandemic / Prefer not to say / Don’t know
PREQ8 For these next few questions, we’d like you to explore the ways in which your organisation shared information about children with other agencies or individuals, either proactively, or in response to a request to share, over the past 12 months.
This section does not cover other agencies sharing information with your agency. We will cover that in later sections of the survey.
Q8 Did you share information about children with other agencies or individuals in the past 12 months?
Yes / No / Prefer not to say
IF YES ASK Q8B, ELSE SKIP TO Q9
Q8B Was this sharing of information mostly on a proactive basis, or in response to requests from other agencies? Or was it an even mix of both?
Mostly proactive / Mostly in response to requests / Even mix of both / Prefer not to say
IF NO AT Q8 ASK Q9, ELSE SKIP TO DISQ19
Q9 What was the main reason for not sharing information
Verbatim / Prefer not to say / Don’t know
IF YES AT Q8 ASK Q10, ELSE SKIP TO DISQ19
Q10 What type of agencies did you share information with?
Verbatim / Other / Prefer not to say
Q11 What type of information did you share and why?
Note, we are interested in the types of information you shared, not specific examples.
Verbatim / Prefer not to say / Don’t know
Q12 Which of the following communication methods did you most commonly use to share information
Telephone / Electronic (email) / Face to face / Specific Form (hardcopy or email) / Other (Specify) / Prefer not to say
Q13 [IF MULTIPLE AT Q12] Of the communication methods that you used, which one is your preferred one?
Telephone / Electronic (email) / Face to face / Specific Form (hardcopy or email) / Other (Specify) / Prefer not to say
Q14 On average how frequently did you provide information to other agencies or individuals in the last 12 months?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Other (Specify) / Prefer not to say / Don’t know
Q15 On a scale of zero to ten, where zero is ‘not at all effective’ and ten is ‘extremely effective’, overall, how effective do you feel your organisation is in providing information to support the wellbeing of children during the last 12 month period?
0-10 / Prefer not to say / Don’t know
Q16 Why do you say that?
Verbatim / Prefer not to say / Don’t know
Q16A In the last 12 month period, did you ever encounter a situation where you determined a need to provide information to promote the wellbeing of a child, but could not act on this due to legal restrictions or organisational policies?
Yes / No / Don’t know / can’t recall
IF YES ASK Q16B, ELSE SKIP TO Q17
Q16B Approximately how often did this occur?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Other (Specify) / Prefer not to say / Don’t know
Q17 Approximately how often did your organisation refuse an external request for information sharing?
Never / Occasionally / Most of the time / All of the time / Other (Specify) / Prefer not to say
IF OCCASIONALLY, MOST OF THE TIME OR ALL OF THE TIMESELECTED ASK Q18, ELSE SKIP TO PREQ19
Q18 What were the most common reasons for refusing a request to share information?
Proper process/system not followed / The information requested could not legally be shared / The information requested was deemed as not relevant for sharing / The procedures in place were too onerous to justify the time it would take to share information / Privacy had to be prioritised over the wellbeing of the child / Did not have the necessary consent to share / Did not have confidence about the legal obligations in relation to privacy / Other concerns about privacy / Other (Specify) / Prefer not to say / Don’t know
Follow-up: other agencies sharing information with your organisation
PREQ19 For these next few questions, we’d like you to explore the ways in which other agencies shared information about children with your organisation over the past 12 months.
Q19 Did you request information about children from other agencies or individuals in the past 12 months?
Yes / No / Prefer not to say
IF NO ASK Q20, ELSE SKIP TO Q21
Q20 What was the main reason for not requesting information?
Verbatim / Prefer not to say/ Don’t know
IF YES AT Q19 ASK Q21, ELSE SKIP TO Q32
Q21 What type of agencies did you request information from?
Verbatim / Other / Prefer not to say
Q22 What type of information did you request and why?
Note, we are interested in the types of information you requested, not specific examples.
Verbatim / Prefer not to say / Don’t know
Q23 Through which of the following communication methods did you most commonly receive information you had requested?
Telephone / Electronic (email) / Face to face / Specific Form (hardcopy or email) / Other (Specify) / Prefer not to say
Q24 [IF MULTIPLE AT Q23] Of the communication methods which you received information through, which one is your preferred method?
Telephone / Electronic (email) / Face to face / Specific Form (hardcopy or email) / Other (Specify) / Prefer not to say
Q25 Approximately how frequently did you request information from other agencies in the past 12 months?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Other (Specify) / Prefer not to say / Don’t know
Q26 On a scale of zero to ten, where zero is ‘not at all effective’ and ten is ‘extremely effective’, overall, how effective do you feel these other agencies were in providing information to support the wellbeing of children during the past 12-months?
0-10 / Prefer not to say / Don’t know
IF 0-10 ASK Q27, ELSE ASK Q27B
Q27 Why do you say that?
Verbatim / Prefer not to say / Don’t know
Q27b In the past 12 months, did you ever encounter a situation where you determined a need to request information to promote the wellbeing of a child, but you could not act on this or were denied access to the information due to legal restrictions or organisational policies?
Yes / No / Don’t know / can’t recall
IF YES ASK Q27C ELSE SKIP TO Q28
Q27c Approximately how often did this occur?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Other (Specify) / Prefer not to say / Don’t know
Q28 On a scale from zero to ten where zero means ‘totally inaccurate’ and ten is ‘totally accurate’, in your opinion, overall, how accurate is the information that you receive from other agencies or individuals?
0-10 / Prefer not to say / Don’t know
Q29 On a scale from zero to ten where zero means ’not at all relevant’ and ten is ’completely relevant’, in your opinion, overall, how relevant is the information that you receive from other agencies or individuals?
0-10 / Prefer not to say / Don’t know
Q30 Approximately how often were you refused a request for information by another agency or individual?
Never / Occasionally / Most of the time / All of the time / Other (Specify) / Prefer not to say
IF OCCASIONALLY, MOST OF THE TIME OR ALL OF THE TIME ASK Q31, ELSE SKIP TO DISQ32
Q31 As far as you are aware, what were the most common reasons for refusing a request to share information?
Proper process/system not followed / The information requested could not legally be shared / The information requested was deemed as not relevant for sharing / The procedures were too onerous to justify the time it would take to share information / Privacy had to be prioritised over the wellbeing of the child / Did not have necessary consent to share / Did not have full confidence about the legal obligations in relation to privacy / Other concerns about privacy / Other (Specify) / Prefer not to say / Don’t know
Adjusting to the CIS Scheme
The CIS scheme has now been in effect since late 2018. These next few questions relate to your current experience.
Q32 As far as you are aware, do your current information sharing practices align with the requirements under the CIS Scheme?
Yes / No / Don’t know / Prefer not to say
Q33 Which processes/systems/attitudes have required the biggest changes to align with the CIS Scheme?
Verbatim / Prefer not to say / Don’t know
Q34 What, in your view, are the benefits of the CIS Scheme to your organisation, to prescribed service workers, and to children and families that receive your services?
Verbatim / Prefer not to say / Don’t know
Q35 What, in your view, are the challenges of the CIS Scheme for your organisation, for prescribed service workers and for the children and families that receive your services?
Verbatim / Prefer not to say / Don’t know
Q35b Have you observed any of those benefits or challenges playing out to date?
Yes / No / Don’t know / Prefer not to say
IF YES ASK Q35C ELSE SKIP TO Q36
Q35c Please describe any of these benefits and/or challenges that have played out for your organisation.
Verbatim / Prefer not to say / Don’t know
Q36 On a scale from zero to ten where zero means ‘very little effort’ and ten means ‘an extremely high level of effort’, overall, how much effort has your organisation needed to expend in aligning practices, procedures and systems to the CIS Scheme?
0-10 / Prefer not to say / Don’t know
The FVIS Scheme
Q37 Have you participated in the Family Violence Information Sharing Scheme (FVISS) Training?
Yes / No / Don’t know / Prefer not to say
IF YES ASK Q38, ELSE SKIP TO Q39
Q38 On average how frequently have you shared information with other agencies over the past six months, under the FVISS?
Daily, or most days / A few times per week / Weekly / A few times per month / Once a month / Once every 2-3 months / Less frequently than once every 3 months / Never – have not shared information under the FVISS / Other (Specify) / Prefer not to say / Don’t know
Q39 Are there any lessons for the CIS Scheme that can be drawn from your experience of the FVISS?
Verbatim / Prefer not to say / Don’t know
Demographics
Now we have a few questions about yourself.
Q40 What is your age?
18-20 years / 21-29 years / 30-39 years / 40-49 years / 50-59 years / 60+ / Prefer not to say
Q41 Are you?
Male / Female / Prefer to self-describe / Prefer not to say
Close
Thank you for your time. This market research is carried out in compliance with the Privacy Act, and the information you provided will be used for research purposes only.
This survey was undertaken by Wallis Market & Social Research on behalf of the Victorian Department of Education and Training.
If you have any questions related to prescription, the Child Information Sharing Scheme has an enquiry line that you can call on 1800 549 646 which operates Monday to Friday 10am to 2pm. Alternatively, the team can be reached at childinfosharing@edumail.vic.gov.au.
If you require any further information about the study or if you’d like to find out how we manage your personal information, you can call Wallis on 1800 113 444 or view the Wallis Privacy Policy at www.wallisgroup.com.au/privacy-policy/.
Just to re-iterate, approval for this research project has been gained through the Human Research Ethics Committee at the University of Queensland (Approval Number: 2018002181).
Appendix E: Phase One prescribed information sharing entities
Appendix E for the Child Information Sharing Scheme Two-Year Review report.
The following lists identify Phase One information sharing entities prescribed under the Child Information Sharing Scheme[30]. The majority of entities are prescribed under all three information sharing reforms (E.1) with an additional small number of entities prescribed under both (E.2) information sharing schemes or the Child Information Sharing Scheme only. For completeness, prescribed entities under the family violence reforms only who formed part of the Initial Tranche of prescribed entities (February 2018) in the phased implementation of the Family Violence Information Sharing Scheme have also been listed (E.4).
E.1 Information sharing entities (ISEs) prescribed under Child Information Sharing Scheme (CISS), Family Violence Information Sharing Scheme (FVISS) and Multi-Agency Risk Assessment and Management (MARAM) Framework, including Risk Assessment Entities (RAEs)
- Child FIRST (RAE)
- Child Protection (RAE)
- Department of Health and Human Services Housing
- Designated mental health services
- Justice Health
- Justice Health's funded services for young people
- Maternal and Child Health Services
- Multi-Agency Panels to Prevent Youth Offending
- Out-of-home care services
- Perpetrator intervention trials
- Registered community-based child and family services
- Risk Assessment and Management Panels (RAE)
- State-funded specialist family violence services including family violence counselling, therapeutic programs and perpetrator intervention (RAE)
- State-funded alcohol and other drugs services
- State-funded homelessness accommodation or homelessness support services (providing access point, outreach and accommodation services)
- State-funded sexual assault services (RAE)
- State-funded sexually abusive behaviour treatment services
- The Orange Door (Support and Safety Hubs) (RAE)
- Victims Assistance Program-funded services (RAE)
- Victoria Police (RAE)
- Victims of Crime Helpline (RAE)
- Youth Justice and funded programs, including the Youth Parole Board (Secretariat)
E.2 ISEs prescribed under CISS and FVISS only
- Commissioner for Children and Young People
- Disability Services Commissioner
E.3 ISEs prescribed under CISS only
- Registry of Births, Deaths and Marriages
E.4 ISEs prescribed under FVISS and MARAM only
- Adult Parole Board
- Children’s Court officials
- Corrections Victoria and Corrections funded services
- Court-ordered family violence counselling services
- Justice Health's funded services for adults
- Magistrates’ Court officials
- State-funded financial counselling programs
- Tenancy Advice and Advocacy Program
[30] Victorian government. About Information Sharing and MARAM reforms. https://www.vic.gov.au/about-information-sharing-schemes-and-risk-management-framework.