- Published by:
- Family Safety Victoria
- Date:
- 21 Mar 2021
Executive summary
Family violence is an endemic issue, which can have terrible consequences for individuals, families and communities.
Family violence is an endemic issue, which can have terrible consequences for individuals, families and communities. The Victorian Government launched Australia’s first Royal Commission into Family Violence in February 2015 to address the scale and impact of this crime in Victoria.
The Royal Commission into Family Violence (the Commission) held 25 days of public hearings; it commissioned research and held community conversations with more than 800 Victorians. It also received almost 1000 written submissions. The Commission provided a once-in-a-generation opportunity to examine our system from the ground up and put victim survivors at the centre of family violence reform.
The Commission delivered its report in March 2016, with 227 recommendations. The Commission outlined a vision for a Victoria that is free from family violence, where adults, young people and children are safe and where their wellbeing and needs are responded to, and where perpetrators are held to account for their actions and behaviours. Where family violence does occur, the Commission outlined how reform of the service system could provide consistent, collaborative approaches to risk identification, assessment and management.
The Commission noted the strong foundations of the service system and practice environment that had been built by the Family Violence Risk Assessment and Risk Management Framework, also known as the Common Risk Assessment Framework or CRAF. To address key gaps and issues, it recommended a review and redevelopment of the CRAF, and to embed it into the Family Violence Protection Act 2008 (Vic) (the FVPA).
The Victorian Family Violence Multi-Agency Risk Assessment and Management Framework (MARAM Framework) updates and replaces the CRAF and is informed by consultations with more than 1650 practitioners and subject matter experts, and evidence-base reviews. In addition to the Commission’s findings and recommendations, the redevelopment was also informed by the Coronial Inquest into the death of Luke Geoffrey Batty and the 2016 Review of the CRAF.
More than 855 organisations and 37,500 professionals are currently prescribed to align their policies, procedures, practice guidance and tools to the MARAM Framework.1 Further organisations will be prescribed from 2020.
Fundamental changes identified by the Commission are reflected in the aims for the MARAM Framework. These include:
- Increase the safety of people experiencing family violence
- Ensure the broad range of experiences and spectrum of risk are represented, including for Aboriginal and diverse communities, children, young people and older people, across identities, and family and relationship types
- Keep perpetrators in view and hold them accountable for their actions and behaviours
- Alignment of practice across a broad range of organisations who have responsibilities to identify, assess and manage family violence risk
- Ensure consistent use of the Framework across organisations and sectors.
The MARAM Framework outlines:
- An approach to practice which is underpinned by the Framework Principles
- Four conceptual ‘pillars’ for organisations to align their policies, procedures, practice guidelines and tools.
- Information to support a shared understanding of the experience of risk and its impact on individuals, families and communities.
- Expectations of practice that are underpinned by a shared understanding of the range of roles across the service system, and consistent and collaborative practice.
- An expansion of the range of organisations and sectors who will have a formal role in family violence risk assessment and risk management practice.
A summary of these elements is described in the Foundation Knowledge Guide (below) to provide background for individual professionals and services.
This document contains the MARAM Practice Guides which underpin the MARAM Framework. These resources are provided in three volumes and are designed for use by professionals and organisational leaders:
- The Foundation Knowledge Guide which focuses on the legislative context, roles and interactions with the service system, risk factors, key concepts for practice and presentations of risk across different age groups and Aboriginal and diverse communities. The Foundation Knowledge Guide is required reading for all professionals across leadership and governance, management and supervision to direct practice roles. Professionals should be familiar with this introductory and supporting information prior to engaging with the MARAM Responsibilities for Practice Guide
- The Responsibilities for Practice Guide reflects each of the ten responsibilities of practice set out in the MARAM Framework. This guide focuses on how to apply foundation knowledge and then build on this to provide practice guidance from safe engagement, identification of risk, through levels of risk assessment and management, secondary consultation and referral, information sharing, and multi-agency and coordinated practice. Professionals’ responsibilities will vary based on the nature of their role within a service or organisation and will be informed by the contact they may have with victim survivors and perpetrators. Professionals should work with their organisational leaders to understand their role and to identify which responsibilities they should be applying in practice. Professionals are required to be familiar with each of the responsibilities that are a part of their role
- The Organisational embedding guide supports organisational leaders to effectively support professionals and services to undertake their roles and responsibilities. This will link the work undertaken by professionals and services to the alignment of organisations’ policies, procedures, practice guidance and tools under the MARAM Framework. Professionals in leadership or management roles should be familiar with the Organisational embedding guide. In addition to responding to the requirements for alignment under the MARAM Framework, organisational leaders should assist professionals and services within their organisations to identify and use the practice guides appropriate to their roles.
All MARAM tools and practice guides were developed through extensive consultation with a range of stakeholders including experts, departmental policy and practice areas, and professionals in specialist and universal services, including those specialising in working with Aboriginal communities, diverse communities, children, young people and older people. The guides will continue to be updated and evaluated to reflect the evolving evidence- base relating to experiences of family violence across the community and shifting practice directions that will contribute to this evidence base.
Responsibility 1: Respectful, sensitive and safe engagement
Responsibility 1 of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
1. Respectful, sensitive and safe engagement
1.1 Overview
This guide should be used to create a respectful, sensitive and safe environment for people who may be experiencing family violence. This includes an emphasis on listening to, partnering with and believing victim survivors as experts in their own experience.
This guide may be used where family violence is already suspected or not and is vital to support disclosure and facilitate identification and screening, which are discussed in Responsibility 2.
Your organisation will have its own policies, practices and procedures relevant to safe engagement. Leaders in your organisation should support you and others to understand and implement these policies, practices and procedures.
Key capabilities
All professionals should use Responsibility 1, which includes understanding:
- The gendered nature and dynamics of family violence (covered in the Foundation Knowledge Guide and the MARAM Framework).
- Respectful, sensitive and safe engagement as part of Structured Professional Judgement.
- How to facilitate an accessible, culturally responsive environment for safe disclosure of information.
- How to respond to disclosures sensitively and prioritise the safety of victim survivors.
- How to tailor engagement with adults, children and young people, including Aboriginal people and people from diverse communities.
- The importance of using a person-centred approach.
- Recognising and addressing barriers that impact a person’s support and safety options.
All information in this guide is relevant for assessing risk to any adult, child or young person who is a victim survivor.
There are additional practice considerations on safe engagement with children and young people in Section 1.10–1.12 of this guide.
Information which refers to a perpetrator in this guide is relevant if an adolescent is using family violence for the purposes of risk assessment with a victim survivor about their experience and the impact of violence. Risk assessment and management for adolescents should always consider their age, developmental stage and individual circumstances, and include therapeutic responses as required.
Remember
The practice guidance across all ten practice responsibilities builds on the Foundation Knowledge Guide which covers the gendered nature and dynamics of family violence, and its impacts. The Foundation Knowledge Guide includes information on practice approaches which complement the information in this guide, including trauma- informed, person-centred practice, applying an intersectional lens, reflective practice and identifying and addressing bias.
1.2 Engagement as part of structure professional judgement
Reflect on the model of Structured Professional Judgement outlined in Section 9.1 of the Foundation Knowledge Guide.
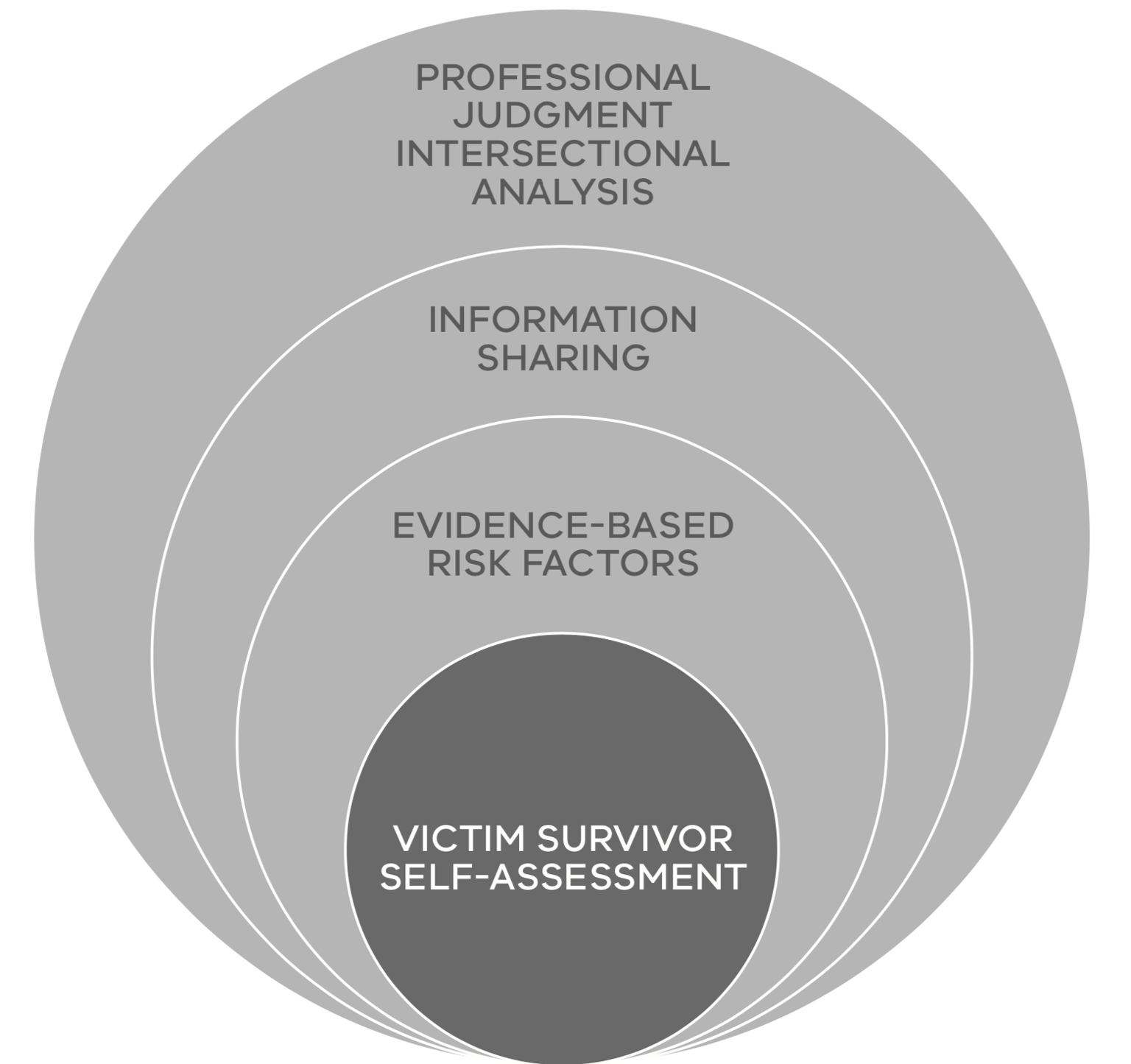
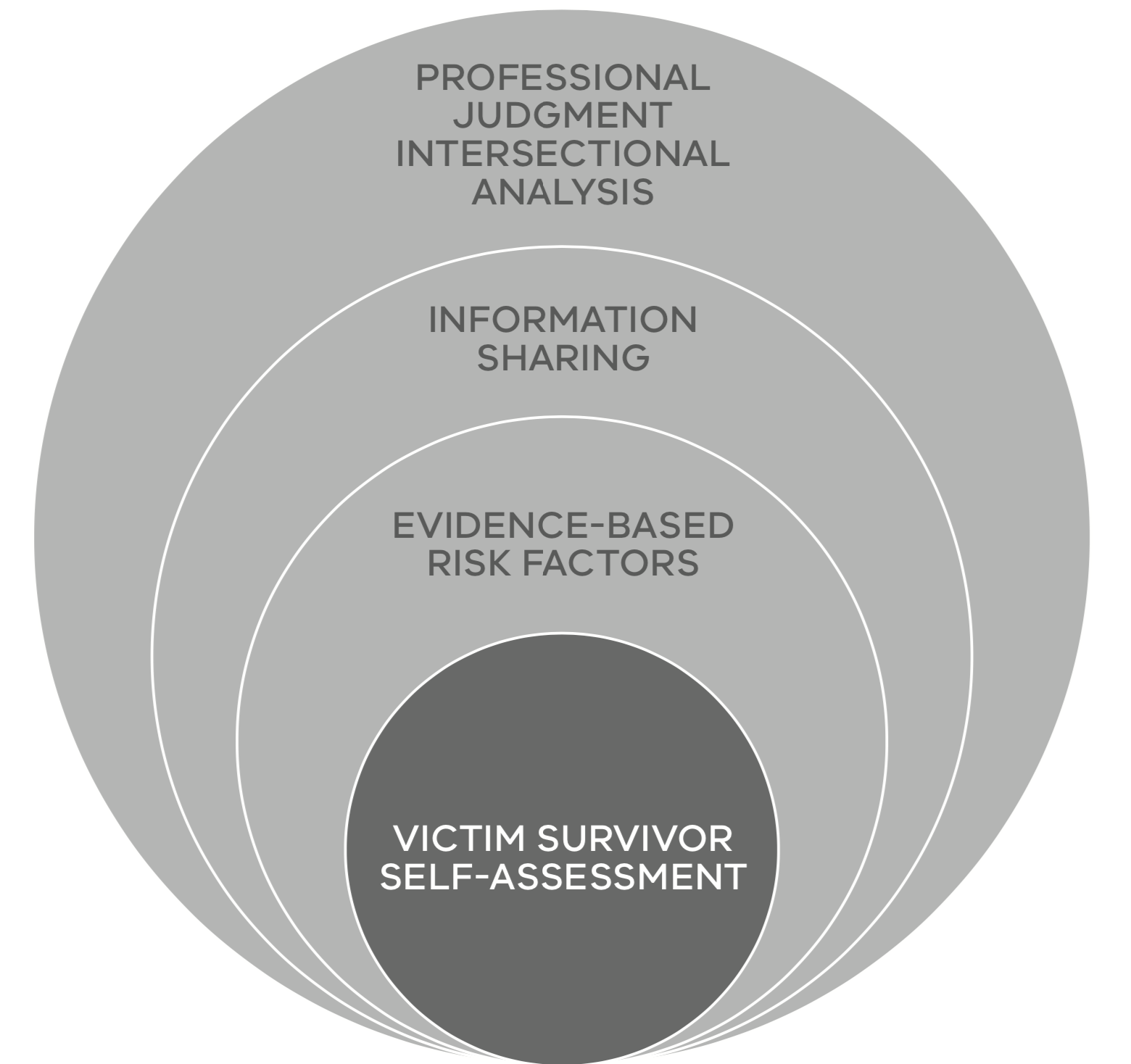
Respectful, sensitive and safe engagement is an important foundation that supports Structured Professional Judgement. This practice creates the trust and rapport with a victim survivor to create an environment where they can feel safe and respected to talk about their experiences of family violence. This underpins the key element of Structured Professional Judgement — facilitating a victim survivor to disclose their self-assessment of their fear, risk and safety, by letting them know they will be believed and supported.
Figure 1: Model of Structured Professional Judgement
{kind=link}
Creating a safe and supportive environment will allow victim survivors to feel believed when they are asked to disclose their self- assessment of fear, risk and safety and whether they hold concerns for other family members’ safety. An adult’s self-assessment of their own level of family violence risk is a strong indicator of the level of risk (see Responsibility 2).
Further information about Structured Professional Judgement will be provided in each of the relevant chapters of the Responsibilities for Practice Guide.
1.3 Creating a safe environment to ask about family violence
Key steps to creating an environment where the person feels safe and respected to talk about their experiences of family violence include considering:
- The immediate health and safety needs of each person (adult or child) who may be experiencing family violence.
- The physical environment, including accessibility
- Communicating effectively, and
- Safely and respectfully responding to the individual’s culture and identity.
1.3.1 Prioritising immediate health and safety
As a first priority, determine if there is an immediate threat to a person’s health or safety. If yes, contact:
- the police or ambulance by calling 000, and/or
- other emergency or crisis services for assistance.
Assessing immediate safety includes both:
- Identifying that a threat is present. This might include situations where the perpetrator is able to access the victim survivor and has made a specific threat or where the specific location of the perpetrator is unknown.
- Determining the likelihood and consequence if immediate action is not taken to lessen or prevent that threat. It may also include facilitating or encouraging access to medical treatment (where physical and sexual violence has occurred).
Further guidance on determining immediate risk to safety from family violence is outlined in Responsibility 2.
Your service or organisation should have established policies and processes in place to manage an immediate threat. If an immediate threat is identified and the whereabouts of the perpetrator is unknown, your service’s safety arrangements could include:
- Conducting interviews in a secure physical environment (see Section 1.3.2), arranging care for children or young people for this to occur, if they are present
- Using the prompting questions and commencing use of the Screening and Identification Tool (Responsibility 2, Appendix 3) or a risk assessment tool to establish the presence of family violence if observable signs of trauma or risk are present (Responsibility 2, Appendix 1)
- Making security or other suitable personnel to be available to prevent the perpetrator entering the premises, and/ or relocating the victim survivor to a safer environment
- If there is an immediate threat, follow your workplace policies and procedures and take any actions necessary, including calling the police.
It may not be appropriate, safe or reasonable to undertake a further risk assessment until any immediate safety risks or health needs are addressed.
1.3.2 Physical environment
The physical environment sets the context for building rapport with the victim survivor
- Make the person feel safe and ask about the things they need to feel comfortable
- Create a safe space — for example, provide physical cues that the client is welcome, and that their culture and other identities will be respected (see Section 1.4 and the Foundation Knowledge Guide).
It is critical that you do not ask questions in the presence of a perpetrator, alleged perpetrator, or adolescent who may be using family violence. Doing so may increase the risk to the victim survivor and any child victim survivors in their care. Using a private environment when asking about sensitive and personal information is critical to establishing rapport with the victim survivor.
If the person suspected of using violence is present, your organisation should have policies and procedures for safely separating them from the victim survivor to provide a private space for conversation. For example, you might ask the person who may be using violence to go to another room by:
- Stating that it is your agency’s standard practice or policy to ask questions in private, or
- You might ask them to complete administration forms.
If the person suspected of using violence is a carer, you may need to arrange alternative communication or support assistance to enable the victim survivor to take part in a safe conversation.
If it is not possible to separate the victim survivor and perpetrator or alleged perpetrator you should consider deferring the conversation about family violence until a safe environment can be established. You may need to consider options on how to re- engage with the victim survivor at another time to support this conversation, such as by booking a follow-up appointment.
When adolescents use family violence against a parent, carer, sibling or other family member, a parent or carer may wish to be engaged in the service along with the adolescent. You should seek the victim survivor’s views and prioritise their safety when considering how to engage in these situations. Keep in mind that adolescents who use violence may also be currently experiencing or have experienced past family violence. Adolescents should always be provided with support that considers their age and developmental stage and circumstances, and be considered for therapeutic responses. Further information on working with adolescents who use family violence is in Responsibility 7 and in the Foundation Knowledge Guide at Section 11.2.
1.3.3 Communication
Creating a safe environment means actively listening with empathy and without judgement. Validate the information provided by showing you believe the victim survivor and are seeking to understand their experience, so you can work together to find ways to help.
As a basis for building a relationship of trust, you should provide key information for example, about what you/your service is there to provide, and clearly set expectations. Always consider the communication needs of any child or young person who is a victim survivor, seeking their views as appropriate, safe and reasonable and validating their unique experiences.
As a priority, ensure that the person can communicate with you. You should consider and make efforts to address any barriers to communication, including those relating to English language proficiency, or for people with disabilities requiring communication adjustments or supports. For example, ensure that you:
- Engage in a culturally sensitive and respectful manner — for example, you could ask if they would like support from a bi-cultural or bilingual worker or services from an Aboriginal organisation. You should adjust to the level of engagement that is comfortable to the person. For example, eye contact is desirable in many cultures and for many people but not all. Consider how the person is engaging with you and be aware that reluctance to make eye contact is not a sign of evasiveness. You should give the person the opportunity to voice their preference regarding the gender of the worker they are engaging with
- Arrange access to an accredited interpreter if needed (level three if possible) or an Auslan interpreter for people who are deaf or hard of hearing. For some communities with smaller populations, it is more likely an interpreter may know the victim or perpetrator. You can avoid identifying names or use an interstate interpreter. Offer an interpreter of the same gender as them. Children, family members and non-professional interpreters should not be used
- Ensure access to any necessary communication adjustments or aids if the person has a disability affecting their communication or other communication barriers, and confirm that they understand the information provided to them (see Practice Tip, below)
- Individually acknowledge the experiences of children and young people who may be victim survivors, particularly if they are present. If developmentally and age appropriate, provide the opportunity for them to raise any concerns of their own. Introduce yourself and explain that you need to speak with their parent/carer in private. Provide an appropriate and safe place to wait, and give them permission to come back into the room if they need anything
- You can assess risk directly with children if it is safe, appropriate and reasonable to do so. If you are doing so, consider if a parent/carer who is not using violence, or another safe person, should be present. If a parent/carer is present, be aware this may affect the responses the child or young person provides. Ensure that questions you ask are appropriate for that child or young person’s developmental age and stage (discussed further below)
- Let the person know that they can take a break at any time, and schedule breaks as required, especially if the person is distressed, ill or has a cognitive impairment or other relevant disability and remind them of this at appropriate intervals
- Ask the person if they would like to have an advocate or support person present (see Section 1.7). Do not assume this if another person attended with the victim survivor. Check that the advocate/ support person is not using violence or is close to the suspected perpetrator. Where possible, ask the question in private.
Practice tip
If the adult, child or young person has a disability or developmental delay that affects their communication or cognition, seek their advice or the advice of a relevant professional regarding what adjustments might assist (including any augmented or alternative communication support, such as equipment or communication aids).
If the victim survivor has an existing augmentation or alternative communication support plan in place, you should engage directly with them, with support from a support worker, advocate or other communication expert, if required, to help you navigate its use.
In cases where a child’s carer or primary caregiver is not a perpetrator or suspected/ alleged perpetrator, you can consult with them.
Where there is an existing relationship between the victim survivor and an advocate or support person, consider this relationship before agreeing to the inclusion of the other professional.
If the person suspected of using violence is a person who usually provides communication support, arrange alternative communication or support assistance to enable the victim survivor to take part in a safe conversation1.
Communicating about a perpetrator’s use of violence
Where family violence is identified or suspected, effective communication also includes placing responsibility for the violence and its impacts with the perpetrator. If an adolescent is using violence, placing responsibility should also occur with an understanding of their age, developmental stage, individual circumstances and family context. For example, any developmental delay or their own experience of family violence. This includes in situations where an adolescent is using family violence toward a parent/ carer, sibling, other family member or intimate partner.
Perpetrators often lead victim survivors to believe that the victim survivor caused or provoked the violence because they did not do something ‘right’. Perpetrators use this narrative to excuse their violence. It is important to keep the focus on the perpetrator’s responsibility for the violence, even if the victim survivor blames themselves.
1.3.4 Cultural safety and respect (using intersectional analysis in practice)
Reflect on information provided in the Foundation Knowledge Guide and the MARAM Framework on using an intersectional lens. The Foundation Knowledge Guide also includes more information on recognising personal bias and understanding the experience, structural inequality and barriers experienced by Aboriginal people and people from diverse communities or at-risk age groups.
Cultural safety is about creating and maintaining an environment where all people are treated in a culturally safe and respectful manner2. All people have a right to receive a culturally safe and respectful service, including:
-
Where there is no challenge or denial of a person’s identity and experience
-
Showingrespect,listening,learning,and carrying out practice in collaboration, with regard for another’s culture whilst being mindful of one’s own potential biases
-
Undertaking genuine and ongoing professional self-reflection about your own biases and assumptions including with more experienced professionals
-
Listening and understanding without judgement.
Other practical steps you can take include:
-
Be familiar with and know the requirements of your organisation’s client access and equity policies and procedures
-
Ensure a welcoming environment with inclusive signage and posters — for example, an Aboriginal flag, rainbow flag or transgender and gender diverse flag
-
Prior to meeting the person, ensure you know their name, including those of any accompanying children. Identify and review notes if available
-
Identify and challenge your own biases (see Foundation Knowledge Guide Section 9.7).
Providing a culturally safe response, particularly for Aboriginal people, includes respecting an individual’s right to self- determination. Consistent with a person- centred approach (described in detail in Foundation Knowledge Guide at Section 9.3), cultural safety includes recognising a victim survivor as the expert in their own experience and including and supporting them to make decisions about their own risk management.
Providing a culturally safe response also involves understanding how family violence is defined in different communities, including for Aboriginal communities. Further information is outlined in the MARAM Framework and Foundation Knowledge Guide at Section 10.4. Assessment processes must be respectful and inclusive of broad definitions of family and culture. For example, it is particularly important not to assume who is ‘family’ or ‘community’ to a child or young person, but rather to ask who should be involved in risk assessment and management.
1.4 Asking about identity
Always enquire about and record the language, culture and other aspects of identity of each family member.
Never assume you know these, or that they will be the same for each family member. It is good practice to openly acknowledge the culture a person identifies with in a positive and welcoming way. This includes, for example, ensuring Aboriginal children or young people that may be in the family are identified, even when accompanied by a non-Aboriginal parent/carer. Information about a person’s identity must inform all subsequent assessment and management responses.
Until you have built trust and rapport, some people may choose not to disclose their identity groups. This might be for a range of reasons, including fear of discrimination based on past experience.
For Aboriginal people, structural inequality, discrimination, the effects of colonisation and dispossession, and past and present policies and practices, have resulted in a deep mistrust of people who offer services based on concepts of protection or best interest. Professionals should be mindful of how this might affect a person’s actions, perceptions and engagement with the service. Acknowledge the impact these experiences may have had on a person, their family or community. Assure the person that you will work with and be guided by them to provide an inclusive service and minimise future discriminatory impacts through their engagement with your service.
It is also important to recognise the strength and resilience of Aboriginal people and culture in the face of these barriers and structural inequalities. Kinship systems and connection to spiritual traditions, ancestry and country are all important strengths and protective factors. The role of family is critical and Aboriginal children are more likely than non-Aboriginal children to be supported by an extended, often close family. Assessment of Aboriginal children must support cultural safety and take into account the risk of loss of culture.
You can find more information about cultural safety, including for Aboriginal children, and Aboriginal identity and experience in the Foundation Knowledge Guide at Section 10.4.
Why do some victim survivors not report family violence?
Victim survivors, predominantly women and children, might not report their experience of family violence or it might be reported in a way that obscures its nature or extent. For example, by reporting an injury, but not attributing it to violence (sometimes called ‘hidden reporting’).
Many varied and complex factors lie beneath hidden reporting and under-reporting, including shame, fear and stigma. Victim survivors may not recognise certain behaviours — particularly emotional or economic abuse — as constituting family violence.
Many women might not disclose or might minimise the extent of violence in an effort to manage the perpetrator. For example, a woman might fear that if she discloses the violence, the risk to herself or her children will escalate.
In the case of adolescent family violence, parents/caregivers may feel stigma and shame arising from unfair assumptions about the victim’s ability (often the mother) to be a good parent and the shock that their child (or grandchild or sibling) has used violence against them. Shame is exacerbated by lack of community awareness about this form of violence. Parents/carers might also fear their child may get a criminal record if the violence is reported to police.
Women may find sexual violence particularly difficult to disclose. The Royal Commission into Family Violence reiterated that sexual abuse is often ‘left under the table’ because of the additional layers of shame.
Responsibility 2, Section 2.6 describes a range of reasons a person may be reluctant to disclose family violence, and how you can address barriers to disclosure.
People who have diverse individual and/or social identities, circumstances or attributes, may or may not choose to disclose that to a professional unless they trust the professional and feel a rapport. You can support disclosure by never assuming how the person and their partner or parents identify. For example:
-
Don’t assume gender identity (which can result in misgendering) based on a person’s voice, appearance or how they dress as this can lead to disengagement
-
You can ask what pronouns a person uses by saying “I use [she and her / he and him / they and them] pronouns, what do you use?” This can let the person know you can provide inclusive and respectful service
-
You can ask if a person identifies as LGBTIQ and if there is a way you can support them to engage with your service, or if there are external supports available to ensure they are comfortable engaging with you
-
You can ask if the person has any disabilities, developmental delays or mental health issues, and if there are any supports or adjustments you need to make.
Services should be aware that identity is complex and that aspects of a person’s identity should be considered as part of their whole experience. To help inform your response, you might choose to engage in secondary consultation with specialist family violence services with an expert knowledge of a particular diverse community, and the responses required to address the unique needs and barriers faced by this group (see Responsibilities 5 and 6).
1.5 Building rapport and trust
From the first moment of engagement, victim survivors will be making decisions about how much information to disclose.
Building rapport with victim survivors is crucial as people are more likely to disclose the full extent of the violence if they feel they will be believed, not judged and provided with support.
When strong rapport and engagement have been established, victim survivors are more likely to discuss their experience, including the circumstances, relationships, impacts of violence and their self-assessment of their own fear, risk and safety.
Professionals will often have built rapport before family violence has been identified or disclosed. For this reason, people will often choose to disclose to a person in a service that they have existing rapport with. It is critical that all professionals are able to provide an appropriate response that preserves rapport and facilitates continued engagement and referral.
Building rapport and trust to support engagement is the responsibility of all professionals. Key elements of rapport building include:
- Fully explaining your role and responsibility within an organisation and introducing the risk screening or assessment process (as applicable) in a sensitive way. This should include an outline of the assessment process
- State that screening and assessing risk, as applicable, is a regular part of your service/organisation’s engagement. State that risk is dynamic and can change over time, so this conversation is undertaken regularly to understand if risk has changed or escalated. It is important to specifically address safety on each occasion. For example, to remind the person to call 000 in an emergency and that 24-hour services are available to support them
- Provide adequate information so the person can make informed choices. This includes providing information about information sharing laws which allow for the sharing of relevant information without consent in specific circumstances, discussed further in Responsibility 6
- Provide advice on your legal obligations as a professional, as applicable
- Ask open-ended questions about wellbeing to start the conversation.This might include questions about the person’s circumstances, identity and their relationship (including positive aspects) before moving to more specific and detailed questions about any family violence they may be experiencing
- Acknowledge the courage it has taken for the person to talk about their experiences with you and that you recognise them as the expert in their own experiences, circumstances and the violence they may have endured
- Continue to affirm to the person that they and their children (if applicable) have a right to live free from violence and that there are services and options, including legal options, to support their safety
- Be aware of how the person has expressed their identity or situation (for example, do they identify as Aboriginal, identify with a particular communityor faith groups, or as a person with a disability). Understanding a person’s identity can help you understand how their experience of family violence relates to other experiences of structural inequality, barriers to service access or discrimination, and its particular impacts on them (see Foundation Knowledge Guide Section 9.4)
- Highlight that any possible interventions will be guided by the person’s views and wishes
- However,safetyforthemselvesandany children that may be experiencing violence will be prioritised. Remember that when any victim survivor’s safety (adultor child) is in competition with an adult’s choices, safety is the paramount concern
- Be transparent around how information they disclose may be shared with other professionals or services, including Child Protection
- Tailor your communication, be flexible and not overly prescriptive in how you ask questions. This can include allowing people to tell their story as a way of gathering relevant information. Hearing a person’s story, guided by your questions and a conversational style can help to draw out information without seeming like an interview.
1.6 Trauma-informed practice in a person-centred approach
Refer to the Foundation Knowledge Guide on information about intersectionality, trauma-informed and person-centred practice. By combining intersectionality and trauma- informed practice into a person-centred approach, it will make it possible for a victim survivor to be validated and aware of the ongoing impacts of their experiences, and how you can tailor your responses to empower them to make informed choices and access services and supports.
You may be engaging with a victim survivor who you know has experienced trauma, from family violence and/or another cause. You can seek secondary consultation or seek shared support from a professional with trauma-informed practice expertise, such as specialist family violence service, to assist you. Their expertise may support you in engagement, and also assist you in a fuller consideration of family violence risk, experiences and management strategies.
Some of these professionals may also have expertise in, for example, art or music therapy, which may support your engagement and give you access to the information you need in a different way. This may be of use in engaging with someone with limited verbal capability.
1.7 Using an advocate or support person
You should ask the victim survivor if they need or would like a support person in the initial engagement process and revisit this during the assessment or management stages as required. The advocate/support person could be a trusted friend or family member who is not a perpetrator (such as a parent/ carer), or a relevant professional, as appropriate.
A support person should be appropriate and safe. There must be no coercion or control from the advocate/support person towards the victim survivor. A perpetrator may use their presence to intimidate or coerce a victim survivor, controlling the information they share as well as behaviour, such as by answering questions on their behalf or reducing the victim survivor’s access to interventions to support their safety.
You should have a private conversation with the victim survivor prior to an assessment, to explore their relationship to their identified advocate/support person. You should ask if the victim survivor feels comfortable with their advocate/support person knowing intimate and personal details about their life, or whether their presence will limit or change what a victim survivor will say.
If an advocate or support person is a new partner, be aware that a victim survivor may defer to a new partner or edit their story in their presence. A victim survivor may seek or need you to deny the support person access if they do not feel comfortable challenging their presence.
If a victim survivor has a cognitive impairment or requires communication adjustments, it is important to work on the assumption that the person has capacity and to overcome any communication barriers. Talking with the person directly rather than through their nominated advocate, support person or carer will assist to build trust and rapport and support disclosure. If required, you can consult with the Office of the Public Advocate for further advice.
1.8 Different factors that impact support and safety options
There are many different factors that might affect a victim survivor’s access to support and safety options.
These factors may also impact on the approach you take to create safe engagement. You should be familiar with how discrimination, structural inequality and barriers have affected Aboriginal people and people who identify as belonging to a diverse community or people from at-risk age cohorts (see Foundation Knowledge Guide Section 9.4).
People may have experienced racism, sexism, ableism, ageism, homophobia or transphobia, or judgement about their personal traits or circumstances. As a professional, it is important for you to acknowledge the influence of both your own culture and values, your biases, and those of the broader service system. Recognising these can enable you to challenge and address them and help you build awareness of your own place in the service system’s creation of structural privilege and power.
You should demonstrate an open and respectful approach to cultural and experiential differences. Consider how your engagement approach, as well as assessment and management practice can be tailored to reduce or remove barriers to engagement for people who face structural inequality and discrimination. Inclusive practice can be informed by asking the person, “What can I do to support you in our service?”.
You can find detailed information about how these different factors intersect, recognising structural inequality and discrimination, and engaging in person- centre reflective practice in the Foundation Knowledge Guide.
1.9 Responding when you suspect a service user is using family violence
As a professional, from time to time you will come into contact with people, including adolescents, who you suspect may be using family violence.
Use of family violence may be indicated from the person’s words or actions, or through another source of information.
A perpetrator or adolescent using family violence may use tactics to try and align you to their position to justify, minimise or excuse their use of violence or coercive behaviour, or to present themselves as a victim survivor. This is known as collusion and these behaviours are outlined in the Foundation Knowledge Guide at Section 11.
Identifying who is perpetrating family violence can be complex. Guidance on understanding misidentification of victim survivors and perpetrators, and identifying predominant aggressors is outlined in the Foundation Knowledge Guide at Section 11.3 as well as in Responsibilities 3 and 7.
You should not engage with a person directly about family violence if you suspect they are perpetrating family violence, unless you are trained or required to do so to deliver your service. This is because confrontation and intervention may increase risk for the victim survivor.
Instead, you should consider proactively sharing information, as authorised, with a specialist family violence service that can support the person you suspect is experiencing family violence (see Responsibility 5 and 6). You can also contact a specialist family violence service with expertise in assessing perpetrator risk and who can safely communicate with a person who may be using violence to engage them with appropriate interventions and services, such as behaviour change programs.
The age and developmental stage of adolescents who may be using violence, their circumstances, experience of trauma, emotional state, mental health and other contexts will inform the assessment or management response. Therapeutic responses, including those that involve other family members, particularly the non-violent parent/carers should be considered (see Responsibility 3). Some responses to adolescents (for example, those who have experienced trauma or have a developmental disability) will include behaviour modification and a skills-based approach.
A trauma-informed and developmentally appropriate approach to engaging with an adolescent who uses family violence may be used if their behaviour stems from trauma and learned violent behaviours from their parent/carer, or they are using intimate partner violence (noting that sometimes a young person may be using violence in both family and intimate partner contexts).
Further information about responding to adolescent family violence is in Responsibility 7 and in the Foundation Knowledge Guide at Section 11.2.
Respectful, sensitive and safe engagement - children and young people
Note: The prevalence of family violence against women and children, and against women as mothers and carers, is well established and recognised across the service system. Recognising this, the following section on risk to children uses gendered language to describe experiences for mothers, including damage to the mother/child bond caused by perpetrator behaviours. However, it should be noted that this guidance also applies to all forms of families and parenting.
Language in this section of ‘mother/carer’ refers to a parent/carer who is not using violence (a perpetrator).
1.10 Experience and engagement
How information in each of the preceding sections (Sections 1.1–1.9) applies to children and young people should also be considered.
A child is defined as a person under the age of 18 and a young person is aged 12–25 years. The guidance below is relevant for children and young people up to the age of 18. You should determine, using your professional judgement, if a young person who is approaching adulthood should be engaged using adult-centred guidance, as detailed above.
It is important to view and acknowledge children and young people as victim survivors in their own right:
- The risks to children and young people can be different to those of an adult victim survivor and may be different for each child or young person.
- Children and young people may be victim survivors of family violence whether they are targeted or not, or directly exposed or not, even if they do not hear or see it. Children who are exposed to family violence or its impacts are more at risk of direct family violence, including physical or sexual abuse.
- Children who experience family violence from an adolescent, such as an adolescent sibling, may be impacted in the same ways as children who are impacted by family violence from an adult. This includes being at risk of physical or sexual abuse.
- Professionals should recognise the experience of violence on a child or young person, including trauma and cumulative harm which can disrupt children’s achievement of development.
- Family violence can create significant risks to a child or young person’s social, emotional, psychological and physical health and wellbeing. Impacts on children who live with family violence may be acute and chronic, immediate and cumulative, direct and indirect, seen and unseen.
- Professionals should provide opportunities for children and young people to raise any views, wishes and concerns they have, and contribute to risk assessment, management and safety planning.
Recognising the signs of family violence or its impacts can be difficult. It is important to remain aware of and balance your own biases and ensure you are being non-judgemental when considering the experiences, wellbeing and safety of children and young people. For example:
- Parents/carers are expected to set boundaries that are appropriate to age and developmental stage for children and young people and these vary across and within all cultural and faith groups, as do approaches to teaching and discipline.
- Male and female children/young people, and children who are non-biological children of one or both parents, may be treated differently within families and according to family, cultural and other gendered norms.
In addition to barriers to service access arising from discrimination and structural inequality related to identity (as outlined in the Foundation Knowledge Guide) children and young people may experience additional barriers due to their age and developmental stage. This includes, generally, requiring consent to engage with services from a parent/carer. You should note that consent is not required to assess or manage family violence risk or promote wellbeing or safety of children and young people.
Each child or young person experiences family violence differently, and in particular forms of violence, to other family members depending on their age, stage of development, identity, their relationship to the perpetrator, and their level of dependence on adult carers. For example, as outlined in the MARAM Framework:
- Aboriginal children experience higher rates of family violence, including from non-Aboriginal family members.
- Girls with disabilities are twice as likely to experience family violence.
- Young people from LGBTIQ communities may experience forms of violence relating to ‘coming out’, their gender identity, and rejection from their families, and are over-represented in homelessness populations.
Children and young people engaged in universal services, such as early years services or education, are likely to have their initial risk identified without a parent/carer present:
- This should only occur if it is safe, appropriate and reasonable to do so.
- In some cases, professionals should seek the input of a parent/carer who is not using violence for further risk assessment.
- Where risk is present for children and young people, the parent/carer should also have their risk assessed.
Young people can be affected by family violence in their own intimate relationships, such as their ‘dating relationships’. Although young women experience family violence at higher rates than their older counterparts, they can also be reluctant or unable to identify the behaviour as coercive or abusive.
Young women experiencing family violence are more likely to disclose or seek help from a peer, and peers are also more likely to know about violence or coercion within a relationship. Therefore, disclosures may not be made directly from the young person experiencing the violence to a professional or service. In such cases, support also needs to be provided to peers who have received a disclosure from a friend.
Many adolescents experiencing family violence are likely to enter the service system through youth support, youth justice or homelessness services.
Adolescents who may be using family violence, may be currently experiencing or may have experienced family violence, sexual assault or abuse in the past. Some adolescents may use violence due to difficulty with emotional regulation or heightened emotional states. This can be further exacerbated by substance use, particularly substances like methamphetamine. Any responses to adolescents should be underpinned by an understanding of the context in which the use of violence occurs, and therapeutic responses and/or behaviour modification strategies should also be explored (see Responsibilities 3 and 7).
1.10.1 How can you support assessment of a child or young person’s risk?
Children and young people, like adult victim survivors, hold information about their own experience of risk. Child victim survivors should be supported through direct engagement where appropriate, safe and reasonable to do so. Engaging directly with children and young people can help them to feel safe.
Most older children and young people can understand and articulate their experiences of violence and coercive control, and this experience differs from those of adults.
While acknowledging children’s unique and individual needs, many children may prefer to be spoken to with the support of their parent/carer who is not using violence, or other significant person/carer. If age and stage appropriate they should have the opportunity to speak privately if they wish to do so.
There are a range of options for assessing a child or young person’s risk. This may occur by:
- Asking questions directly if appropriate, safe and reasonable to do so (reflecting their age, developmental stage and individual circumstances).
- Asking questions of the parent/carer who is not a perpetrator (usually a mother, who may also be a victim survivor).
- Asking questions of another appropriate adult or professional engaged with the child.
You should consider each option as to whether it is safe, appropriate or reasonable. Further guidance on determining the appropriate approach to assessing risk for children and young people is in Responsibility 3.
Each option requires you to ensure you have built rapport with any supporting, non-violent parent/carers and the child or young person.
1.11 Building rapport with parent/carer to support assessment of a child or young person
Remember
Victim survivors who are parents/carers (usually mothers) may prioritise immediate action that minimises harm to themselves and their children. It should be acknowledged that victim survivors who seek assistance and intervention are acting in the best interests of the child or young person.
Mothers who may also be victim survivors are often a key source of information and expert in assessing risk to self and their children. However, in some situations, their ability may be restricted in providing for their child’s needs due to the actions of the perpetrator. Due to their own experience of violence from a perpetrator, their assessment of risk and impact of the violence on their children should be balanced with an independent assessment of the child or young person’s risk. Parents/carers may require information and support to understand the assessment of risk for their children.
A perpetrator’s actions and behaviours may be specifically directed to undermine a child’s relationship with their parent/carer (usually the mother). Children who witness or experience family violence directly, or are exposed to its impacts, may not recognise protective behaviours from a parent/ carer who is not a perpetrator, or might be accustomed to hiding or tolerating the violence.
Mothers might need assistance to help their children make sense of their negative experiences within the family home. It is important to recognise that parents/ carers often go to significant lengths to try to minimise or prevent the perpetrator’s violence from impacting his children. Sometimes these actions have their own impact on the child’s safety, and on their relationship with their mother.
Perpetrators often use family violence to attack or undermine the child’s bond with an adult victim survivor/other parent/ carer (described in detail in the Foundation Knowledge Guide at Section 10.2) It is important to create a safe environment to explore risk that is being experienced by children, including through talking and building rapport with a parent/carer (who is not a perpetrator) and may be a victim survivor. Approaches to do this include:
- Asking the parent/carer rapport-building questions about the children in the family. For example, “tell me about your children”. It is important to establish early on the level of risk that a child is experiencing, and this should be considered independently to any risk being experienced by their parent/carer
- Assessing the risk of adult victim survivors without children present. Arrangements should be made for appropriate professionals, or another safe person, to care for the children during this time.
- Asking specific questions about what risk the perpetrator poses to the children (such as through screening or assessment, see Responsibilities 3 and 7), and how the violence is impacting the children. This should be done whether or not the violence is being experienced by direct actions towards a child or indirectly through exposure to violence or its impacts. Affirm the experience and impact of indirect violence on a child.
If you can’t assess children directly, you can build rapport and trust with the parent/ carer through their assessment to help you do so in the future. This will help to reduce the fear, shame and self-blame that a parent/carer may feel if their child has experienced family violence. A good rapport can also support direct discussion if the parent/carer has fears about possible engagement with Child Protection, and is unsure how they can be supported in this process. This is particularly important when working with adults, children or young people who identify as Aboriginal, belonging to a diverse community group and older people who may have experienced discrimination, impacts of child removal or other structural inequality and barriers which have created mistrust in services (see also the Foundation Knowledge Guide).
1.12 Building rapport to engage directly with children and young people
If you are trained and resourced, or your role is to engage with children and young people, you can do so for the purposes of assessing risk. If not, consider engaging or seeking secondary consultation with services that specialise in working with children and providing therapeutic interventions. Consider:
-
If a child is old enough to speak with you, talk to them about your role as appropriate to their age and developmental stage. For example, you might say to a very young child “I am here to help you and mummy.” You should tailor your use of language and style to meet the needs of the child or young person.
-
If a child or young person has experienced trauma, ensure your practice does not further traumatise them. As described above, consider seeking secondary consultation or support from appropriate professionals or services (see Responsibility 5 and 6).
-
The older and more developmentally advanced a young person is, the more information you can/should be able to provide. If a young person is nearer in age to adulthood (18 years), you can consider if it is age and developmentally appropriate to use the adult risk assessment tools, discussed further in Responsibility 3.
-
Your assessment will be more accurate and complete if children and young people have direct input. For example, you might note the presence of a range of potentially supportive adults in a child’s life. However, the child/young person themselves is best placed to tell you about whether they see these people as supportive and trusted, and the degree to which they feel trust in them.
-
If assessing a child/young person directly, building rapport will need to be centred on them, as much as the parent/carer who may be experiencing violence, if they are also present. The focus of the assessment will change from one centred on the adult to one centred around the child/young person, and the impact of violence on the carer/ parent-child relationship, as applicable. Remember a child victim survivor may have an enduring relationship with the perpetrator. For example, if this person is a parent. Obtaining the child’s views and wishes regarding both of the parents is necessary to meet the child’s wellbeing and developmental needs.
-
Where assessing risk directly with a child/young person, without a parent/ carer present, another appropriate professional should be engaged as an independent third person to support the child/young person.
1.12.1 Safe engagement with infants
Play-based support: If a victim survivor is very young, or has limited verbal communication, you may wish to seek support in understanding their play-related behaviour. Their behaviour can reveal a significant amount about what a child or young person is navigating. A professional with training in engaging with infants, such as a maternal child health nurse, behaviour specialist, early childhood teacher (who may be employed in early learning centres), or early primary teacher may be able to assist you in this engagement and consideration of their behaviours. Where they have an existing relationship with the victim survivor, they may be able to assist with contextualising behaviours, and/or providing further information about their play beyond your engagement.
Infants usually communicate a great deal about themselves through their play. When you communicate with an infant:
-
Observe closely to see their reactions and modulate your approach accordingly.
-
Look for any signs of physical violence, such as bruising or abrasions.
-
Remember that sudden moves and loud voices may be re-traumatising for infants, even if they are intended to be fun and engaging.
-
Where possible, sit at the child’s level (often this means on the floor) and play alongside them.
-
Remember that infants understand more than they can express verbally — talk about what you are doing as you are doing it.
-
Acknowledge what the child seems to be feeling, consciously modelling ways to validate both the emotions that the child has, and their expression of them.
Remember, eye contact is desirable in many cultures but not all. In the latter case, even young infants will have absorbed their parents’ cultural practices in this regard. In addition, infants generally look away if they feel overwhelmed.
1.12.2 Safe engagement for children and young people
Engagement with children and young people should be based on their age and developmental stage. You should consider whether the information needs to come from direct communication with the child/ young person, or if it could be obtained from other sources, including any appropriate adult who is not suspected of using family violence.
For many professionals, the conversation with a child or young person about whether they are experiencing family violence will take place in an organisational environment such as an office or clinical setting. Children and young people are more likely to engage with you at your office if the space is welcoming and inclusive.
However, if your workspace is not a safe environment or is not optimal for the child/young person’s needs, you should consider appropriate alternatives. This may include the child/young person’s home, or a playground, park or cafe. Settings that have movement, require limited eye contact, and there is something neutral to look at can make it easier for children and young people to communicate. For example, children and young people may prefer to talk with you whilst being driven somewhere or while playing, driving or walking.
Young people might have different views, needs and wants to their parent/carer, and you might feel a tension in supporting both parties. If your agency does not have a youth worker, consider asking a youth service to support and advocate for a young person.
1.12.3 Activities
Children and young people also tend to engage through age-appropriate play. Children and young people might struggle to find words to describe their experiences and label their feelings. Consider using age-appropriate communication aids such as drawing, dolls, puppets, or feelings/ strengths cards. It is preferable to seek advice or training on how to incorporate these into your practice.
Children and young people with communication barriers or are non-verbal, may also benefit from this form of engagement.
1.13 What's next?
Guidance on identifying and screening for family violence risk is outlined in Responsibility 2. All professionals who suspect that a person is experiencing family violence should use the guidance in the next chapter on how to identify the presence of family violence, including the use of the Screening and Identification Tool.
1. Organisations such as Scope and Communication Rights Australia may be able to assist.
2. Adapted from State of Victoria, 2018, Dhelk Dja: Safe Our Way, Cultural safety, page 31.
Responsibility 2: Identification of family violence risk
Responsibility 2 chapter of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
Appendix 1 contains the observable signs of trauma that may indicate family violence. The document includes separate lists for adults, children and young people (Tables 1-5).
Appendix 2 contains the Screening and Identification Tool within a table of practice guidance.
Appendix 3 contains the Screening and Identification Tool as a standalone template.
Appendix 4 contains a flow diagram of response options and a basic safety plan.
2. Identification of family violence risk
2.1 Overview
This chapter should be used when family violence is suspected but not yet confirmed.
This guidance will enable you to identify if family violence is present and undertake screening for an adult, child or young person to assist you to decide if further action and/or assessment is required. Specific guidance on identifying violence and use of screening tools with children and young people is outlined in Section 2.7 of this guide.
Only professionals who have received training to engage with perpetrators about their use of violence should do so. It can increase risk to a victim survivor to engage with a perpetrator when not done safely.
Key capabilities
All professionals should have knowledge of Responsibility 2, which includes:
- Awareness of the evidence-based family violence risk factors and explanations, outlined in the Foundation Knowledge Guide
- Being familiar with the questions to identify family violence, observable signs and indicators, using the Screening and Identification Tool and how-to-ask identification questions
- Using information gathered through engagement with service users and other providers via information sharing to identify signs and indicators of family violence (for adults, children and young people) and potentially identifying victim survivors. Information sharing laws and practice is further described in Responsibility 6.
Remember
Guidance which refers to a perpetrator in this guide is relevant if an adolescent is using family violence for the purposes of risk assessment with a victim survivor about their experience and the impact of violence. Risk assessment and management for adolescents should always consider their age, developmental stage and individual circumstances, and include therapeutic responses, as required.
2.1.1 Who should use the Screening and Identification Tool?
Appendix 2 contains the Screening and Identification Tool within a table of practice guidance. The Screening and Identification Tool as a standalone template is in Appendix 3.
All professionals should use the Screening and Identification Tool, either applied routinely when this is a part of your professional role or service, or only when indicators of family violence are identified.
Screening is not an activity that occurs only once by a single professional or within a service. In service settings where a person has multiple contacts, it is necessary to screen over time and at each contact to ensure any changes in the relationship or use of violence is identified.
Some organisations and workforces will undertake routine screening, asking every person accessing their service questions to screen for family violence (such as in perinatal settings or Youth Justice). Other workforces will only use the Screening and Identification Tool when they have identified indicators or signs of family violence risk through their regular service and are seeking to confirm the presence of family violence.
Identification (including through use of the Screening and Identification Tool) will support professionals to form their professional judgement about how to respond.
2.2 Structure professional judgement in identification and screening
Reflect on the model of Structured Professional Judgement outlined in Section 9.1 of the Foundation Knowledge Guide.
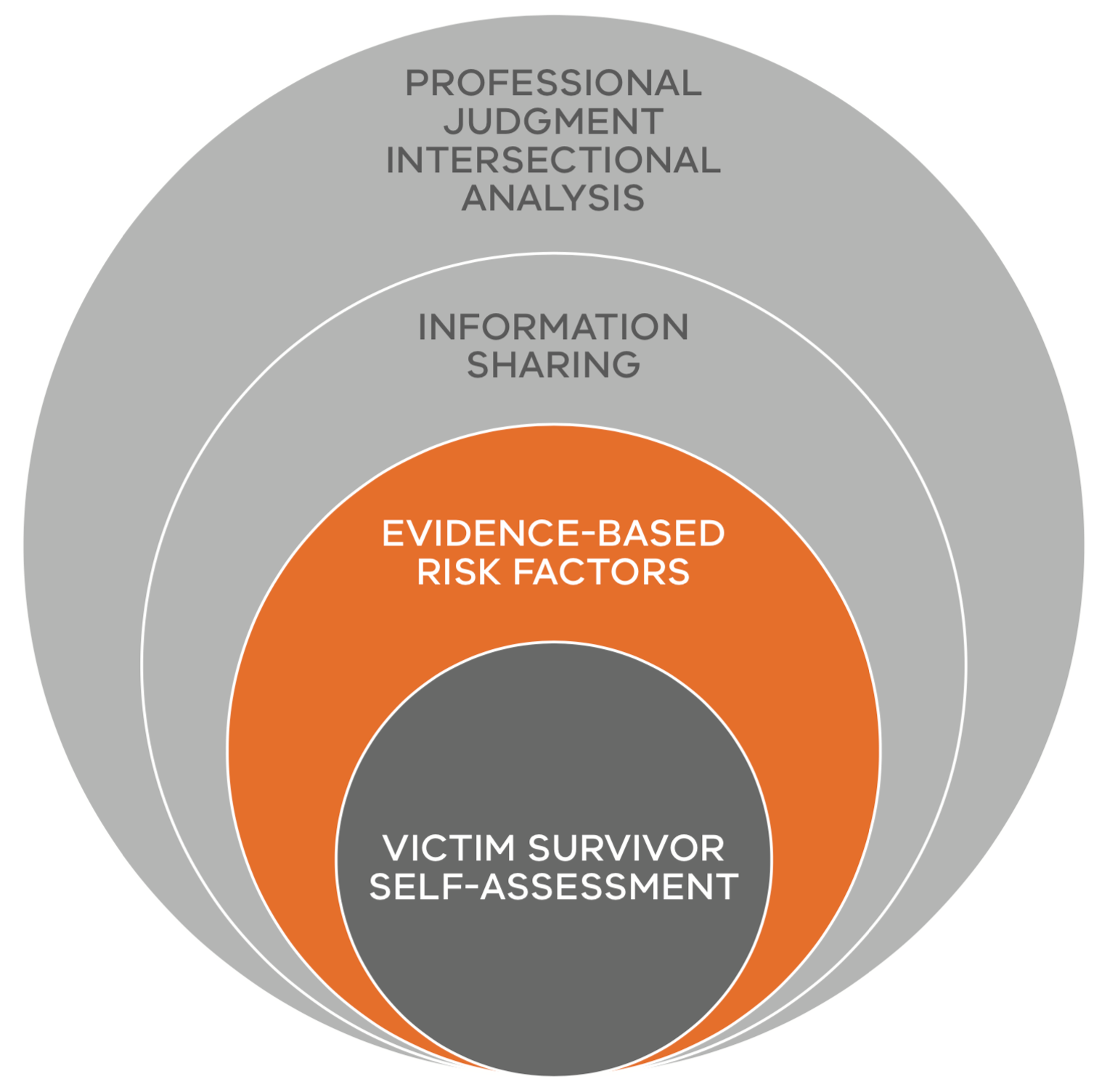
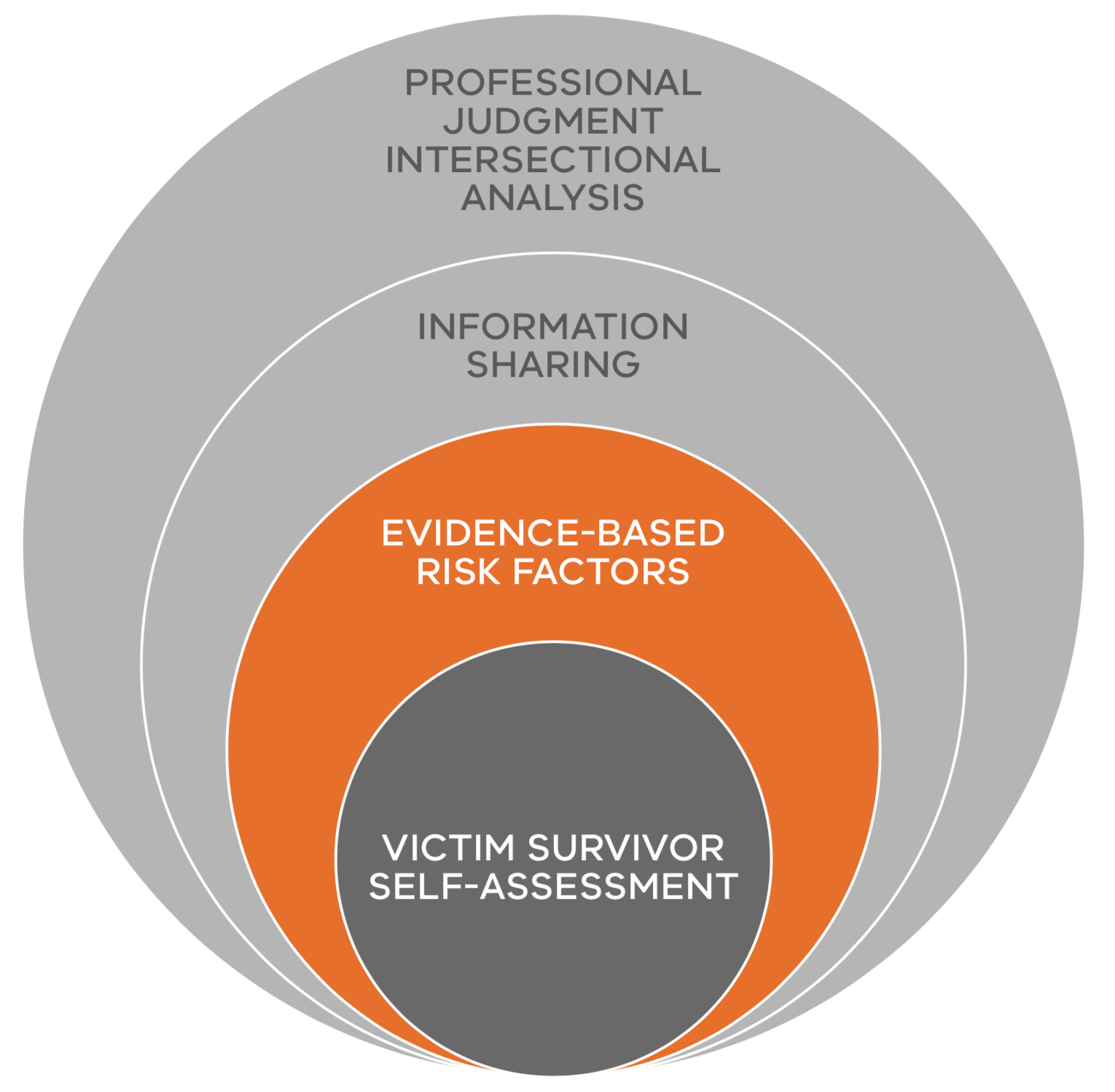
Identification and screening is the first opportunity to ask a victim survivor about their self-assessment of their risk, fear and safety, as well as some initial questions about family violence risk factors. These can be further informed by risk assessment and information sharing, described in later responsibility guides.
Figure 1: Model of Structured Professional Judgement
{kind=link}
Identification and screening is the first step in understanding if family violence risk factors are present, and is informed by a person’s assessment of their own level of family violence risk (self-assessment). Observing signs and indicators of risk and asking screening questions about family violence support these two elements of Structured Professional Judgement.
2.3 Identification of screening for family violence
Identifying and screening for family violence means identifying that family violence risk factors are present. This can be done through observation of signs of trauma that may ‘indicate’ family violence is occurring, and/or confirming this by undertaking screening.
Screening involves asking questions defined in a ‘tool’ (provided in Appendix 3) to enable a person to disclose whether they are experiencing family violence. The questions are designed to identify information about evidence-based family violence risk factors. The Screening and Identification Tool includes some of the high-risk factors associated with an increased likelihood of a person being killed or almost killed. All of the questions in the Screening and Identification Tool should be asked, when possible.
Before beginning, you should discuss the purpose of the Screening and Identification Tool (or risk assessment) with the person. You should acknowledge that some of the questions may be confronting and difficult to answer but that they are important for assessing risk and identifying appropriate responses.
2.3.1 What are family violence risk factors?
The family violence risk factors are outlined with a short description in the Foundation Knowledge Guide in Section 8. Family violence risk factors are evidence-based factors that are used to:
-
identify if a person is experiencing family violence
-
identify the level of risk, and
-
identify the likelihood of violence re-occurring.
Responsibility 3 describes how to assess for risk factors, including determining the level or seriousness of risk.
2.3.2 Observable signs of trauma that may indicate that family violence is occurring
Family violence risk factors may be identified through observing signs or ‘indicators’ related to a person’s physical or emotional presentation, behaviour or circumstances. These signs are presentations of possible trauma, which may indicate family violence is occurring and can be expressed differently across a person’s lifespan, from infancy, childhood and adolescence1, through to adulthood and old age.
Appendix 1, Tables 1–5, contain a non- exhaustive list of signs of trauma which may indicate that family violence is occurring for adults and children.
These signs of trauma do not by themselves determine that family violence is occurring, they are ‘indicators’ only at this stage. These signs may also indicate that another form of trauma has occurred. If you suspect someone is experiencing family violence, it is important to ask the person screening questions about family violence.
Adults and children experiencing family violence may also not exhibit any of these signs and indicators. If you don’t observe any signs or indicators but think that something is ‘not quite right’, you should use prompting questions or the Screening and Identification Tool to explore whether family violence might be occurring.
2.3.2.1 Signs and indicators relating to age for children and young people2
Signs of trauma in a child or young person may indicate family violence or another form of trauma. Signs may be observed through the presentation, behaviour or circumstances of a child or young person. Some signs may relate to trauma from specific forms of family violence, including sexual abuse (indicated by) or emotional abuse (indicated by *).
Some signs may indicate a child’s experience of trauma or other circumstances outside of the family or home environment. Consider the wellbeing and safety of a child within and outside of the family context when observing these indicators.
Children’s behaviours may be driven by a range of underlying factors, including disability, developmental issues, and non-family violence related trauma and you will need to consider how these factors may be affecting or reinforcing each other. Significant changes in behaviour can indicate the presence of family violence and/or increased risk.
Observable ‘general’ signs of trauma for a child or young person of any age are listed in Appendix 1, Table 2. Signs can also vary considerably according to the age and stage of a child or young person’s development, and are listed in Appendix 1, Tables 3 and 4.
Sometimes the presence of family violence may be observed from a child’s circumstances and may relate to neglect due to the experience of family violence. Some signs or indicators of neglect are listed in Appendix 1, Table 5.
Guidance on whether to assess children and young people directly, or through asking questions of a parent/carer who is not using violence, is outlined at Section 2.7.
2.4 Using prompting questions with an adult support screening
You can use broad, prompting questions that lead into screening questions to begin the conversation. You can use your judgement on how to use these example questions or other prompting questions appropriate to the individual or their circumstances.
You can begin by asking open-ended, rapport-building questions about their wellbeing, for example:
-
“I’m pleased to see you today — how are things going?” [if Aboriginal — “Can I ask who are your mob?”]
-
“What has brought you here today?”
-
“Can you tell me what has been happening for you lately?”
-
“Tell me a bit about your family/home life/relationship with X?"
You can also frame prompting questions as part of routine or formal process used in your service to identify and screen for family violence risk. You can have a scripted question, such as:
- “In our organisation it is common that we ask questions about family violence so we can connect people with appropriate support. Is it ok if I ask you a few questions about how things are going at home/in your relationship?”
- “When we are concerned about someone, we always ask a set of questions to find out if they are experiencing violence or being mistreated in any of their relationships”
- “You have just let me know X (i.e. that you have recently separated). When any of our clients tell us this we ask a question about your experience at home and safety”
- “Is there anyone else in the family who is experiencing, seeing, overhearing, or being exposed to or aware of these things?”
You can also start by linking some of the observable indicators (Appendix 1) into the conversation.
- “I noticed that you appear to be experiencing X, is there something worrying you/you would like to talk about?”
You could use simple statements such as:
-
“Many people experience problems in their relationships.”
-
“I have seen people with problems like yours who have been experiencing trouble at home.”3
If an adult, child or young person responds to your prompting questions, you can ask the direct screening questions in the Screening and Identification Tool. These are purposely direct, because research indicates that victim survivors are more likely to accurately answer direct questions.
2.5 When to use Screening and Identification Tool
The Screening and Identification Tool as a standalone template is at Appendix 3.
Guidance on each question in the tool is at Appendix 2.
It is important to note that the Screening and Identification Tool has been developed to be used with adult victim survivors to identify family violence for both adult and child victim survivors.
The purpose of the Screening and Identification Tool is to identify:
-
If family violence is occurring
-
The victim survivor’s level of fear for themselves or another person
-
The person using violence/perpetrator.
The outcome of the Screening and Identification Tool will guide you on what to do next, that is, whether immediate action, further assessment and/or risk management is required.
If someone isn’t ready to respond to your questions about family violence, you need to respect this and let them know that if they are ready in future to talk about any experience, you are open to doing this.
The Screening and Identification Tool should be used:
-
When you suspect that someone may be experiencing family violence and have observed signs/indicators of family violence
-
To start the conversation if someone discloses they are experiencing family violence
-
If your workplace requires you to screen all individuals you work with for family violence (that is, ‘routine screening’ such as in antenatal/maternal child health settings).
At times, a victim survivor may want to give detailed answers about their experiences. The priority in this identification and screening stage is to identify the presence of risk and any immediate risk. This may mean you need to refocus or guide them back to a question. You can say you want to give them space and time to share their experience. However, if risk is identified as present and it is the role of another professional within your service or another service to continue to undertake intermediate or comprehensive assessment, you can sensitively contain the conversation around screening to ensure they do not have to tell their story multiple times (which can increase trauma).
Screening and identification should not be undertaken if the person suspected of using violence is present.
Your objective is to encourage the person to tell their story in their own words. You could lead into the questions by describing how the questions are structured, with a statement such as:
-
“I would like to ask you a series of questions that have ‘yes’, ‘no’ or ‘don’t know’ answers. They will help us work out what to do next together”
-
“We will start with questions about the person making you feel unsafe or afraid and then ask some questions about your level of fear and questions about children (if relevant).”
It is important to ask direct questions about family violence. Questions 1–4 support you to understand if family violence risk is occurring, the victim survivor’s level of fear for themselves or another person and the identity of the person using violence (the perpetrator).
Risk factors may change over time and some may increase in severity. A perpetrator may change their behaviours and their impact on the victim survivor may become more severe. If a risk factor has increased in severity, recently or over time, this should be noted as indicating an escalation in violence and a serious risk.
Frequency by itself is not always the indicator of the level of risk you should be asking further questions to understand if frequency has changed or escalated. This is particularly important for some high-risk factors and provides important information when considering if someone is at immediate risk.
Some key considerations when asking screening questions 1–4 is to look out for information about changes in frequency or severity which may indicate escalation and imminence of risk, particularly if change or escalation has occurred recently (further explored in questions 5–7).
How to move through the risk assessment questions:
- If the answer to a question indicates that family violence is not occurring no action is required relating to that risk factor/ question. Advise the individual that if this occurs in future to seek assistance
- If the answer to a question indicates family violence is occurring, proceed to the next question(s) as outlined below.
Remember
Screening questions are designed to be asked to an adult victim survivor about their risk or risk to any children and/or young people. The risk for children and/or young people correlates to the level of risk for the adult.
Risk to children and young people should be identified independently and informed by risk identified as present for the adult victim survivor (for example, who may be a parent/ carer).
2.6 Why someone might not disclose family violence, even if asked
There are many reasons why people do not feel comfortable or ready to disclose family violence. For example, a person might:
- Not be ready.
- Not identify their experience as family violence.
- Have had negative experiences when disclosing it in the past.
- Be scared that the perpetrator will find out that they have talked to you and the potential repercussions for their safety.
- Be concerned about cultural profiling or not feeling culturally safe.
- Be concerned about their visa or residency status.
- Be worried that they don’t meet family or community expectations.
- Be worried that their primary carer will be taken away.
- Be worried that their children will be taken away.
- Be worried about judgement if they are in a same-sex relationship.
- Be worried about judgement if they are not ready to end their relationship.
- Be worried about judgement for their life circumstances or lifestyle choices.
- Be worried that a disclosure is interpreted as evidence of mental illness.
- Be worried about the perpetrator harming themselves or their children if they report family violence and/or end the relationship.
- Be concerned about the impact of disclosure on the family unit, a perpetrator or adolescent using family violence, such as on their development or involvement of justice responses.
- Be worried that professionals won’t believe them.
To address barriers to disclosure and provide a safe opportunity to disclose, you can take a partnership approach by explaining processes, active listening, normalising anxieties and fear of disclosure, and setting realistic expectations to strengthen your rapport and engagement.
Some issues identified above can be mitigated by reassuring the person (adult or child) how your service will not share their disclosure of family violence with the person who may be using violence. For example, if information is shared with other sources it can be conveyed as sensitive and should not be made known to the perpetrator.
If a perpetrator becomes aware information was shared, it should be presented as being based on other sources or reports rather than by the victim. For example, family violence safety notices or intervention orders which they would already be aware of.
2.7 Identification and screening for children and young people
Children and young people can be affected by family violence even if they do not hear or see it. Whilst there can be many causes of trauma, signs of trauma can be an indicator that the cause of that trauma is from family violence. If you observe one or more of the signs of trauma listed in Tables 2–4, Appendix 1, this may indicate that a child is experiencing direct family violence or being exposed to family violence and its impacts. Consider any observable signs of trauma with other information about the child’s circumstances.
If you see signs of trauma, this should prompt you to screen for family violence. For children and young people you can screen for family violence by asking:
- The child or young person prompting questions at Section 2.7.3 to provide you with more information about what may be causing the signs of trauma.
- A parent/carer who is not using violence questions in the Adult Screening and Identification Tool (Appendix 3) which includes questions about risk to children.
Making a decision on whether to screen directly with a child or young person, or through assessment with a parent/carer is outlined further in Responsibility 3, including considerations about whether it is safe, appropriate and reasonable to do so, with reflection of your professional role and experience or training in working directly with children or young people.
You should also consider assessing for wellbeing and general safety, guided by your organisation’s policies and procedures and any existing child wellbeing frameworks that apply to your role.
2.7.1 Speaking with adults about violence their child might be experiencing
You should always ask the parent/carer about what their child/ren might be experiencing directly or exposed to from a person who may be using violence (even if the person does not live with them). This includes if a child is being exposed to the aftermath of family violence (for example, broken furniture or an upset or injured victim survivor).
Explain to the parent/carer that they may be experiencing family violence and that it may be impacting their children. It is important for you to ask:
- “What are your worries for each of your children?”
- “What have you noticed about how this is affecting the children?”
Explain to the parent/carer:
- That you may speak to their child directly
- What kind of questions you will ask their child (even if they will be present)
- Why you need to ask the questions.
If the parent/carer is not present, ask the child or young person:
- To identify a parent/carer (who might also be a victim survivor) or safe person who is not using violence
- For their views about sharing information about what they have told you with that parent/carer.
Reassure both adult and/or child victim survivor(s) that they will not be identified as the source of any information to the perpetrator.
When asking these questions, you should be sensitive to the impacts of perpetration of family violence on women (and other caregivers, kin or guardians) as parents. Perpetrators often use various harmful tactics to deliberately undermine, manipulate and damage the mother-child relationship. This can cause women to lose confidence in their parenting and affect their ability to be as engaged with their children as they want to be. In this context, questions touching on parenting may be seen as intrusive and undermining.
You should be aware of these dynamics and tactics to avoid making judgments about women’s parenting when asking the questions above. See Section 10.2 of the Foundation Knowledge Guide for detail about the impacts of perpetrator behaviours on parenting.
2.7.2 Deciding when to talk with a child or young person directly
If you or another professional has expertise and training in working with children, and it is safe, appropriate and reasonable in the circumstances, you can speak with the child or young person directly about the signs you have observed. Assess all children and young people in ways that are appropriate to their stage of development:
- When talking to younger children it is useful to physically get down to their level, consider your tone of voice, and speak gently and reassuringly. You might start your conversation by acknowledging that they may be nervous or confused about speaking to an adult they don’t know, or don’t know very well. Reassure them that they will not be in trouble and you won’t judge them, no matter what they tell you
- In addition to above information, primary school-aged children can be asked the simple direct prompting questions suggested below
- For young people, a mix of the questions for adults and children might be suitable. Young people, especially young women, might experience violence in the family home and/or from a partner outside the home so it is important to obtain the name of the suspected perpetrator or adolescent who may be using violence and their relationship to the victim survivor.
Further information on assessing risk for children and young people can be found in the Assessing Children and Young People Experiencing Family Violence Practice Guide.
You can screen for family violence with children and young people by asking the prompting questions below.
2.7.3 Using prompting questions with children and young people
For children and young people, use prompting questions that may relate to observations you have made about their manner or situation. If you have identified signs or indicators of trauma, including those that may relate to neglect, you can start by asking questions based on things you have observed. For example:
- “You appear to be really tired today. Is there a reason you’re maybe not getting enough sleep?”
You can also ask general prompting questions about their home life or family relationships:
- “Have things changed at home recently?”
- “Tell me about the good things at home”
- “Is there someone at home that makes you feel safe?”
- “Can you talk to them if you had a problem or were worried about something?”
- (If the answer to the above question is no) “Are there other adults who make you feel safe that you might be able to talk to?”
- “Are there things at home you wish you could change?”
- “What don’t you like about home?”
- “Does anyone living in your home do things that make you feel unsafe or scared?”
- “Tell me about the ways mum/dad/family member or carer look after you?”
- “What happens in your house if people have a fight?”
- “Do you worry about your mum/dad/ brothers/sisters for any reason?”
When using these prompting questions, you should keep the following practice considerations in mind:
- Ask questions in an empathic, non-judgemental manner
- Remember to validate a child who provides you information or expresses their feelings about their family or circumstances
- Do not ask questions in a way that feels like a list
- Use language that is age and developmentally appropriate, as well as relevant to the culture and community that the child is part of. Some children and young people may not like the words ‘violence’ and ‘abuse’. Some cultures and communities have other words that they use with the same meaning
- It is important to use words that adults and children themselves use
- If a child is experiencing family violence their trust in adults may already be damaged.
2.8 Guidance on using the Screening and Identification Tool
Appendix 2 contains the Screening and Identification Tool questions, and relevant practice guidance information.
The Screening and Identification Tool as a standalone template is in Appendix 3.
It is important to note that the Screening and Identification Tool has been developed to be used with adult victim survivors to identify family violence for both adult and child victim survivors.
How to move through the risk assessment questions:
- If the answer to a question indicates that family violence is not occurring, no action is required relating to that risk factor/ question. Advise the individual that if this occurs in future to seek assistance.
- If the answer to a question indicates family violence is occurring, proceed to the next question(s), as outlined below.
2.9 If it seems family violence is not occuring
If responses to the screening questions indicate that no family violence is occurring, you must respect this. The person might not be ready or not feel comfortable talking to you about the family violence they are experiencing. They may also not be experiencing family violence.
Thank the person for answering the questions and inform them about the help that is available and that they are able to contact your service in future should they ever experience family violence.
2.10 If family violence is occuring
If the person’s responses indicate that they are experiencing family violence:
- Reassure the person that you believe them and state clearly that the violence is not their fault, and that all people have a right to be and feel safe.
- Acknowledge any challenges and difficulties they have spoken of and validate their efforts to protect themselves and their family members.
- Let them know that there are different services and options for people who experience family violence.
- Ask whether they would like your help.
- If Responsibilities 3 or 7 are a part of your role:
- Explain that you would like to ask them further questions to assess the level of risk and ask them if they are ok for you to proceed.
- If Responsibilities 3 or 7 are not a part of your role:
- Let the person know you would like to seek secondary consultation or refer them to a trusted professional who can undertake further assessment of the level or seriousness of risk (see Responsibilities 5 and 6). Let them know that this will enable you and the specialist professional to determine together what action may be required to support the person to be safe.
- You might need to contact several services or authorities in response to a disclosure of family violence for secondary consultation or to respond to immediate risk.
- Appendix 4 outlines a flow diagram of response options and provides a basic safety plan.
- If children are identified as experiencing family violence, let the person (adult) know that you may have responsibilities to assess or manage children’s wellbeing or safety, or under legislation to report any abuse to the relevant authorities.
2.11 If family violence is occurring and an immediate response is required
If family violence is identified and an immediate risk management response is required (that is, the person has let you know they are experiencing an immediate threat to their life, health, safety or welfare, or you have determined this based on their answers to screening questions):
- contact the police or ambulance by calling 000, or
- contact other emergency or crisis services for assistance
This may be indicated if the person does not feel safe to leave the service. For example, you could say “I am very concerned about your safety and would like to help you get assistance today. How do you feel about us contacting specialist assistance?”
You should ask the victim survivor about their views on calling the police or other emergency and crisis services. If there is an immediate threat, calling the police is an appropriate response, however, if the person indicates that calling police may increase their risk:
- Their experience and views should guide your approach as this can inform you about the level of immediate risk and management responses that may be needed.
- You should talk to them about the support police and crisis services can provide, and how you can plan with them to keep them safe.
Victoria Police have a range of discretionary response options available to them when responding to reports of family violence. It is important that you are aware of the different types of action police can take when discussing options with a victim survivor. Responses can include, but are not limited to:
- Crisis responses and attending a family violence incident in response to a ‘triple 0’ (000) call.
- Responding to reports of family violence or criminal offences in person or by contacting local police stations (that is, non-emergency reports).
- Laying charges.
- Issuing a Family Violence Safety Notice.
- Making an intervention order, which may include conditions such as exclusion of an individual from a property.
- Removing an individual from a property or location.
- Referring an individual to a specialist service that works with either victim survivors or perpetrators of family violence, Child Protection or child and family services.
- Referring the incident to the Victoria Police Family Violence Unit for further action or investigation.
- Providing individuals with information around next steps.
2.12 What's next?
See the flow chart diagram in Appendix 4 for how to act based on the outcome of the screening questions.
If risk is present, the diagram will guide you on what to do if there is immediate or non-immediate risk.
Use the template at Appendix 4 to develop a basic safety plan.
Professionals with responsibility for family violence risk assessment should use the information outlined in Responsibility 3.
If this is not within your role, contact another professional within your service or another service to assist. Professionals who need to make referrals, seek secondary consultation or share information should refer to guidance on Responsibilities 5 and 6 respectively.
Consider if any statutory responsibilities apply and if you may have to report to authorities in the situation.
2.12.1 Document in your organisation’s record management system
It is important that you document the following information in your service or organisations record management system:
- If you had a conversation about consent and confidentiality, and its limitations (see Responsibility 6)
- Contact details for the victim survivor, including method of contact (such as text before call) and time it may be safe to make contact
- Children’s details and if they were present
- Emergency contact details of a safe person if the victim survivor cannot be contacted
- What signs of trauma indicated to you that family violence may be occurring and led you to complete a screening tool
- If an interpreter was used in the conversation
- If you completed the Identification and Screening Tool
- If you spoke with a child or young person directly using prompting questions about their risk
- If family violence has been identified as present or not present
- The action required, that is, if you go on to undertake a safety plan, referral, secondary consultation or further risk assessment.
1. For young people over the age of 18 signs and indicators for adults apply.
2. For further information of indicators of family violence in children and young people, see the practice resource by the Department of Health and Human Services, Assessing children and young people experiencing family violence: a practice guide for family violence practitioners.
3. Adapted from World Health Organization, 2014, Health care for women subjected to intimate partner violence or sexual violence: A clinical handbook, pp 10–11
4. There are evidence-based risk factors which may indicate an increased risk of the victim being killed or almost killed. These are described as ‘serious risk factors’.
Responsibility 3: Intermediate Risk Assessment
Responsibility 3 chapter of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
Appendix 5 contains the Adult Brief Assessment Tool reflecting high-risk factors only.
Appendix 6 contains the Adult Intermediate Assessment Tool.
Appendix 7 contains the Child Victim Survivor Assessment Tool.
Appendix 8 contains the Adult Intermediate Assessment Tool within a table of practice guidance about each question to support response.
3. Intermediate risk assessment
3.1 Overview
Professionals should refer to the Foundation Knowledge Guide and Responsibilities 1 and 2 before commencing intermediate risk assessment.
This chapter should be used to guide intermediate risk assessment of the level or ‘seriousness’ of family violence risk — for either an adult or a child1. This assessment may be done directly after disclosure or identification and screening (see Responsibility 2), or to assess changes in family violence risk over time.
Key capabilities
This guide supports professionals to have knowledge of Responsibility 3, which includes:
- Asking questions about risk factors.
- Understanding the evidence-base of how questions link to the level of risk.
- Using the process of Structured Professional Judgement in practice.
- Using intersectional analysis and inclusive practice.
- Using the Brief or Intermediate Assessment Tools.
- Forming a professional judgement to determine seriousness of risk, including levels ‘at risk’ ‘elevated risk’ or ‘serious risk’.
An ‘intermediate’ level risk assessment may be undertaken using either:
- The Brief Assessment Tool reflecting high-risk factors only. The Brief Assessment Tool is for professionals providing time-critical interventions only. This assessment can be used to inform a full intermediate assessment at a later point when time or the situation allows
- The Intermediate Assessment Tool includes questions about a broader range of evidence-based risk factors experienced by adults and questions about risk to children
- The Child Assessment Tool contains a summary of adult risk factors, questions for an adult about a child’s risk and a separate set of questions for direct assessment of an older child or young person.
Guidance on undertaking an intermediate assessment to determine risk for children and young people is at Section 3.8 of this guide.
Practice considerations to assist your decision-making on how to assess risk for a child or young person include:
- creating opportunity for a child’s personal agency and voice to be heard
- individually assess their experience of risk
- wherever possible, collaborate with a parent/carer who is not a perpetrator
- reinforcing responsibility is with the perpetrator.
Remember
Guidance which refers to a perpetrator in this guide is relevant if an adolescent is using family violence for the purposes of risk assessment with a victim survivor about their experience and the impact of violence. Risk assessment and management for adolescents should always consider their age, developmental stage and individual circumstances, and include therapeutic responses, as required.
After an intermediate risk assessment, a professional may escalate the risk assessment (through secondary consultation or referral) to a comprehensive assessment to be undertaken by a specialist family violence worker.
3.1.1 Who should undertake intermediate risk assessment?
This guide should be used by professionals whose role is linked to, but not directly focused on, family violence. As part of, or connected to your core work, you will be engaging with people:
- at risk of experiencing family violence
- in crisis situations from family violence
- who are perpetrating family violence.
Do not engage directly with perpetrators about their violence if you are not trained to do so.
For further information please refer to your organisation’s family violence policies and procedures or the Responsibilities Decision Guide for Organisational Leaders (Figure 2) in the Foundation Knowledge Guide.
3.2 Structure professional judgement in intermediate assessment
Reflect on the model of Structured Professional Judgement outlined in Section 9.1 of the Foundation Knowledge Guide.
Structured Professional Judgement is the practice model that underpins risk assessment to support you to determine the level of risk and inform risk management responses. The Brief and Intermediate Tool questions are designed to support victim survivors to tell you about their experience of family violence, to inform you about the current level of risk and history of violence.
Risk assessment relies on you or another professional ascertaining:
- a victim survivor’s self-assessment of their level of risk, fear and safety
- the evidence-based risk factors identified as present.
You can gather information to inform this approach from a variety of sources, including:
- interviewing or ‘assessing’ the victim survivor directly
- requesting or sharing, as authorised under applicable legislative schemes, with other organisations and services about the risk factors present or other relevant information about a victim or perpetrator’s circumstances.
Secondary consultation and information sharing are more fully described in Responsibilities 5 and 6, and in the Family Violence Information Sharing Guidelines.
An intersectional analysis lens must be applied as part of Structured Professional Judgement. This means bringing an understanding that a person may have experienced or be experiencing a range of structural inequalities, barriers and discrimination throughout their life. These experiences will impact on:
- their experience of family violence
- how they manage their risk and safety
- their access to risk management services and responses.
Professionals should consider any additional barriers for the person and make efforts to address these.
Your analysis of these elements and application of your professional experience, skills and knowledge are the process by which you determine the level of risk.
Figure 1: Model of Structured Professional Judgement
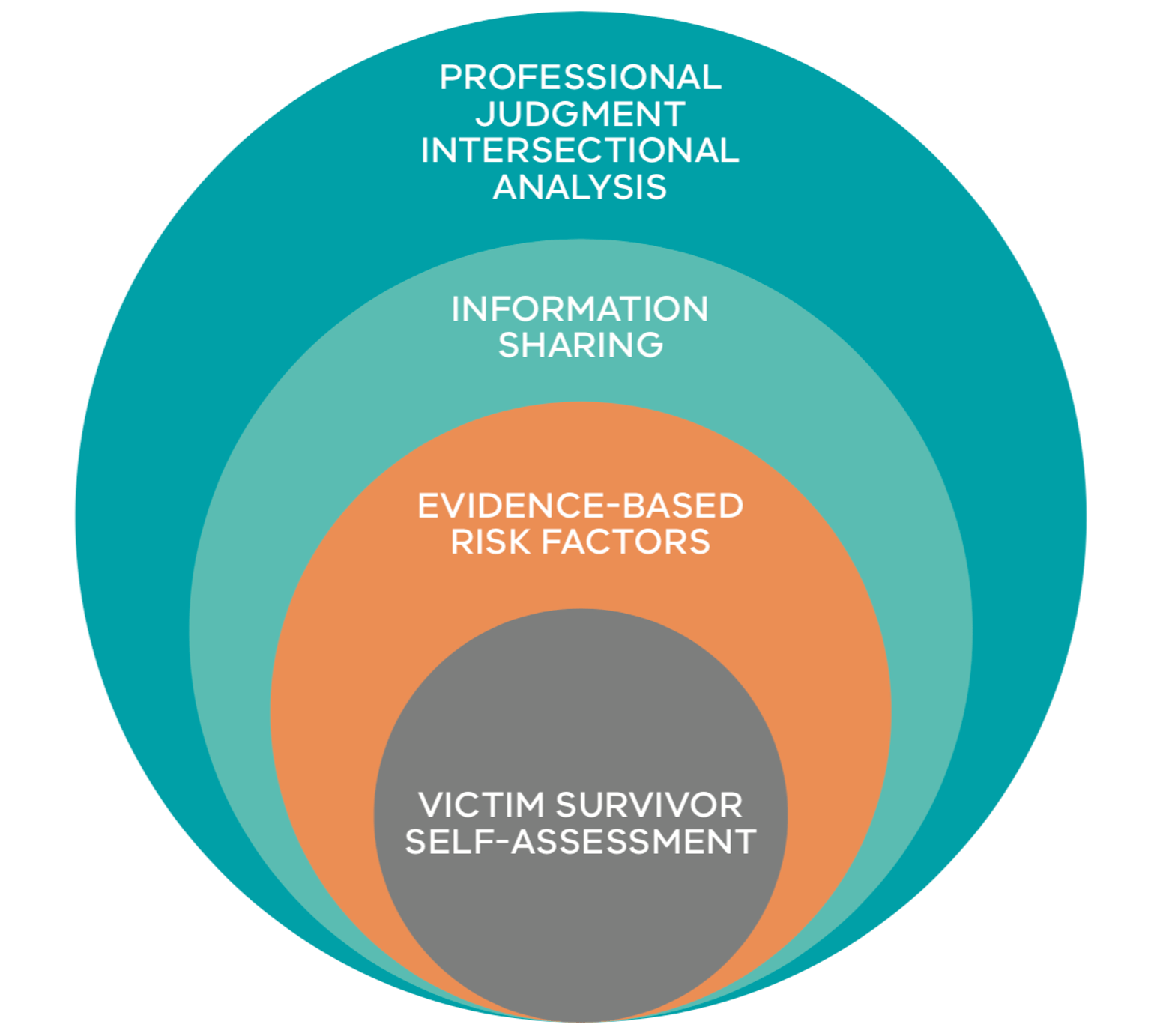
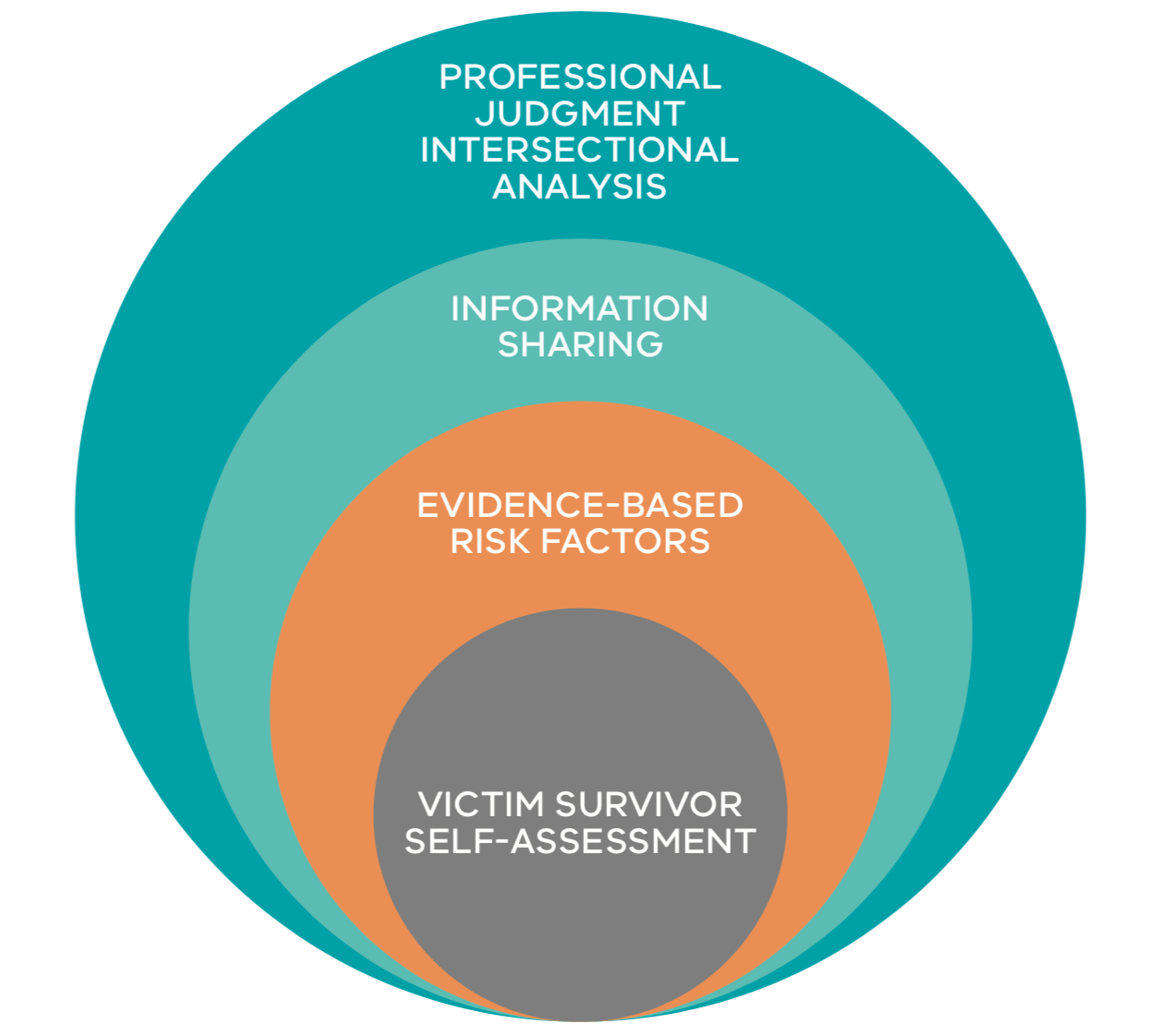{kind=link}
3.2.1 Information sharing to inform your assessment
Information sharing can inform your risk assessment.
See Responsibility 6 for further guidance on understanding what is ‘risk-relevant’ information when sharing and, if authorised, the Family Violence Information Sharing Scheme Guidelines and Child Information Sharing Scheme Guidelines on how to make requests and share information.
You can request information from other professionals or services concurrently with undertaking risk assessment with a victim survivor. There are some circumstances where you may request information before assessing risk with a victim survivor. Examples may include:
- Where you cannot engage with a victim survivor to undertake an assessment with them due to their fear of discovery by a perpetrator or third party
- Where high-risk factors are identified as present by a professional or service and it is not safe, appropriate or reasonable for a victim survivor to engage in an assessment at that time and risk management responses are required to intervene to reduce or remove (manage) an identified threat.
3.3 Intersectional analysis and inclusive practice in intermediate assessment
Experiences related to a person’s identity, including experiences of barriers and discrimination, can influence how a victim survivor might:
- Talk about and understand their experience of family violence or recognise that what they have experienced is a form of family violence.
- Understand their options or decisions on what services to access based on actual or perceived barriers. This may be due to past discrimination or inadequate service responses from the service system, including from institutional or statutory services.
- Perceive and talk about the impact of their experiences of family violence.
Be open to the ways that victim survivors might present and ask about and engage with them in ways that are responsive to their lived experiences. This may include:
- Asking about and recording concerns the victim survivor has and consider these in how you undertake risk assessment and the risk management responses you develop with them.
- Seeking secondary consultation and possible co-case management with a service that specialises in responding to diverse communities in the context of family violence (see Responsibility 5, 6 and 9).
- Engaging in a culturally appropriate manner, including offering to contact or engage with other agencies and/or the services of a bi-cultural worker
- Discussing any protective concerns you hold for children with the victim survivor.
- Where an adolescent is using violence discussing with an adult victim survivor the:
- Safety, risk and needs of the adolescent’s siblings and other family members.
- Any immediate risks to the safety, security and development needs of the adolescent using violence.
- The victim survivor’s capacity to take action to protect themselves, other children and family members.
It is critical for you to understand and explore:
- A victim survivor’s individual circumstances, including how the impact of family violence might be expressed.
- The underlying reasons for any reluctance the victim survivor has to use a service or engage with the service system.
- The relationship between the victim survivor/s (including each child and/ or family members) residing in the household to ascertain other risks of family violence for each person e.g. sibling abuse.
Remember
Secondary consultations with appropriate support professionals and services can assist you to provide appropriate, accessible, and culturally responsive services to the victim survivor.
Remember to challenge your biases. This can minimise the chance that any concerns you may hold arise from cultural or other misunderstandings.
See Responsibility 1 and the Foundation Knowledge Guide for more information on intersectional analysis, inclusive practice and providing a safe and accessible environment.
3.4 How to use the intermediate or child assessment tool
Standalone templates for the:
- Intermediate Assessment Tool is in Appendix 6
- Child Assessment Tool is in Appendix 7.
A table of practice guidance on each question in the Intermediate Assessment Tool is in Appendix 8.
The purpose of the Intermediate Assessment Tool is to:
- Identify the range of family violence behaviours being experienced by asking questions based on risk factors (this includes questions about risk to any children in the family/household)
- Consider the information gained through the assessment and apply Structured Professional Judgement to determine the level of risk — this will support you to understand a perpetrator’s individual behaviours and characteristics to assess whether the (adult or child) victim survivor is at an increased risk of being killed or almost killed
- Understand the level of risk at a point in time or changes in risk over time.
Questions in the Intermediate Assessment Tool are grouped according to:
- Risk-related behaviour being used by a perpetrator against an adult, child or young person
- Self-assessment of level of risk (adult victim survivor), and
- Questions about imminence (change and escalation).
There are two templates for an intermediate risk assessment:
- Assessing an adult by asking them questions about their risk (Intermediate Assessment Tool)
- Questions in the Intermediate Assessment Tool are grouped according to:
- Risk-related behaviour being used by a perpetrator against an adult, child or young person
- Self-assessment of level of risk (adult victim survivor), and
- Questions about imminence (change and escalation).
- Questions in the Intermediate Assessment Tool are grouped according to:
- Assessing a child or young person (Child Assessment Tool):
- Has a section about risk factors present from an adult victim survivor assessment. This also enables you to carry over information about a parent/ carers risk and identify factors that are relevant to the child’s assessment
- Provides additional questions that can be asked to a child/young person (if age and developmentally appropriate, safe and reasonable). These can be tailored in the language used to ensure they are age and developmentally appropriate.
An intermediate risk assessment may be guided by the victim survivor’s narrative and what they are ready to talk about. That is, the questions do not need to be asked in a strict order of the template.
Some assessments can be explored over a number of service engagements as you build rapport and enhance a professional relationship with the victim survivor. The questions are direct and explicit, because research indicates that victim survivors are more likely to accurately answer direct questions.
3.5 When to use the brief assessment tool
The Brief Assessment Tool as a standalone template is in Appendix 5.
The decision to use either the Brief or full Intermediate Risk Assessment Tool depends on whether a time-critical intervention is required, or there are other constraints to using the full Intermediate Assessment Tool. The Brief Assessment Tool is appropriate to use with adults and young people nearing adulthood only.
Brief assessment will be undertaken by frontline staff and critical responders, such as paramedics, in time-critical interventions. A brief assessment will be used when:
- There is limited time to engage with an individual.
- It is not safe to seek further detail about the family violence beyond high-risk factors.
- It immediately follows an incident.
- It is during a crisis intervention.
The Brief Assessment Tool covers all the high-risk factors and is a sub-set of the full Intermediate Assessment Tool. High-risk factors are linked to an increased likelihood of the victim survivor being killed or nearly killed.
A brief assessment can be used by yourself or another professional to later inform a full intermediate assessment, or comprehensive assessment by a specialist family violence practitioner.
All guidance following this section will refer to the Intermediate Assessment Tool and is applicable if the Brief Assessment Tool is being used.
3.6 Using prompting questions
“The question is not what is important. It is the answer. We need to be careful that our focus is on the answer rather than preparing for the next question.”
Family Violence Intake Worker
You can start an intermediate assessment conversation by providing context to why you are asking the questions, your role and the role of your organisation.
You can then use prompting and open- ended questions to support the victim survivor to tell their story in their own words, before moving on to ask specific questions in an assessment to draw out important information about risk factors.
Remember
Using prompting questions is also explored in Responsibility 2.
Prompting questions for children and young people are outlined in Section 3.8.
Your objective is to encourage the victim survivor to tell their story in their own way. This will assist in making the risk assessment feel less like a checklist of questions. Prompting questions can also be used during risk assessment to encourage conversation.
If you are working in a universal service that the person is accessing for another purpose, you may seek to use prompting questions to introduce the assessment and its purpose.
You could lead into the questions by describing the assessment structure, with a statement such as:
- “You have let me know that you are experiencing family violence from [name of person/relationship]. Risk assessment is the next step we take in this organisation”
- “It sounds like you are really worried about (adolescent’s/perpetrators) behaviour and the impact it is having on you and/or other children/family members. It’s important to understand the risks of this behaviour. I’d like to ask you some questions to understand this better”
- “I would like to ask you a series of questions that have ‘yes’, ‘no’ or ‘don’t know’ answers. The questions are quite direct as it is important for me to understand the risk you may be experiencing from the behaviour of [name of person using violence, if disclosed]”
- “This will help me to understand how serious the risk is, and what we will decide together to do next”
- “We will start with questions about the [name of person using violence, if disclosed] and then ask about your level of fear and questions about children (if there are any)”
- “Usually we undertake the assessment over a short period of time (in a single sitting or over a few sessions). This is important as risk level is understood as a ‘point-in-time’ assessment. If we continue to work together, letting me know about changes in risk over time can help me to understand if your level of risk has changed and if we need to change how we are responding to keep you safe”
- “If you need a break at any point during the assessment, just let me know”
Key prompting questions to ask prior to introducing the risk assessment tool, that will open the conversation, build rapport and trust, and elicit important information relevant to risk, include:
- “Could you tell me about the most recent incident?”
- “How long has this been going on?”
- “In your view, is the situation getting worse?”
- “What is the most serious thing that has happened?”
- “Do you think the situation will continue?” If not, why not? If yes, why?
After you have introduced and completed asking direct questions about family violence risk factors in the assessment tool, you should then explore more detail about the risk factors through open-ended questions, such as:
- “We have talked about the last incident. Can you tell me more about previous incidents? Have you noticed a pattern to their behaviour?”
- “What do they do that hurts / scares / controls you or your children?”
- “What do they do that gets in the way of your relationship with your children / the way you parent them?”
- “What do they do that makes you afraid for yourself, (if an adolescent) your other children, or themselves (in the case of self-directed violence, for example, including self-harm or threats to suicide)?”
- “Have they ever hurt or threatened to hurt your pets?”
- “Is there something I should be asking you that I have not asked?”
Remember
Women may be reluctant to disclose violence for a range of common reasons, such as: fear of the consequences (including of the perpetrator carrying out threats of violence or escalation, or involvement of statutory services or justice interventions); concerns they won’t be believed; shame; or thinking that they are to blame for the abuse. A further range of reasons are outlined in Responsibility 2.
Throughout the assessment process, you should explore if some of these reasons are present so you can respond appropriately and support the person to feel safe to disclose.
3.7 Understanding the assessment process and risk levels
In a full intermediate assessment you will seek answers to all questions, or as many as possible. This can be done through conversation or direct questioning, as appropriate.
Your analysis of the elements of Structured Professional Judgement and application of your professional experience, skills and knowledge are the process by which you determine the level of risk.
Remember, you can seek secondary consultation from a specialist family violence service if, for example, some high- risk factors are present that may require a specialist response, or there is a perceived difference between what a person has told you and what you have observed.
3.7.1 Responses to questions
The questions in the Intermediate Assessment Tool are seeking to elicit answers about the presence of family violence risk factors. It is key that you believe a person if they are disclosing that family violence is occurring2. The responses to questions are ‘yes’, ‘no’, and ‘not known’. If the answer is ‘yes’ there are some follow- up questions in Appendix 8 that can further inform your assessment.
If you cannot ascertain the answers to a question, then select ‘not known’. This may be if you don’t have the opportunity to ask the question or if you don’t get a clear response. You should make a comment if you haven’t been able to ask the question, especially if the question relates to a high- risk factor.
A risk factor may be indicated if the person discloses that the risk factor is present. It may also be indicated if you have noticed observable signs, or you have received the information from another professional or service, or a third party. The context and circumstances of risk factors that are identified should be noted in comments.
3.7.2 Risk levels or ‘seriousness’
Before undertaking risk assessment, it is important that you understand the levels of risk which denote ‘seriousness’, outlined below.
Table 1: Levels of family violence risk
There are three recognised levels of risk, ‘at risk’, ‘elevated risk’ and ‘serious risk’.
‘Serious risk’ can also ‘require immediate protection’, or not. This can change and escalate over time.
| At risk | High-risk factors are not present. Some other recognised family violence risk factors are present. However, protective factors and risk management strategies, such as advocacy, information and victim survivor support and referral, are in place to lessen or remove (manage) the risk from the perpetrator. Victim survivor’s self-assessed level of fear and risk is low and safety is high. |
| Elevated risk | A number of risk factors are present, including some high-risk factors. Risk is likely to continue if risk management is not initiated/increased. The likelihood of a serious outcome is not high. However, the impact of risk from the perpetrator is affecting the victim survivor’s day-to-day functioning. Victim survivor’s self-assessed level of fear and risk is elevated, and safety is medium. |
| Serious risk | A number of high-risk factors are present. Frequency or severity of risk factors may have changed/ escalated. Serious outcomes may have occurred from current violence and it is indicated further serious outcomes from the use of violence by the perpetrator is likely and may be imminent. Immediate risk management is required to lessen the level of risk or prevent a serious outcome from the identified threat posed by the perpetrator. Statutory and non-statutory service responses are required and coordinated and collaborative risk management and action planning may be required. Victim survivor’s self-assessed level of fear and risk is high to extremely high and safety is low. Most serious risk cases can be managed by standard responses (including by providing crisis or emergency responses by statutory and non-statutory (e.g. specialist family violence) services. There are some cases where serious risk cases cannot be managed by standard responses and require formally convened crisis responses. Serious risk and requires immediate protection: In addition to serious risk, as outlined above: Previous strategies for risk management have been unsuccessful. Escalation of severity of violence has occurred/is likely to occur. Formally structured coordination and collaboration of service and agency responses is required. Involvement from statutory and non-statutory crisis response services is required (including possible referral for a RAMP response) for risk assessment and management planning and intervention to lessen or remove serious risk that is likely to result in lethality or serious physical or sexual violence. Victim survivor self-assessed level of fear and risk is high to extremely high and safety is extremely low. |
3.7.3 Determining seriousness or level of risk
The process of applying the Structured Professional Judgement model includes identifying and analysing the presence of risk factors to help you determine the level of risk. This includes high-risk factors and how, based on the perpetrator’s behaviour and circumstances, they have changed or escalated in frequency or severity.
Children and young people’s risk should be independently assessed, and your assessment of them will be informed by the risk level for an adult victim survivor, and vice versa. Further guidance on assessing risk to children and young people (both directly and indirectly) is in Section 3.8 of this chapter.
Every question contained in the Intermediate Assessment Tool is connected to the family violence risk factors outlined in the Foundation Knowledge Guide. Some risk factors are described as ‘high risk factors’ that strong evidence shows are crucial indicators that the victim survivor is at an increased risk of serious injury or death.
REMEMBER
In considering the level or seriousness of risk:
- A lower level of risk is determined if an assessment indicates:
- Risk factors are not present or are rarely present.
- The high-risk factors are not present.
- A higher level of risk is determined if an assessment indicates:
- Self-assessment of risk is high.
- Risk factors are present, particularly high-risk factors.
- Risk factors, particularly high-risk factors, have changed/escalated in severity, likelihood (has continued and past behaviour indicates it will occur in future) and timing (change in frequency or escalation), and the degree of change indicates a more serious level of risk.
3.7.4 Reviewing risk assessment over time
The level or seriousness of family violence risk is dynamic and may change or escalate over time due to:
- Changes or escalation in frequency or severity of the perpetrator’s behaviour to a victim survivor
- A change in each individuals’ circumstances (that can reflect the domains of protective factors, as well as specific risk factors relating to circumstances for adults and children)
- Changes in perpetrator behaviour toward a child or young person in response to their developmental stage.
Remember
You may determine the risk level based on a single assessment.
Risk is also dynamic and can rapidly change, resulting in changes to the level of risk. Ongoing risk assessment and management is a part of all professionals’ responsibilities.
A key to understanding seriousness of risk is to understand how risk escalates or changes in severity or frequency over time.
It is therefore important to regularly revisit risk questions with an individual. Understanding a victim survivor’s risk over time involves undertaking risk assessment at a ‘point in time’ and comparing with previous risk assessments/information (that is, analysing the trend and change of behaviours used by the perpetrator). This process of conducting point-in- time assessment and review of previous assessments is referred to as ‘ongoing assessment’. Further detail on ongoing assessment is outlined in Responsibility 10.
A person may not disclose all information about their experience of family violence, and professionals can use their judgement when they have concerns that they have not gained a complete understanding of the risks that may be present.
3.7.5 Practice considerations in determining level of risk:
Victim survivor’s self-assessment of risk, fear and safety:
Evidence is clear that an adult victim survivor’s self-assessment of risk is a crucial input to your assessment. Where self- assessment indicates that the adult victim survivor considers themselves (or any child victim survivor) to be at serious risk, this is key information about the level of risk, even if other risk factors have not been identified as present.
An adult’s self-assessment of fear, risk and safety is also relevant to assessing the risk to a child. An adolescent/young person who is closer to adulthood may be asked to self- assess their risk.
There is no current evidence base that a younger child’s self-assessment of risk is reliable in determining their level of risk. However, asking the child or young person about their experience of fear may support validation of their experience by supporting them to feel heard, and for you to consider in your risk management responses.
Practice tip
Evidence shows that adult victim survivors are often good predictors of their own level of safety and risk and that this is the most accurate assessment of their level of risk. However, some victims may minimise their level of risk. Therefore, it is critical that you check if the victim survivor’s behaviour matches their reported level of fear and ask questions to explore this. A victim survivor- led approach to risk assessment and safety management recognises that clients are the experts in their own safety and have intimate knowledge of their lived experiences of violence3.
Self-assessment for adult victim survivors is explored through a set of questions in the Intermediate Assessment Tool in Appendix 8.
When introducing the self-assessment, you can ask the victim survivor to rate on a scale from 1 (not afraid) to 5 (extremely afraid), for example:
“How afraid of them are you now?”
Such as a 1-5 scale comprising:
- 1 not afraid
- 2 slightly afraid
- 3 moderately afraid
- 4 very afraid
- 5 extremely afraid
You can also ask how their current fear compares to the victim survivor’s experience at their most afraid:
“What is the greatest level of fear you have experienced in your relationship?”
This can assist you to explore what was happening for the victim survivor at that time to further understand the history of violence. A victim survivor’s level of fear should also guide you on whether any immediate management responses are required from current violence or threats of repeated violence that has occurred in the past.
Remember
Serious risk may be indicated from a single incident or experience of a high-risk factor only. However, it is also important to explore whether risk factors have occurred over a period of time, and changes to severity and frequency over time.
Severity:
Severity can be explored by asking about current risk factors and history of violence and their impact on the victim survivor. Often risk factors that indicate serious risk based on the severity of violence can be identified, such as sexual assault, physical harm, strangulation or choking, particularly when this violence has resulted in a loss of consciousness.
An example of exploring this question may be:
- “Have they ever physically assaulted you?”
(If yes)
- “Can you describe the assault/s?”
(Allow them to reply — then ask)
- “Were you ever hospitalised due to an injury sustained during an assault?”
- “Has the frequency or severity of the assaults changed in any way recently?”
Risk factors may change over time and some may increase in severity. A perpetrator may change their behaviours and their impact may become more severe to the victim survivor. If a risk factor has changed to increase in severity, recently or over time, this should be noted as indicating an escalation in violence and a serious risk.
Frequency
Frequency by itself is not always the indicator of the level of risk — you should explore further to understand if frequency has changed or escalated. This is particularly important for some high-risk factors.
If a victim survivor has disclosed a risk factor is present, you can explore changes in frequency and escalation by providing examples of time periods and asking, “How frequently?” to establish a baseline — before asking “has this changed in frequency or escalated recently? Over time?”.
Change or escalation in frequency or severity:
After you have explored frequency, you can also ask related questions about change in behaviours/risk factors that might indicate escalation in either severity or frequency.
If the types of behaviour the perpetrator is using have changed in terms of frequency or severity, this would indicate escalation of risk. It is a strong indicator of serious risk if the perpetrator is using more specific threats or has increased their use and severity of violence.
You should also consider the scale of the escalation and the impact on the victim survivor.
Practice tip
Exploring risk factors used by the perpetrator enables you to concentrate on assessing the perpetrator’s behaviour, beliefs and attitudes, personality and situational factors that increase the risk posed by them.
It is important to explore with the victim any (changes in) circumstances that may lead to an escalation in violence from the perpetrator. For example, a recent:
- Separation may challenge the perpetrator’s self-belief about their role or position within the family, such as a partner or parent.
- Court order excluding the perpetrator from the family home.
- Family Court order removing or restricting access to children.
3.8 Intermediate risk assessment for children and young people
Note: The prevalence of family violence against women and children, and against women as mothers and carers, is well established and recognised across the service system. Acknowledging this, the following section on risk to children uses gendered language to describe experiences for mothers, including damage to the mother/child bond caused by perpetrator behaviours. However, it should be noted that this guidance also applies to all forms of families and parenting.
Language in this section of ‘mother/carer’ refers to a parent/carer who is not using violence (not a perpetrator).
Children and young people affected by family violence are victim survivors in their own right, with unique experiences of family violence and its impacts. Children and young people should have their risk independently assessed. This should then be considered alongside the risk being experienced by mother/carer to collectively inform your determination of the level of risk for each family member.
When assessing risk for children and young people, you should:
- Reflect on previous guidance that outlined risk factors specific to a child or young person (Foundation Knowledge Guide).
- Build on your observation of signs of trauma that may indicate family violence in children and young people (Responsibility 2).
- Build on any response to screening questions (Responsibility 2).
The Child Assessment Tool can be completed from information received from a range of sources, including from:
- The mother/carer about a child or young person’s experience of risk. Noting also that a mother/carers own experience of risk is relevant to the experience of risk for a child.
- The child or young person directly about their experience.
- Other professionals and services. You should proactively seek and share information relevant to a child’s experience of family violence and, their wellbeing and safety, as authorised by the Family Violence Information Sharing Scheme and Child Information Sharing Scheme, or other legal authorisation, to inform your assessment.
The Child Assessment Tool is divided into 2 sections:
- Questions to ask a mother/carer about a child/young person. You can complete the list of risk factors present for a mother/carer from a previous assessment undertaken with them, if applicable.
- Questions designed to ask a child or young person directly.
The approach you choose to how you assess risk for a child should consider what is appropriate, safe and reasonable in the circumstances and may include asking questions:
- To a child/young person directly (appropriate to their age/developmental stage), with or without their mother/carer present.
- Of a mother/carer to indirectly assess the risk for a child/young person.
- To another appropriate adult family members or professionals who work with the child/young person to indirectly assess the risk for a child/young person.
Some direct questions may be asked of children from around the age of 3+ years, noting that this will need to be appropriate to the age and developmental stage of the child, and where possible with a mother/ carer present. Prompting questions for children and young people may be most appropriate to ask directly to this age group (see Responsibility 2).
In deciding whether to assess a child or young person directly or indirectly, you should take into account their age, development stage and circumstances. You should also consider whether it is appropriate, safe and reasonable to do so.
In some cases, an adolescent using family violence may be experiencing risk themselves. For example, adolescents may be:
- Experiencing family violence from another family member.
- At risk of self-harm or suicide.
- Using violence, which may or may not also relate to developmental delay or psychosis (whether drug-induced or otherwise).
Responses to an adolescent’s experience and/or use of family violence (if applicable) must include therapeutic support and be appropriate for their age and developmental stage.
Practice tip
Some professionals use language such as ‘protective parent’ or similar, which seeks to acknowledge the protective actions a mother (parent/carer) who is not a perpetrator has taken to protect the child in situations of family violence.
This term should not be considered to infer that a non-violent parent/carer is responsible for preventing violence. The responsibility for using violence and its impacts on adult and child victim survivors sits with the perpetrator alone.
3.8.1 Practice considerations for directly or indirectly assessing risk for a child or young person
Remember
The MARAM Framework principles guide professionals to recognise:
- Family violence may have serious impacts on the current and future physical, spiritual, psychological, developmental and emotional safety and wellbeing of children, who are directly or indirectly exposed to its effects, and should be recognised as victim survivors in their own right.
- Services provided to child victim survivors should acknowledge their unique experiences, vulnerabilities and needs, including the effects of trauma and cumulative harm arising from family violence (see Foundation Knowledge Guide Section 10.3).
While consent is not needed to share information in order to assess or manage risk to a child under the Family Violence Information Sharing Scheme, or to promote their wellbeing or safety under the Child Information Sharing Scheme, professionals are encouraged to take all reasonable steps to seek and obtain the views of the child and/ or the mother/carer who is not a perpetrator before sharing the information.
The practice considerations outlined below aim to assist professionals to put these principles into practice.
Practice considerations to inform your decision-making on how to assess risk for a child or young person reflect the MARAM Framework principles above, as well as a trauma and developmental lens, and include the following:
- Create opportunity for a child’s personal agency and voice to be heard: enquire to understand children and young people’s own identity and experience.
- Individually assess their experience of risk: directly assess risk with the child or young person where appropriate, safe and reasonable to do so; identify protective factors and develop the required management responses.
- Wherever possible, collaborate with a mother/carer: support strengthening/ repairing the relationship and bond between the child and mother/carer.
- Reinforce that risk and its impacts are the responsibility of the perpetrator: in all communication with the mother/carer and the child or young person, make sure they are aware they are not responsible for a perpetrator’s use of violence.
Remember
The risk level of a mother/carer who is a victim survivor is highly relevant to the risk level of any child victim survivors, and vice versa. Still, it is critically important that, wherever possible, you create the opportunity in your risk assessment practice to hear from a child or young person directly to conduct a specific and individual risk assessment for each child or young person in a family.
To determine if assessing risk directly with a child is appropriate, safe and reasonable for their age, developmental stage or circumstances, consider:
- Is it currently a crisis situation?
The safety of children, young people and adult victim survivors is paramount, and a child’s risk may be indirectly assessed through a mother/carer in crisis situations.
- Who is the primary service engagement with/who is present?
You should start assessment of the client who is present. You should also identify other family members, including children, who may also be at risk of or using family violence (in some families there may be more than one person).
- Is the child present or able to attend the service?
If the child is not present or not your primary client, consider if it is appropriate to ask a mother/carer to bring the relevant child or young person to a subsequent appointment to enable direct assessment.
- Are you suitably trained in working directly with children and young people?
If not, are there staffing and service arrangements that can be made to support you to work directly with a child or young person to assess their risk?
What other services should be engaged to assist in direct assessment of a child or young person?
If assessing risk directly:
- Is there a parent/carer (usually a mother) or appropriate safe adult who can support the child or young person in the assessment?
- Have you determined if there is a ‘protective’ parent/carer (who is not a perpetrator)? Are they aware of the risk being experienced by the child/young person?
- Is your service or another service engaged with the parent/carer to gauge their understanding of the child’s experience of risk?
- What are the views and wishes of an older child or ‘mature minor’ to a parent/ carer being present? — or an alternative support person present?
- Is there an alternative appropriate adult (such as another adult family member or other professional) who works with this child who can support risk assessment with a child or young person?
Note: None of the practice considerations should limit the recognition of children and young people as victim survivors in their own right. Through each approach to assessing risk for children and young people, you should maintain a lens on their individual experiences, vulnerabilities and needs, and respond to the impacts of trauma and harm.
3.8.2 When assessing risk to children you must also consider their wellbeing and needs
Professionals need to use their professional judgement of the individual circumstances for each case as to how they respond to the wellbeing and needs of both the child and adult victim survivor. When undertaking risk assessment and management planning, you and the mother/carer who may also be a victim survivor, need to consider the wellbeing and needs of the child or young person, including the vulnerability of the child, such as the in/ability of children to take action and move away from danger when violence is occurring, and to privilege thinking about the child’s wellbeing and needs, especially as the age and developmental stage of the child mean they are not able to do this for themselves.
Further guidance on understanding a child or young person’s wellbeing and needs can be undertaken through assessing protective factors in Section 3.9.
3.8.3 Challenges to assessing risk to a child or young person, or through a parent/carer or other appropriate third party
To facilitate direct risk assessment with a child or young person, you may need to address barriers to engagement by parent/ carers disclosing risk to children and young people. These may include:
- parental shame
- fear of statutory intervention and child remova
- seeing questions as intrusive and undermining, particularly if a perpetrator has used violence to attack the child- mother bond
Undermining the mother-child bond
Perpetrators often undermine an adult victim survivor’s (usually mother’s) bond with their child. To understand the impact of violence on children and young people you should maintain a lens on the child-mother/carer bond and parenting.
This is commonly based in social norms and gender stereotypes about women as primary carers who are responsible for children’s health, wellbeing and development. Attacking the mother/carer in this role has direct impacts on both the child and their mother/carer. Additionally, perpetrators may undermine a mother/ carers relationship and attachment with other children or stepchildren in the family/ household.
Often perpetrators expose children and young people to family violence against their mother/carer as a tactic to attack or undermine the child-mother/carer bond. Exposure to family violence is a direct risk for children and young people that can disrupt their attachment and development, and impact their safety, needs and wellbeing.
You should:
- Recognise and respond to the impact family violence has on children and young people including wellbeing and needs, emotional, social, and educational challenges, and attachment or bond with the mother/carer.
- Not blame the mother/carer or children/ young people for the family violence or its impacts.
- Strengthen the child-mother/carer bond and parenting confidence and capability that may have been undermined by the perpetrator’s family violence behaviours.
- Advocate to services and systems, in partnership with the mother/carer, so that they are not held responsible for managing the perpetrator’s actions and behaviour or its impact on children and young people.
More detail on how perpetration of family violence impacts on women (and other caregivers, kin or guardians) as parents is provided in the Foundation Knowledge Guide in Section 10.2.
Other barriers to engagement
Engagement with children about violence may also be hindered if the mother/carer is concerned about:
- Re-traumatising or upsetting children by talking about the violence with them.
- Mandatory reporting requirements and the repercussions for them and their child.
- Being judged and having their parenting/ caring role undermined instead of responsibility being placed on the perpetrator for the child/young person experiencing family violence (directly or from exposure).
These concerns from mothers/carers may override understanding their child/children’s experience of living with family violence. Addressing the fear and stigma related to children’s experience of violence with the parent/carer can support building trust to engage with the assessment process.
Building trust and rapport
You can build trust with an adult victim survivor by affirming their role as a mother carer. This can help you to assess children’s risk, both directly and indirectly. You can discuss the child or young person’s needs and wellbeing with the mother/carer, including any issues relating to the impacts of trauma for the child, such as signs observed through their behaviours (see Responsibility 2, Appendix 1).
You can also support a mother/carer to repair the child-parent/carer bond, by modelling safety, help-seeking behaviours and being aware, affirming and responding to the experience of children (fear, risk, safety, needs and wellbeing).
An effective approach to building rapport and trust with a mother/carer can be by having a conversation with both a child/ young person and their mother about the risk being experienced by the child/young person. This will involve you asking some questions to:
- the mother/carer about the child or young person’s experience, as well as
- direct questions to the child or young person
It is important to give permission, space and time to the child or young person to discuss sensitive matters, including their experiences of risk, safety and wellbeing.
If an adolescent is being assessed as experiencing violence, and they are also using violence, do not include the adolescent in a joint conversation with a parent carer, but ask if they would like another appropriate support person present.
Note: Following assessment and depending on the level of risk, you may determine that a report to Child Protection or a referral to a service with expertise in child and infant development, such as Child FIRST, and/or mental health may also be appropriate (for example, child or family services). If so, consider how you may support the parent/ carer who is not a perpetrator in this process. (See Responsibilities 5 and 6 for further information on secondary consultation and referral).
Guidance on approach to assessment of a child or young person (directly or indirectly)
Table 2 outlines approaches to assessment with children based on their age and developmental stage.
Assessment can occur directly with children and young people, if safe, appropriate and reasonable to do so, which includes considering their age and developmental stage.
Table 2: Approaches to risk assessment of children
| Age | Approach to assessment of a child or young person (direct or indirect) |
|---|---|
Infants and younger children (0–5 years) | If infants are suspected of being at risk from family violence, a full intermediate assessment of the adult victim survivor and the child must be done. Assess indirectly by asking questions with the mother/carer who is not a perpetrator, considering your observation of signs of trauma that may indicate impact from family violence in play and communication or other interactions with the mother/carer, or siblings (see Responsibility 2, Appendix 1 for signs of trauma that may indicate family violence). The Intermediate Assessment Tool includes questions about both the child’s experience of risk, and the experience of the adult victim survivor. Remember the experience of the child and their parent/carer who is a victim survivor are strongly related. |
Older children and young people (6–18 years) | An older child may be assessed directly, if appropriate, safe and reasonable to do so, which should consider their age, developmental stage and circumstances. The Child Assessment Tool includes questions for assessing older children (see Appendix 7). For young people aged 15–18 years, considering their age and developmental stage and circumstances, it may be appropriate to ask adult-focussed questions in the Intermediate Assessment Tool (see Appendix 6). For example, for a young person experiencing violence in an intimate partner relationship, it may be appropriate to ask direct questions that are broader than the questions specific to children and young people. If assessing risk directly:
If assessing risk indirectly, use the Child Assessment Tool questions directed to a parent/carer about risk experienced by a child or young person (see Appendix 7). |
3.8.4 Approach to assessing risk directly with children or young people
Your assessment must focus on the risk and needs of the children or young people. A list of family violence risk factors for children and young people is included in the Foundation Knowledge Guide.
Table 3 of the Foundation Knowledge Guide also outlines risk factors relating to a child’s circumstances to support you to identify external risk to a child’s wellbeing or safety. If external risk factors relating to a child’s circumstances are present, this may also indicate the presence of family violence. If a child or young person is experiencing risk in the community, consider how this is cumulatively impacting them, and also how you might manage both causes of risk.
Consider if the child or young person is at risk from people outside the family, such as in the community, in clubs or other social engagements. This may indicate there is an environment of polyvictimisation (that is, multiple sources of harm) that may connect to a child’s family violence risk.
Rapport is particularly important, as a child or young person will need to have some confidence in you before answering the risk assessment questions. Use child friendly activities and age and developmental stage appropriate supports for talking with young children. Refer to Section 1.5 “Building rapport” in Responsibility 1.
Use a trauma-informed approach to understand the child’s behaviour in terms of their experiences of abuse and fear. Considerations for children must be appropriate to their developmental stage and circumstances and should include:
- Their own views of their needs, safety and wellbeing.
- Their current functioning at home, school and in other relevant environments.
- Their relationships with family members and peers.
- Their relationship with the perpetrator.
- Their relationship with other people experiencing family violence in the family or household, particularly if it is their mother.
- Their sense of cultural safety, where relevant.
- The level of support available to them if they are a child with a disability.
- Their developmental history, including experiences of family violence or other types of abuse or neglect.
When assessing children, it is important to remember that they will have their own unique experiences of family violence and its impacts. This may include either positive or negative feelings towards the relationship they have with the perpetrator. During the assessment you should validate the child’s feelings and continue to keep the perpetrator’s accountability in focus as well as the child and each family member’s safety.
Create a place of emotional and physical safety for the child before you ask the assessment questions. Remember, it is ideal to directly ask an older child or young person about how safe they feel and what they need in order to feel safe.
Start by asking prompting questions such as:
- “What are the things that make you feel happy or that you like to do?”
- “Is there someone at home that makes you feel safe?”
- “Do you think you could talk to them if you were scared or worried?”
- “Do you feel unsafe or scared of anyone living in your home?”
Further prompting questions for children are in Responsibility 2.
3.9 Identifying protective factors for victim survivors (adults, children and young people)
Following risk assessment, you should explore with the victim survivor what ‘protective factors’ are present for them (and if relevant, any children). Protective factors alone do not remove risk. However, if protective factors are present these can help to mitigate or reduce risk and promote stabilisation and recovery from violence.
Where protective factors are identified, they must be confirmed before assessing if they mitigate or reduce the identified risks or their impacts (short or long-term). Accepting what a parent/carer describes as a protective action should be explored to ensure it is an effective protection.
Responsibility for family violence sits with a perpetrator, and often it is their actions which undermine the ability of a mother/carer to establish protective factors for themselves or their children. The ‘protectiveness’ of any protective factor is only useful to the degree a perpetrator is willing or unwilling to undermine or ignore that factor.
Some protective factors are also values- based judgements that reflect social advantage. Inability to establish protective factors due to circumstances is not representative of a deficit on the part of a victim survivor.
Remember
Protective factors may mitigate or lessen risk. They can also build resilience and support recovery where family violence has occurred. Strengthening protective factors is a key element of safety planning, reflected in the Table 4 in Responsibility 4. These may already be present and described in a safety plan or may be established through safety planning and other risk management processes.
You should take into account existing protective factors, but do not rely on them too heavily without considering the victim survivor’s view of whether the factor can protect them or has previously protected them or a child or young person from the actions of a perpetrator.
Table 3: Protective factors for adults and children
| Protective factors for adults and children | |
|---|---|
| Systems intervention |
|
| Practical/ environmental |
|
Strengths-based (Identity / Relationships / Community) |
|
You should take protective factors into account when considering risk level, but not rely on them to determine the level or seriousness of risk.
Consider an adult victim survivor’s view on whether the factor can protect them to inform:
- Your understanding of whether they are aware of the seriousness of risk.
- How to build on recognised protective factors through risk management, including safety planning.
Strengths-based protective factors for children
Adult and child victim survivors can have different perspectives on what protective factors are present for children. For adults, protective factors for children are often centred on resilience to promote stabilisation and recovery through communication, imparting values and modelling safe behaviours and relationships.
For children and young people, protective factors are important to understand the context of how they are impacted by violence and how they can be supported to strengthen their resilience.
Table 4: Strengths-based protective factors that promote children’s resilience
| Child-based Protective Factors |
|---|
Consider the age, stage and vulnerability of the child. Age is a significant factor in children’s resilience. Older children may be able to engage in activities outside the home and develop supportive relationships. Consider whether the child has/is:
|
For Aboriginal children, cultural pride and a strong sense of Aboriginal spirituality and community are important protective factors.
Connection to culture and community are also important for children from culturally, linguistically and faith diverse communities.
| Parent/carer actions to promote child’s protective factors |
|---|
The parent/carer:
|
| Family-based Protective Factor |
|---|
|
3.10 Misidentification of victim survivor and perpetrator
Refer to further guidance in the Foundation Knowledge Guide in Section 11.3 and Responsibility 7 on determining a predominant aggressor and misidentification.
In some circumstances, misidentification of the victim survivor and perpetrator occurs. Misidentification is where a victim of family violence is categorised as a perpetrator (respondent in criminal or civil proceedings) — or where a perpetrator has misrepresented themselves as a victim of violence.
Evidence and research demonstrate that relatively few men in heterosexual relationships are solely experiencing family violence or intimate partner violence. In heterosexual relationships, men are much more likely than women to be using a number of repeated, patterned forms of violence to dominate and control over time.
Through the course of your assessment if you are uncertain about who is using violence, you should refer the person to a specialist family violence service or seek secondary consultation.
Practice tip
In all circumstances where a man is initially assessed as or claiming to be a person experiencing family violence in the context of a heterosexual relationship, you should refer him to a men’s family violence service for comprehensive assessment or to the Victims of Crime Helpline. His female (ex)partner must always be referred to a women’s family violence service for assessment, irrespective of whether they are thought to be the victim survivor or the perpetrator.
It is important, however, that professionals recognise that misidentification can occur in any community or relationship type.
3.11 What's next?
The outcome of the intermediate risk assessment will inform your decision- making on what to do next. If family violence is present, you must use the guidance in Responsibility 4 on undertaking risk management on how to respond.
For example, next steps for risk management could include:
- Immediate action (calling police on 000 or making a report to Child Protection or Child FIRST/ child and family services).
- Secondary consultation or information sharing (seeking or sharing) to further inform your assessment.
- Safety planning and risk management.
- Referral to a Specialist Family Violence Service, or other services (if required).
Specialist family violence services can provide secondary consultation or receive referrals for comprehensive assessment and specialist risk management. This action:
- Must occur if the assessed level of risk is ‘serious risk’ or ‘serious risk and requires immediate protection’
- May occur if the assessed level of risk is ‘elevated risk’.
If a child or young person is experiencing risk that requires you to make a referral to Child Protection or to share information or seek secondary consultation with a service with expertise in child and infant development, refer to guidance in Responsibilities 5 and 6.
Refer to guidance on the following responsibilities:
- Responsibility 4: Intermediate risk management
- Responsibility 5: Seek consultation for comprehensive risk assessment, risk management and referrals
- Responsibility 6: Contribute to information sharing with other services (as authorised by legislation).
3.11.1 Document in your organisation’s record management system
It is important that you document the following information in your service or organisation’s record management system:
- Consent and confidentiality conversation outcome.
- Each risk assessment you undertake, the level of risk for each victim survivor and reasoning.
- Children’s details and if present — also if children’s own assessment has been completed.
- Any other relevant information such as relating to protective factors and the circumstances of the victim survivor, perpetrator and other family members
- If an interpreter was used in the assessment.
- If a support person was present and their relationship to the victim survivor.
- Contact details for the victim survivor, including method of contact (such as text before call) and time it may be safe to make contact.
- Emergency contact details of a safe person if the victim survivor cannot be contacted.
1. Intermediate assessment can be undertaken directly following disclosure from a victim survivor, without a screening assessment being first undertaken.
2. If you are uncertain about the identity of the victim survivor or perpetrator, such as where you think a perpetrator may be misrepresenting themselves as a victim survivor, refer to Section 10.2 of Foundation Knowledge Guide on how to respond.
3. ANROWs National Risk Assessment Principles, 22.
4. ANROWS, National Risk Assessment Principles for domestic and family violence: Companion resource, page 28.
5. http://providers.dhhs.vic.gov.au/criminal-offences-improve-responses-ch…
6. https://aifs.gov.au/cfca/publications/domestic-and-family-violence-preg…
7. https://www.aaimh.org.au/resources/position-statements-and-guidelines/ (Position Statement on Infants and Family Violence)
8. Ibid.
9. Ibid.
10. Australian Institute of Family Studies (2015). Children’s exposure to domestic and family violence.
11. Dawson, J. (2008). What about the children? The voices of culturally and linguistically diverse children affected by
family violence. Melbourne: Immigrant Women’s Domestic Violence Service.
12. Edleson JL 1999, ‘Children’s witnessing of adult domestic violence’, Journal of Interpersonal Violence, 14(8): 839–870
13. Harne L 2011, Violent Fathering and the Risks to Children, The Policy Press, London
14. Morris, A., Humphreys, C., & Hegarty, K. (2015). Children’s views of safety and adversity when living with domestic violence. In N. Stanley & C. Humphreys (Eds.), Domestic violence and protecting children: New thinking and approaches (pp. 18-33). London, UK: Jessica Kingsley Publishers.
15. Bagshaw, D. et al (2011). The effect of family violence on post-separation parenting arrangements Family Matters, (86).
16. Brownridge, D (2006), ‘Violence against Women Post-Separation’, Aggression and Violent Behavior, vol. 11, no. 5, pp. 514–30.
17. Kirkwood, D. (2012). ‘Just Say Goodbye’ Parents who kill their children in the context of separation. Domestic Violence Resource Centre Victoria, Discussion paper (No.8).
18. Section adapted from Victorian Government Department of Human Services (2012). Assessing children and young people experiencing family violence A practice guide for family violence practitioners.
19. Segrave, M (2017) Temporary migration and family violence: An analysis of victimisation, vulnerability and support.
Melbourne: School of Social Sciences, Monash University
20. Laing, L. (2003). Domestic Violence in the Context of Child Abuse and Neglect. Australian Domestic and Family Violence Clearinghouse, Topic paper.
21. Edleson, J. L. 2001. ‘Studying the co-occurrence of child maltreatment and domestic violence in families’, in Domestic Violence in the Lives of Children: The Future of Research, Intervention, and Social Policy, eds S. A. Graham- Bermann & J. L. Edleson, American Psychological Association, Washington, D.C.
22. Bowlby J 1969, Attachment and Loss, Basic Books, New York
23. Bunston W & Sketchly R 2012, Refuge for Babies in Crisis, Royal Children’s Hospital Integrated Mental Health Program, Melbourne, p 26
24. DHHS, with acknowledgement of Humphreys, C., Connolly, M., & Kertesz, M., University of Melbourne (2018). Tilting our practice: A theoretical model for family violence. Victorian Government, Melbourne.
Responsibility 4: Intermediate Risk Management
Responsibility 4 chapter of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
Appendix 9 contains a template safety plan for adult victim survivors which can include safety planning for children through the non-offending parent/carer.
Appendix 10 contains a template safety plan that can be used directly with older children or young people.
4. Intermediate risk management
4.1 Overview
This guide supports professionals to undertake risk management that responds to the presentation and level of family violence risk (seriousness), as identified through intermediate risk assessment (Responsibility 3).
Professionals should refer to the Foundation Knowledge Guide and Responsibilities 1–3 before commencing intermediate risk management. You should reflect on the Structured Professional Judgement model and applying an intersectional lens in particular (Responsibility 3 and Foundation Knowledge Guide Section 9.5) to inform your risk management approaches.
Key capabilities
This guide supports professionals to undertake intermediate risk management and includes:
- Working with victim survivors (adults, children and young people) to develop an appropriate risk management response based on their unique experience of risk and assessed level of risk.
- The different elements of intermediate risk management.
- Discussing staying at home or leaving and talking to adult victim survivors about their options.
- Responding to serious and immediate risk.
- Documenting evidence of family violence.
- Developing risk management strategies where there are multiple victim survivors, including children.
- Developing safety plans for children and young people, working with a parent/ carer (usually the mother) who is not a perpetrator (who may also be a victim survivor), and/or working directly with the child or young person.
You should use this guide:
- After an intermediate risk assessment (Responsibility 3) has been completed and family violence risk has been assessed as present.
- To develop risk management strategies and a safety plan in the first instance or to review and update an existing plan if family violence risk has changed and/or escalated.
Guidance on other elements of risk management including information sharing, referral and secondary consultation with other services is provided in Responsibilities 5, 6, 9 and 10.
Remember
Guidance which refers to a perpetrator in this guide is relevant if an adolescent is using family violence for the purposes of risk assessment with a victim survivor about their experience and the impact of violence. It does not refer to risk assessment and management for adolescents, which should always consider their age, developmental stage and individual circumstances, and include therapeutic responses, as required.
Professionals and services can take a wide range of actions to manage risk. The actions you take depend on your role, your organisation and the resources available to you.
4.2 What is risk management?
Risk management is a coordinated set of strategies and actions aimed at enhancing the safety of the victim survivor (adult, child or young person) and reducing or removing the likelihood that the perpetrator will commit further violence. All risk management must involve safety planning. In addition to safety planning, other forms of risk management may also be required such as discussing options with victim survivors, connection to support and services, secondary consultation, and ongoing risk assessment.
4.2.1 Elements of intermediate risk management
Intermediate risk management activities for victim survivors may include responding to a range of risks and associated needs. Key intermediate risk management actions you can take include:
- Responding to immediate risk (Section 4.5)
- Safety planning (including for children or young people) (Sections 4.6 and 4.8)
- Talking to victim survivors about options and connection to relevant services (Section 4.11)
- Ongoing risk assessment and management (monitoring for change and/or escalation) (Section 4.14).
Intermediate risk management is focused on immediate risk management and safety planning, which is outlined in this chapter.
Some intermediate risk management activities require engaging with other services for assessment and management activities, including information sharing. Practice guidance on undertaking these collaborative risk management activities is covered in:
- Responsibility 5: Seek consultation for comprehensive risk assessment, risk management and referral
- Responsibility 6: Contribute to information sharing with other services
- Responsibility 9: Contribute to coordinated risk management
- Responsibility 10: Collaborate for ongoing risk assessment and risk management.
Collaborative risk management processes increase the visibility of the perpetrator, facilitate more tailored responses and risk management strategies, and can be more timely and responsive to changes in the level of risk. These coordinated responses make victim survivors safer. Service providers who use collaborative risk management can also consider and access a range of risk management activities for victim survivors which may not be possible for services who work independently.
It’s important to continually review your assessment of risk and update risk management and safety plans, as risk levels can change quickly and at any time. Depending on your role, you may contribute to risk management in a short- term support or intervention or have an ongoing role. An ongoing role includes supporting monitoring of risk and continued collaboration with specialist services to support the victim survivor, share information, and/or maintain visibility on the perpetrator.
Remember
All professionals must still comply with their existing legal obligations, such as mandatory reporting to Child Protection (for relevant occupations) and the reporting of possible sexual abuse of children under 16 to Victoria Police (applies to all adults).
This guidance on risk management is consistent with these obligations and provides additional information on how to manage family violence risk in the context of these obligations.
4.3 Structure professional judgement in risk management
Structured Professional Judgement supports you to respond through risk management actions to the level of risk you have determined through risk identification and assessment with the victim survivor and through information sharing.
Through the process of risk management at an intermediate level, you should:
- continue to keep the victim survivors wishes and needs central to your planned risk management actions
- respond to risk factors you have identified as present, particularly focussing on high risk factors and those identified as most impactful by the victim survivor
- continue to use information sharing with other professionals and services to ensure your risk management responses are relevant and support keeping perpetrators in view
Reflect through risk management on your intersectional analysis to respond to structural inequalities, barriers and discrimination a person may have informed you they have experienced throughout their life. These experiences will impact on:
- their experience of family violence from the perpetrator
- how they manage their risk and safety, and
- their access to risk management services and responses
Professionals should consider and make efforts to address any additional barriers for the person.
Your analysis of these elements and application of your professional experience, skills and knowledge support you to respond to the level and presentation of risk for each victim survivor.
Figure 1: Model of Structured Professional Judgement
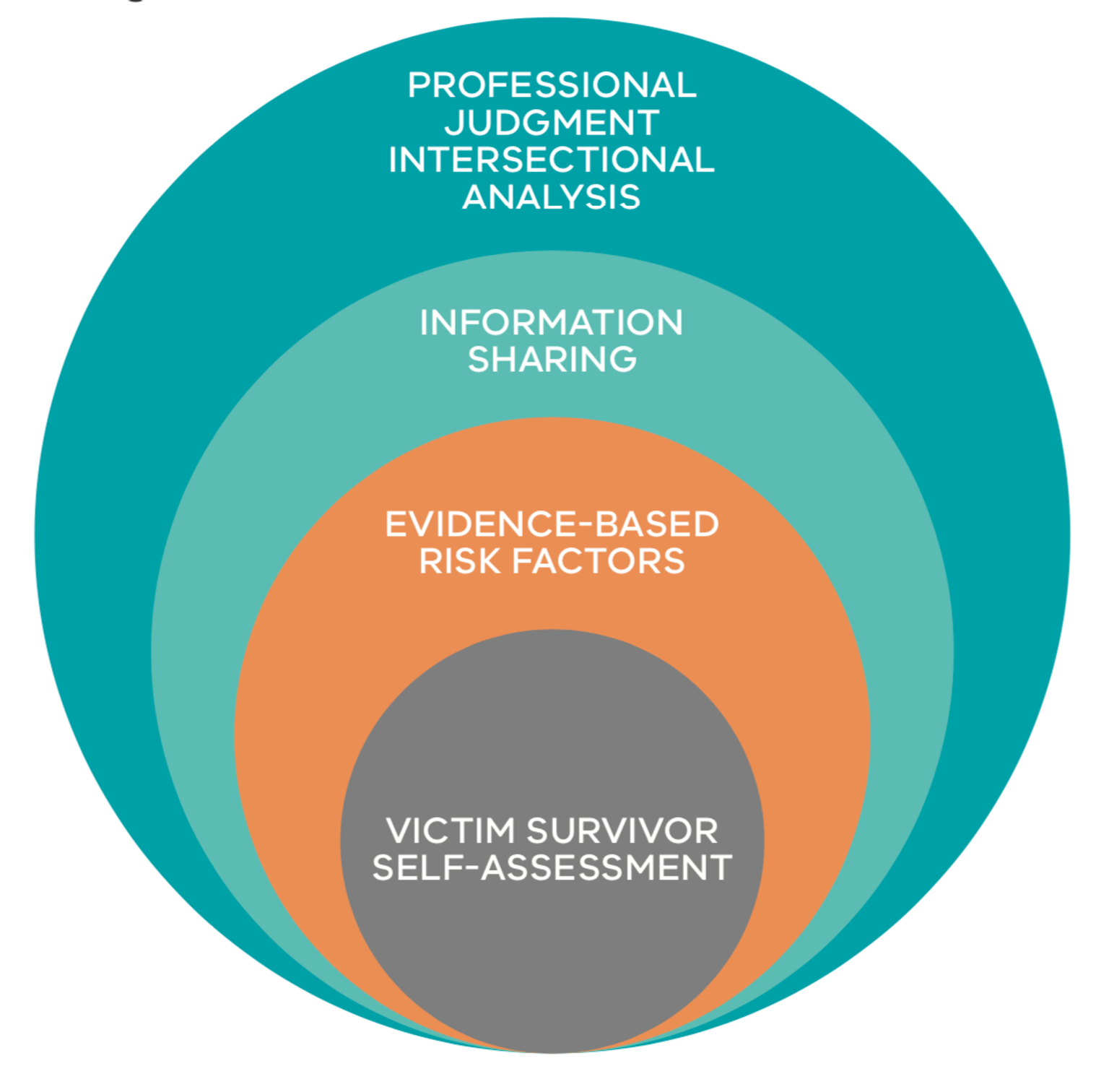
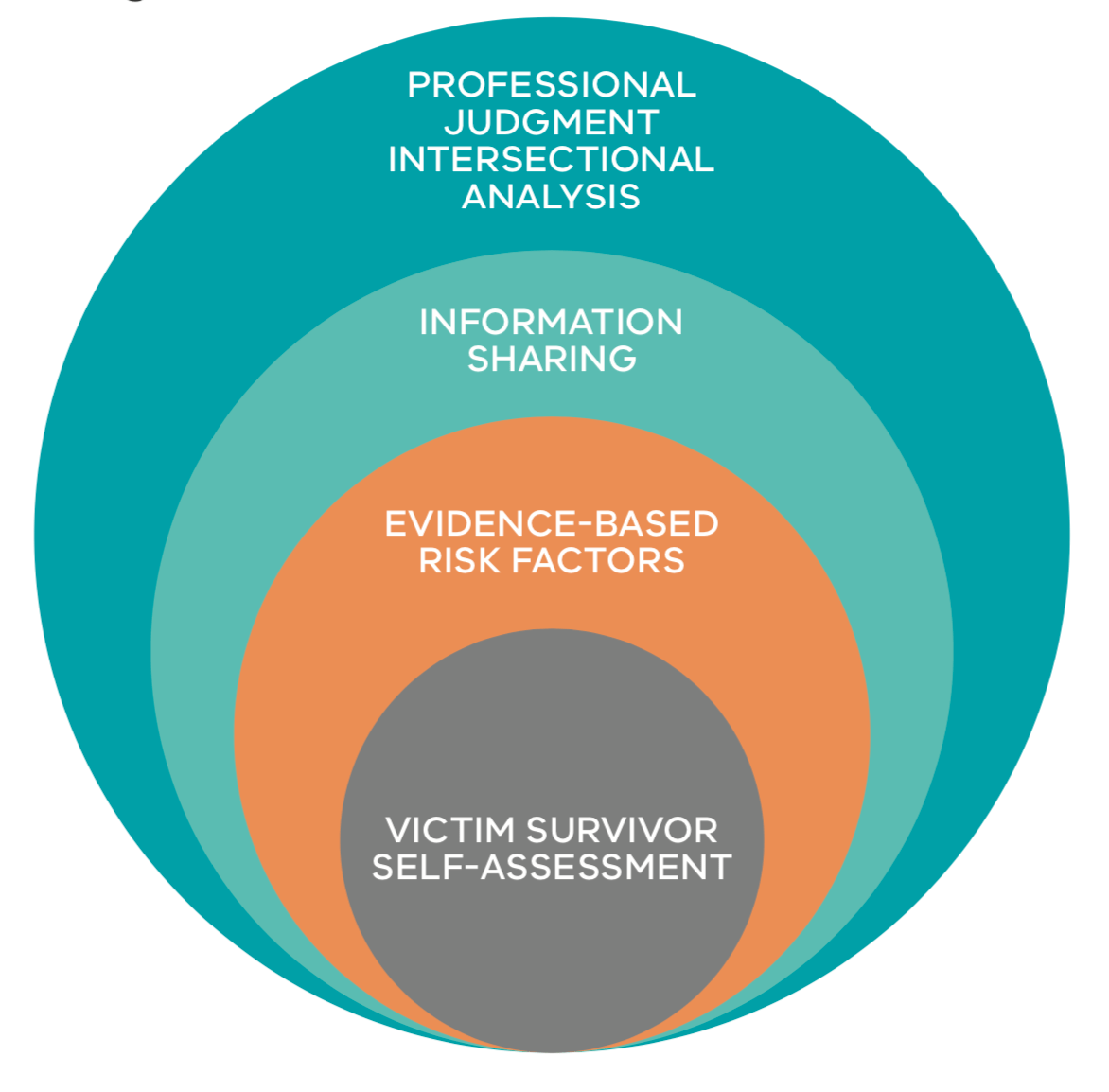{kind=link}
See guidance on secondary consultation, referral and information sharing in Responsibilities 5 and 6.
4.4 Starting the conversation about risk management
The victim survivor is an expert in their own life experiences and provides critical insight into the perpetrator’s attitudes, beliefs and behaviours.
You should recognise that the victim survivor has been taking actions to manage the risk posed by the perpetrator, including to any children who may also be victim survivors, and may have been doing so for a long period of time. The victim survivor will have likely tried many strategies to mitigate risk of violence and abuse, and its impacts. It is important to ask the victim survivor what has worked and what has not worked. We know that service involvement can be a protective factor. Therefore, ask what services or programs they have been involved with in the past.
You should start a conversation about risk management by telling the victim survivor that based on the outcome of the risk assessment you’ve undertaken, you need to work together to develop actions to support their safety.
You can begin by stating:
- “I’d like to talk to you about how we can assist to keep you (and your children, if applicable) safe.”
- “You have demonstrated strength and resilience in managing your own (and your family’s) safety — how have you done this in the past and how can we best support you with this?”
You can then ask the following questions:
- The behaviour of the perpetrator:
“Can you tell me about the impact his behaviour has had on you (and any children)?”
- The likelihood of the perpetrator repeating the behaviour:
“Can you tell me about what the pattern of behaviour has looked like in the past?”
- Service involvement:“
Can you tell me about any services that are currently supporting you or have been involved in the past?”
(These might have been legal, medical, educational, specialist family violence, housing/homelessness, AOD or mental health, disability, youth, Child FIRST or Child Protection?)
“What support did they provide to you?”
- Actions and strategies which the victim survivor has employed in the past:
“What has helped in the past that has kept you/you and your children safe?”
4.5 Responding to immediate risk
Actions to respond to immediate risk could involve:
Practice tip: Seek practice advice from a specialist family violence service.
- Contacting police (000) in crisis situations where an immediate response is required:
- You will be asked your name and where you are calling from
- Clearly explain who you are and your role, and why you are calling
- Give the full name of the victim survivor/s and their address and telephone number
- Give the full name of the perpetrator, (if known) their whereabouts and address
- Provide details about the situation, including about any crime that may have been committed, if known
- Report any risk posed to children or young people
- Provide any other information requested by the operator.
- A crisis situation may include both immediate risk from the perpetrator, as well as responding to immediate impacts from family violence, including medical response to serious/injury.
Remember
If loss of consciousness from strangulation or choking, or physical force to the head or neck is suspected or confirmed, you should seek an immediate health assessment for the victim survivor to ensure any injuries to the brain or body are responded to.
- Making a referral to a specialist family violence service, including for crisis or refuge response.
- Seeking secondary consultation from a specialist family violence service for comprehensive risk management planning or referring the victim survivor to a service for this support.
- If anyone discloses that the perpetrator has sexually assaulted a child, you have a statutory obligation to report to the police1:
- It is best practice to inform the adult victim survivor of your responsibility to report where possible. You can also reassure them that you can support them to ensure the safety of both the adult victim survivor and child from any increase in risk from the perpetrator that may occur as a result of the report
- Further practice advice about maintaining rapport and engagement can be found in Responsibility 1.
- Report the risk posed by the perpetrator to children or young people to Child FIRST/Child Protection and schools/ childcare centres (including sharing information regarding an intervention order if one is in place).
- Supporting an adult victim survivor to engage with legal services, and to make an application for:
- A family violence intervention order including for children and young people (if applicable).
- A personal safety intervention order, if appropriate, for community-based family violence or in family-like relationships, where the victim survivor does not want to apply for a family violence intervention order.
Remember
When making decisions on what course of action you should take, it is important to talk to the victim survivor about who you are contacting to seek assistance and who you are sharing information with.
You should seek the views of an adult or child victim survivor/s about sharing information about a child or young person’s risk wellbeing or needs, unless it is not appropriate, safe or reasonable to do so in the circumstances.
4.6 Safety planning with an adult victim survivor
Safety planning is thinking about practical actions a victim survivor (and/or services) can take to be safer when living with family violence.
The process looks at the current situation and assesses what steps and strategies can be put in place to mitigate risk. A safety plan must be current, relevant, adaptable and kept up-to-date in response to change in circumstances.
It is important that safety planning is discussed in a way that does not make the victim survivor feel that family violence risk or its impacts are their fault.
A safety plan may be developed by professionals who have undertaken an intermediate risk assessment, or in collaboration with, or by, a specialist family violence service (see Responsibilities 5 and 6). If a specialist family violence service is not involved, you must develop a safety plan with the victim survivor.
Where family violence risk has been identified, all victim survivors, including children and young people, benefit from having a safety plan. This supports them to know what to do if risk changes or escalates.
4.6.1 When to do a safety plan
Safety planning should be undertaken:
- Where any level of risk is present, noting that the safety plan will differ depending on the level of risk identified.
- In collaboration with the adult victim survivor, including in the development, implementation and monitoring of the plan. It may be appropriate to work with a young person to develop their own personal safety plan.
- With the adult victim survivor to develop separate safety plans for each child or young person (if not being done separately), and to reflect these plans in the adult victim survivor’s plan, if appropriate2.
All risk management must involve safety planning, and it’s key that the victim survivor participates in and understands this process. Safety planning must occur whenever family violence risk is identified and assessed and should be updated whenever there are changes or escalation in family violence.
Ensure safety plans reflect risks and management responses of each family member so that each family member’s plan supports safety requirements for each individual as well as the family unit. You also need to ask what constraints/circumstances may impact the victim survivor’s capacity to implement a safety plan.
The safety plan must be documented and should be regularly updated to reflect changes in circumstances and risk levels. Any referrals made, or secondary consultations undertaken as part of risk management should be incorporated and documented as part of safety planning. For more information, see Responsibility 5.
4.6.2 Developing a safety plan — key elements
A template safety plan is available in Appendix 9.
Each safety plan is unique to the needs of the victim survivor and should be informed by their views on what will and won’t work. It can be empowering for the victim survivor if you recognise and affirm the successful actions and strategies a victim survivor has already used in the safety plan you develop with them. Actions that are helpful in some situations might inadvertently increase their risk in other situations. You should be guided by the victim survivor on what strategies will work best in their situation.
Safety planning involves talking with the victim survivor (adult, child or young person, if appropriate) about their living and travel arrangements, community connections, financial resources and other circumstances and arrangements that support safety for themselves and their children. Each victim survivor’s circumstances are different and safety planning can cover some or all of the areas below.
A safety plan for adults should (as appropriate):
- List emergency contact numbers.
- List the contact numbers for a specialist family violence organisation, including if an Aboriginal organisation or other culturally appropriate service is being engaged.
- Identify a safe place for the victim survivor to go if they are in danger, and how to get there.
- Reflect protective factors, incorporated from what the victim survivor has discussed with you.
- Identify a friend, family member or neighbour who can assist in an emergency, and how to contact them.
- Identify a way for the victim survivor to get access to money in an emergency.
- List what to include in an ‘escape bag’ or identify a place to store valuables, so that the victim survivor can access them when needed. An escape bag at a minimum should include:
- phone/communication devices
- keys (house, car, office, etc.)
- money (cash and coins), bank cards (if the account is not shared with a perpetrator)
- medications/scripts and important documents (or copies)
- clothing for themselves and any children or person in their care
- Identify ways to safely use technology, including e-safety strategies, and the limitations of devices used, including children’s devices.
- Specifically address any barriers to the victim survivor implementing the safety plan (for example, access to funds, access to vehicles, leaving a pet behind, or having mobility or communication difficulties).
- Explore necessary ties to community, such as caring responsibilities, access to medical care, education (particularly for children and young people), access to cultural organisations or faith places, or requirements to contact justice services (e.g. parole officer).
- Consider support needs: disability support, medical care, translation, systems literacy (such as being primary person engaging with Medicare, banks and Centrelink), financial literacy or access (if usually provided by the perpetrator).
4.7 Mandatory reporting to child protection and referral to child first
Reflect on your reporting obligations that are an existing part of your professional role.
Remember
Use of the MARAM Framework andMARAM Practice Guides are in addition to existing legal obligations, including mandatory reporting to Child Protection and professionals with obligations to refer to Child FIRST.
Where it is safe, appropriate and reasonable, involve a parent who is not a perpetrator in the referral or reporting process. You can use your professional judgement to determine this — and consider how to assist them to continue engaging with your service and support them in this process. This will contribute to a person-centred approach (see Foundation Knowledge Guide Section 9.3) and partnering with victim survivors.
4.7.1 Reporting to Child Protection or child and family services
Always make a report to Child Protection if you have a significant concern that a child needs protection. Professionals should consult their organisation’s policies on making reports to Child Protection for guidance on circumstances and factors to consider.
Medical practitioners, nurses, midwives, teachers (including early childhood teachers) and school principals, and police are mandatory reporters under the Children, Youth and Families Act 2005 (CYFA) (section 182). Mandated reporters must make a report to Child Protection if they form a belief on reasonable grounds that a child is in need of protection from physical injury or sexual abuse, and that the child’s parents are unable or unwilling to protect the child from that abuse.
From March 2019, out-of-home care workers, early childhood workers, social workers, registered psychologists and youth justice workers become mandated reporters. From early 2020, school counsellors will also be included.
If the child is Aboriginal or Torres Strait Islander, ensure this information is contained in the report from your service to Child Protection. This ensures that the Aboriginal Child Specialist Advice and Support Service (ACSASS) is notified and that cultural supports are put in place.
Make a referral to child and family services, such as Child FIRST, if you have significant concerns for the wellbeing of a child or an unborn child after their birth. Consider making a referral if wellbeing or needs issues are identified AND the child’s safety is not compromised (which would require a report to Child Protection).
4.8 Safety planning for a child or young person
Language in this section of ‘mother/carer’ refers to a parent/carer who is not using violence (not a perpetrator).
A template safety plan that can be used with an older child or young person is available in Appendix 10.
Refer to guidance on working with children and young people in Responsibility 3 for determining if it is safe, appropriate and reasonable to develop a safety plan:
-
Directly with a child or young person (using the plan in Appendix 10).
-
Through a parent/carer (usually the mother) in the adult safety plan template (Appendix 9).
You should consider safety planning needs for children and young people separately to an adult victim survivor. This will assist in identifying different experiences, risks and needs from adults and other children/ affected people in the family.
Each child’s experience of risk and safety/ needs is inextricably linked to that of the adult victim survivor/carer and other children in the family. Consequently, each child or young person’s plan must also take into account and work consistently with the safety plan of the adult victim survivor and other children or family members (as applicable).
There are two aspects to safety planning for a child or young person.
Where you are working with a mother/carer who may also be a victim survivor:
-
You need to work with them to develop a safety plan for each child in the family/ household affected by family violence. This can be recorded in the mother/ carer’s safety plan.
-
The primary focus of this plan for children will be about the child or young person’s immediate safety and removing them from harm.
Where you are working directly with a child or young person:
-
If appropriate, safe and reasonable (see Responsibility 3) you can fill out the child safety plan template with the child or young person. This will enable them to be actively involved and understand how they can also be active to support their own safety.
-
Older children and young people, like adult victim survivors, often take steps to manage their experience of risk which should be acknowledged and considered in how this can be included in the plan. The child’s safety plan will also focus on how they will act in response to and in addition to the mother/carer’s actions.
-
When talking with children and young people about their safety plan you should continue to focus on their experience of violence, reflect on how they have acted in the past to keep themselves safe and that it is not their fault.
-
As part of the safety plan for the child, as well as any adult victim survivor, you should discuss parenting arrangements and the relationship between a child and parent who is a perpetrator. This may apply whether the child’s mother/carer is in a relationship, has separated or the relationship has ended.
-
Each relationship scenario will alter the parenting arrangements that are in place for the child/ren in the family. If the relationship dynamics change at any point, this needs to be reflected with an update to the safety plan.
Record the key agreed details of each family member’s safety plan together to ensure they are consistent.
This can be included in the overall risk management plan.
It is important to note that the safety plan approach will need to be adjusted according to the age and developmental stage of the child or young person, as well as whether it is appropriate, safe and reasonable to develop a safety plan with them, or if planning should occur with a mother/carer present.
Table 4: Considerations for age and developmental levels in safety planning
|
Age |
Considerations3 |
|
|---|---|---|
|
Infants and younger children (0–5 years) |
May have their safety plan contained within the adult victim survivor/carer’s plan. |
When safety planning with young children (3–5 years) you should have the mother present. Affirming to the child that everyone wants them to be safe and they are not to blame are important messages for them to hear and for the mother/carer to deliver. Practice Tip: There may be times when a safety plan for a child under the age of 3 is needed. Children at this developmental stage should have their mother/carer with them for this discussion. Because the child at this developmental stage is often too young to openly discuss the safety plan, incorporate the child’s safety plan into that of their mother/carer. |
|
Older children and young people (6–18 years) |
The child or young person’s age and developmental stage will influence the level of involvement they have. They should be included in the development of their own safety plan wherever possible, including to reflect their views and wishes. This ensures they understand the purpose of the plan and enables them to feel empowered — providing a direct response to their experience of violence. If you cannot seek the views or input of the child or young person in the development of their plan, e.g. if the child is not present, you can develop safety plans on their behalf by talking with the mother/ carer who is not using violence. It also may not be possible to create a safety plan for a child or young person in consultation with a parent who is not using violence (generally the mother). In this situation, it is important to still consider the impact of your planning on any mother/carer in their life (who is not using violence). |
6–11 years of age: You can use the template plan with older children and young people of this age. Work with the child to define and understand what family violence is. Let them know that everyone wants the child to be safe. If you are working with both a mother/carer and child or young person, safety planning with children at this developmental level can be more effectively done with the mother/carer present. 12–14 years of age: You can use the template plan with older children and young people of this age. Another option is to create a simple written agreement with the young person stating what they could do and where they could go if they feel unsafe. You should ask the young person how much involvement they need or desire from the mother/carer in developing the safety plan. You can suggest they share their safety plan with their mother/carer. 15–18 years of age: The template plan for either a child and young person or adult can be used, working directly with the young person. Young people often have a greater ability to keep themselves safe but may need help in identifying their own resources and developing a realistic plan for themselves. You should ask the young person how much involvement they need or desire from the mother/carer in developing the safety plan. Suggest they share their safety plan with their mother/carer. At this age, males especially may feel they can protect their mother by intervening in the violence. While respecting their feelings, encourage discussion and state that this may put them and their mother at more risk — let them know that it is not the child’s responsibility and the father’s behaviour requires system intervention. |
4.8.1 Talking to child victim survivors about their parent who is a perpetrator
If the perpetrator is a parent/carer to a child, this can create complex and confusing relationships and situations for the child. Sometimes children aren’t sure what impact changes between their parents/carers as a result of family violence will have on their relationship with the parent who is a perpetrator. You should consider the following:
-
When engaging a child to complete a risk assessment or safety plan it is important to understand the tactics a parent who is a perpetrator (usually a father) may use to coerce a child or young person into providing and gathering information
-
The child or young person understanding what information they can talk with the perpetrator parent about. Some information may seem harmless but is used to monitor the parent/carer or child who is a victim survivor, such as their daily activities, where they go, who they spend time with/contact with other family or friends, or other questions
-
You (and the mother/carer who is a victim survivor) recognising that a child or young person may have strong loyalty to a parent/carer who is a perpetrator. This may impact on whether the child or young person feels it is ok to share information with them (whether voluntarily, without meaning to or in response to questions from a perpetrator)
-
You should consider the experience of the child in these circumstances and how their experience of trauma and cumulative harm can change their understanding of what is ‘normal’ or ‘ok’ to talk about with the perpetrator. For example, when they ask the child for information to monitor the mother/carer or other family members.
Your approach to discussing this issue with a child or young person will depend on their age and developmental stage. Sometimes it may be appropriate, safe and reasonable to have a conversation directly with the child (guidance in Table 4 on age and developmentally appropriate actions can support your decision-making around this).
Inform the child or young person that the purpose of the conversation is safety for them or other family members. It is important to recognise the experience and impacts of violence on children and young people in this situation. In any situation, you should let the child know:
-
That they will not be in trouble for telling information to the perpetrator and emphasise that they should let their parent who is not a perpetrator, yourself or another safe person know if they have done so
-
They are not responsible for any behaviour or violence from a perpetrator which occurs if the child does share information with the perpetrator.
Practice tip: If you are not trained in working with children or young people, or feel you need assistance on risk management or safety planning, you may wish to seek advice through secondary consultation with a specialist children’s worker or specialist family violence service for their advice and support in these activities (see Responsibilities 5 and 6).
As part of a safety plan with the child or young person, it is best practice to:
-
Ask the child if the perpetrator asks them questions about the parent who is a victim survivor, or anyone else in the family
-
Suggest ways the child or young person can respond to questions from the perpetrator that are attempting to monitor or seek information about the child or a parent/carer who is a victim survivor, to further perpetuate violence
-
You can also role play options with the child on responding to questions from the perpetrator to help them feel more prepared.
It is likely that at some point in time a child or young person will disclose information to a parent who is a perpetrator. This disclosure may change the level of risk if the perpetrator uses that information to further perpetrate violence. In these circumstances the risk assessment should be reviewed and risk management and safety plans be updated.
Practice tip: You should develop risk management and safety plans with the presumption that at some point in time the child or young person will disclose risk- relevant information to the perpetrator.
Ensure that the child or young person, and the adult victim survivor are prepared in this situation. This includes the child or young person being ready to tell their parent who is a victim survivor when this has happened or to let yourself or another safe adult know so that the risk can be appropriately managed.
4.9 Safety planning where an adolescent is using family violence
Safety planning if an adolescent is using family violence differs to planning in response to an adult perpetrator. This is because risk management for adolescents using family violence should always consider their age, developmental stage and individual circumstances, and include therapeutic responses, as required. This is particularly important if the adolescent is both using and experiencing family violence.
Safety planning with the adult victim survivor (usually the mother) will need to include discussion on the therapeutic and other needs of the adolescent and how safety can be enhanced for the whole family whilst also addressing these needs.
The adolescent’s safety plan is generally shared with the adult victim survivor, so they can support the adolescent to implement their safety plan. Permission is needed from the adolescent before this occurs.
Any safety plan undertaken with an adolescent using family violence should occur and be consistent with safety planning for other family members, including adult victim survivors (usually mothers) or children (usually siblings) who are the target of violence.
Where adolescents use family violence a safety plan for that adolescent may include:
-
List the contact numbers for support organisations they may be already linked with, including if targeted community services are being engaged and that they can call if they identify their ‘early warning’ signs for abuse and violence.
-
Reflect protective factors, discussed and incorporated from what the adolescent has shared with you. E.g. Practice calming exercises every morning.
-
Identify a safe place for the adolescent to go if they feel they may progress to using violence, and how to get there.
-
Identify a friend, family member or neighbour who can assist and how to contact them.
Safety planning for an adolescent using violence may involve strategies for the victim survivor to respond to the adolescent’s use of violence. This does not mean the adult victim survivor is responsible for the use of violence by the adolescent but does acknowledge their contribution to family safety.
You can seek secondary consultation on how to support parenting practices with parent/carers of adolescents using violence, to ensure they are supported to respond to the adolescent’s behaviours, including if there are other siblings in the home. These may include:
-
How to improve conflict management, how to respond to threats and how to protect other children or young people or family members.
-
Strategies to de-escalate the adolescent’s abusive behaviour. For example, by not ‘buying into’ arguments.
If an adolescent using violence has a cognitive or intellectual disability, a risk management plan may include supporting the adult victim survivor to access a service that can support them to learn and implement behaviour modification strategies.
If the victim survivor is a parent of an adolescent using violence, particularly if the adolescent is young and/or has a disability, it is often a less feasible option for a victim survivor to leave. Additional options include:
-
Exploring the possibility of respite for the adolescent (if they have a disability) to facilitate a ‘cool off’ time and provide an opportunity for an exploration of interventions the victim survivor can use to prevent and minimise the use of violence.
-
Exploring the possibility of the adolescent going to a youth refuge to ‘cool off’. The police or a youth support service may be able to assist.
-
Exploring with the victim survivor the triggers, if any, which may lead to the use of family violence and how to avoid ‘triggering’ the adolescent or making changes to parenting and communication. This does not mean telling the victim survivor to rescind their parenting role, but it can begin to explore the patterns of communication and relating between parent and adolescent that may support the use of violence.
4.10 Discussion about leaving or staying safe at home
Making a decision or beginning to plan to leave a relationship with a perpetrator is a high-risk time period for an escalation of, and/or change in violence, including increased risk of being killed or seriously harmed.
It is important to recognise that a victim survivor does not have control over the abuse they are experiencing from the perpetrator.
Some victim survivors face significant barriers to leaving violent relationships and remain at home or in a relationship out of legitimate fears about what might happen to them and their children if they leave. It is important not to blame the victim survivor for this decision, and to explore the barriers or reasons with them. Some common, often interrelated reasons include:
-
Fear of escalation of violence.
-
Self-esteem (which may be significantly diminished from violence, trauma and abuse, shame at failure of relationship and guilt or self-blame about the abuse experienced).
-
Housing security, access to money/ financial security.
-
Keeping the family unit together (this may be internal and/or external pressure) — or have caring responsibilities for the person using violence (such as an adolescent).
-
Belief and hope that the perpetrator will change.
-
Isolation (family and support networks).
-
Lack of transport and means of communication.
-
Cultural and social expectations.
-
Concerns about what will happen to the perpetrator.
If a victim survivor has expressed a desire to stay in the relationship or family home, explore some of these reasons. If the reasons are based on barriers to leaving, you can ask whether they would like support to overcome these barriers.
If the person is not ready to leave a relationship and/or planning to leave may take time, you can explore options for them to remain more safely in the home. These include action in the safety plan (outlined above), and may also include:
-
Being ready to call police on ‘000’ and/or crisis specialist family violence services.
-
If the victim survivor feels the situation is escalating which might lead to violence, try moving to a space that is lower risk — avoid bathrooms, garages, kitchens, or other locations where there are objects or weapons available, or spaces where violence has previously occurred.
-
Plan possible escape routes from every room in the house, practice escapes and have window and door keys readily available.
-
Talk to the children about what is happening and encourage them to call for help and not intervene if violence occurs. Emergency numbers may be programmed into the phone or an older child or young person’s phone. They should never use a phone to call for help in front of the perpetrator as this may endanger them further. Make sure they know their safety plan actions if violence occurs.
-
Create code words or phrases for trusted friends or children so they know when to call for help and/or leave danger areas.
-
Choose a place to go — and let the children know where this is if you are separated. Let trusted friends/family know the safe place.
If they have decided that leaving is the best option, advise them that you or a specialist family violence service can help make plans to leave for a safe place. You should discuss whether it is safe to tell the perpetrator that they are leaving. If it is not, discuss when might be a safe time to leave. For example, when the perpetrator is not at the family home, at work, or away, or when the victim survivor has to leave the family home for a reason perceived as ‘legitimate’ by the perpetrator, such as picking the children up from school, going to a medical appointment, or going to work.
4.11 Talking to adult victim survivors about their options
Assist the victim survivor to identify and consider their options for support in a collaborative manner. Risk management and safety planning should be person-centred and victim-led, supporting each plan’s feasibility, safety and implementation (see Foundation Knowledge Guide Section 9.3).
Often, improving broader wellbeing or responding to needs, such as responding to the impact of a perpetrator’s behaviours, can improve effectiveness of risk management and safety plans, and support stabilisation and recovery from violence. These elements are reflected in the protective factors outlined in Responsibility 3, and the safety planning template at Appendix 9.
If making referrals, explore barriers to utilising referrals. Barriers will be different for each victim survivor and may be based on:
-
Their personal goals or interests and those of their children (for example, housing security, connection to community, culture, identity, family and friends).
-
Their experience of services in the past or experiences of structural inequality or discrimination (for example, poor engagement or response from services).
Many victim survivors may not feel ready to accept a referral, but by talking about barriers and options, you will have let them know that there is assistance available. You may also be able to reduce or remove barriers by facilitating warm/active referral and information sharing to limit a victim survivor having to retell their story. This is further outlined in Responsibility 5 and 6.
You could discuss:
What actions they have taken in the past to keep themselves safe
- How they have demonstrated resilience or strength — “Are there things you have done in the past that you think helped keep you (and your children) safe?”
Barriers to service access
-
Ask if they have experienced discrimination or poor service response in the past. Do they identify as Aboriginal or belonging to a diverse community? (See Foundation Knowledge GuideSection 9.4 and 9.5). Consider if there are ways you can reassure the person about these barriers and experiences and respectfully acknowledge their identity and circumstances while doing do (see Responsibility 1)
-
Ask “Is there anything I can do to make the referral or connection to a service successful?” For example, for victim survivors who identify as gender non- conforming or transgender, you might want to ask if conveying this information with the next service could assist them in providing a safe environment. Other examples could include asking about communication and/or access supports for victim survivors with a disability or interpreters for culturally and linguistically diverse victim survivors
-
You can also seek secondary consultation rather than referral if working together with another service can support engagement and consistent support (see Responsibilities 5 and 6)
-
Victim survivors experiencing elder abuse or family violence from adolescents may hold concerns about what will happen to the person using violence (often their child). This can be a significant barrier to the victim survivor leaving or excluding the person from the home. These concerns should be explored with the victim survivor.
Current needs
- Reflect on the domains of protective factors to guide conversation around wellbeing and needs. These may be personal or practical around housing, transport, communication, etc
- What issues are most important to them right now, e.g. “What would help most to support you?”
Informal social support
- Explore social supports available, e.g. “Have you talked to anybody about the family violence? Who do you feel you can trust? Do you have a family member, friend or trusted person in the community that you could talk to?”
Formal supports
-
“Have you had any previous involvement from services?” “What was your experience?”
-
“Are you currently or would you like to receive support from a service provider who specialises in [...]” (targeted community support, family violence, counselling or financial support, housing, or other support service outlined further below)
-
If so, then they could be encouraged and supported to contact that service using a ‘warm referral’ process.
Legal needs
-
“Are you currently engaged with any legal services?” “Do you want advice about [...]?” (financial entitlements if they leave the relationship, parenting arrangements for children, child support, property division, separation or divorce etc)
-
“Are there any family violence intervention orders in place?” “What are the conditions of the order/s?” “If so, has the order been breached?”
-
Are there any ‘red flags’ around legal issues, for example:
-
“Has a crime been committed? Such as criminal damage?”
-
“Has anyone been charged with a crime?” (Note, some victim survivors may have criminal charges)
-
“Has the person made any threats to remove/limit access to children or leave the country?” (Consider checking who has access to children’s passports)
-
“Have any fines/infringements been incurred? If yes, has it been wrongly assigned to you?” Relief may be available even if the fine/infringement was made against a victim survivor if it is linked to their experience of family violence. Relief is also available to re- assign fines and infringements which were caused by the perpetrator’s behaviour. Consideration should be given where the perpetrator incurs fines that the victim survivor pays.
-
Practice tip: If you aren’t sure about how current legal processes work, you can contact a specialist family violence service or a legal service for assistance to understand options and how to manage risks.
Mental health needs
- “Some people experience impacts on their mental health from the violence. Is this something you’ve experienced? Would you like assistance with this?”
Parenting needs
- “It sounds like you have done a lot to keep yourself and your children safe. Even with these efforts, sometimes a perpetrator will undermine the relationship between a parent and children, or your parenting skills and abilities. Would you like assistance in strengthening your relationship with your children?”
Service supports for children and young people
- “Children and young people are often impacted by family violence in invisible or less well-recognised ways. Are there actions we can take together to support the child/young person?”
- Check in on children and young people’s health and wellbeing needs: “What things does the child/young person enjoy doing? Are they still able to do these activities? Do they get to see friends and family? Do they have another trusted adult? Do they have any immediate health needs?”
- “Do the children have any disability support needs I should be aware of when safety planning or connecting you to services?”
4.11.1 Information sharing
This is further outlined in Responsibility 6.
You should ask the victim survivor if they have any concerns about information being shared with individual professionals or services, or if there is information they are concerned will increase their risk if the source is known to the perpetrator. These concerns should be responded to and detailed in the safety and risk management plan. Recording this in each plan will ensure you and the victim survivor have a shared understanding of how their information is shared, or protected, as required in the circumstances.
4.11.2 Connection to relevant services
Guidance on making referrals and seeking secondary consultation is in Responsibility 5.
Guidance on information sharing is outlined in Responsibility 6, and the Family Violence or Child Information Sharing Guidelines.
-
Making connections for the victim survivor to relevant services involves:
-
Sharing information with other service providers engaged with the victim survivor (adult, child or young person) as authorised, such as under the Family Violence Information Sharing Scheme, Child Information Sharing Scheme or privacy law
-
Referral or coordinated risk assessment and management responses with specialist family violence services, such as for housing relocation for the victim survivor, or other available services, or the victim survivor’s personal support networks (as required)
-
Referring to support services to address co-occurring issues related to wellbeing and needs, such as drug and alcohol problems, mental health concerns, legal needs and housing/homelessness, as required.
When working directly with children and young people, keep in mind that most services require parental permission to engage with children and young people under the age of 18.
4.12 Responding to serious and immediate risk
If you or any other professional or service identifies a victim survivor at serious and imminent threat of harm from family violence, you or they should immediately:
-
Notify Victoria Police.
-
Contact the local specialist family violence services, based on the victim survivor’s current place of residence.
In cases of ‘serious risk and requires immediate protection’, the specialist service will respond to provide comprehensive risk management, often in coordination with Victoria Police and other justice responses.
If these responses are not successful, they may require a coordinated response by a referral to a Risk Assessment and Management Panel (RAMP). A RAMP is a formally convened meeting, held at a local level, of key agencies and organisations that increases the collective capacity and effectiveness of the service system to identify and respond to perpetrators that pose a serious risk, and to hold them responsible and accountable for their violence.
This contributes to the safety of adults and children at serious risk and allows a response with direct interventions to immediate threats from family violence.
4.13 Documenting evidence of family violence
Documenting evidence of family violence is an important way to support applications for intervention orders and breaches or other justice or civil processes. You should only suggest this if the victim survivor can do so in a safe way.
Documenting could increase risk if discovered by a perpetrator. If the victim survivor is in the home with a perpetrator, you may explore keeping the documenting evidence in a safe place outside of the home.
If safe to do so, you can guide the victim survivor on documenting their experience of family violence. This might include:
-
Photographing injuries.
-
Medical evidence (including of sexual assault by specialist services).
-
Evidence of financial abuse.
-
Recording or writing down what was said or done, including details on time, location and specific details including any witnesses.
-
Noting breaches of orders, such as communication or exclusion orders.
-
Evidence of stalking, including through apps and technology, telephone or in-person (or from a third party on the perpetrator’s behalf).
-
Noting evidence of behaviours that led to harm of children or impact of that harm on children.
Records that you keep as part of your work practices, such as case notes and emails, can also be important sources of documentation that can support victim survivors. This is also important in keeping the perpetrator in view and ensuring their behaviour and impact is visible in case notes. For example:
Client presents as homeless; she has had to move three times in the past year due to ex-partner’s repeated attempts to locate her in breach of existing intervention order.
4.14 Ongoing risk assessment and management
Guidance on collaborative ongoing risk assessment and management is outlined in Responsibility 10.
Each risk assessment is a point-in-time analysis of the present risk, which is based on information known at the time from current and past behaviours of the perpetrator.
Risk management includes ongoing/ repeated risk assessment to identify if family violence risk has changed or escalated. Updates to risk management strategies and safety plans may be required where there are changes or escalation to the level and presentation of risk behaviours.
All professionals can support monitoring the safety of victim survivors through regular checking in, asking about changes in circumstances or experience of violence, observing changes in behaviour, or considering a review of assessment information that has been received from other sources/services that (may) affect risk.
If your service is child-focused, make sure to check in regularly with the child and any staff who have regular contact with them, and pay attention to any changes in behaviour that may indicate a change in risk. Refer to Responsibility 2, Appendix 1 and Section 10.3 of the Foundation Knowledge Guide for more information about the impacts of family violence on children.
If you or other professionals or services have contact with the perpetrator, you can seek information to monitor the actions and behaviour of the perpetrator to inform your understanding on the level of risk. You can also ask the victim survivor through your ongoing communication and service engagement about any changes or escalation in violence and support them to report breaches of any intervention orders or parenting orders to police.
Support can also be provided through contact and sharing information with the police and agencies and organisations involved in supporting the victim survivor.
4.14.1 Monitor safety, and the completion of actions against plans
It is important that organisations share relevant information about the perpetrator’s actions, behaviour and circumstances and the experience and circumstances of a victim survivor (including children). This information will be used to update risk management and safety plans, and to further share this information with other relevant services, such as specialist family violence services. This is especially important when the level of risk has changed or escalated, such as change in frequency or severity of violence.
Each professional or service which has an action assigned to them should make the best efforts to complete that action and let a coordinating service know when they have done so.
4.15 What's next?
You may seek advice and information from specialist family violence services to develop risk management and safety plans with victim survivors. After hours, professionals may contact 24-hours specialist family violence services for information and advice. To identify local family violence services you can refer to The Lookout(opens in a new window) website, or contact 1800RESPECT (1800 737 732).
In some circumstances, it is appropriate to seek secondary consultation or referral to a specialist family violence service for comprehensive risk management. Secondary consultation or referral:
- Must occur if the assessed level of risk is ‘serious risk’ or ‘requires immediate protection.’
- May occur if the assessed level of risk is ‘elevated risk.'
You may still have a role if a comprehensive risk management and safety plan is developed by a specialist service. This may include implementing actions, monitoring of safety and information sharing.
Guidance on:
- Making referrals and seeking secondary consultation is outlined in Responsibility 5.
- Information sharing is outlined in Responsibility 6.
- Collaborative ongoing risk assessment and management is outlined in Responsibility 10.
4.15.1 Document in your organisation’s record management system
It is important that you document the following information in your service or organisation’s record management system:
- All risk management and safety plans you develop for each adult and child victim survivor.
- Case notes and any other relevant information about the victim survivor or perpetrator’s circumstances.
- Any reports to police or statutory authorities you have made responding to serious and immediate risk, or if you have a significant concern for a child and young person.
- Any referral and secondary consultation actions you undertake.
- Any information you share with other services or professionals.
- Any risk management actions assigned to you or other professionals.
1. See State of Victoria, 2018, Children, youth and families, Criminal offences to improve responses to sex abuse, available online.
2. In some situations, entirely separate plans for children and young people may be required.
3. Table information adapted from Ministry of Justice Canada, 2013, Safety Planning with Children and Youth: A Toolkit for Working with Children and Youth Exposed to Domestic Violence.
Responsibility 5: Secondary consultation and referral, including for comprehensive family violence assessment and management response
Responsibility 5 chapter of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
5. Secondary consultation and referral, including for comprehensive family violence assessment and management response
5.1 Overview
Guidance is included on referral and secondary consultation. These are key practice aspects for further risk assessment and management, and to respond to co-occurring issues related to wellbeing and needs.
Key capabilities
Professionals required to have knowledge of Responsibility 5 should be able to:
- Seek internal supervision through their service or organisation
- Consult with family violence specialists to collaborate on risk assessment and risk management for adult and child victim survivors and perpetrators
- Make active referrals for comprehensive specialist responses, if appropriate.
5.2 Purpose of secondary consultation and referral
Seeking secondary consultation and referral, including by sharing information, are essential aspects of Structured Professional Judgement.
These assist professionals to determine seriousness of risk, inform ongoing risk assessment and approaches to risk management and safety planning. Secondary consultation is also a key aspect of building a shared understanding of family violence and to develop system-wide consistent and collaborative practice (Pillar 2 of the MARAM Framework). Secondary consultation and referral necessarily involve a degree of information sharing.
Secondary consultation and referral involve you determining what response is required to respond to an individual’s risk, or to support their wellbeing or needs, and identifying appropriate services that can assist.
Secondary consultation can take place for a range of reasons, including using the skills and knowledge of specialist family violence services to help you gain a further understanding of family violence risk and possible referral options. Secondary consultation can also occur with mainstream and other specialist services that have expertise to address wide-ranging needs. This can include: providing practical or therapeutic support; working with Aboriginal people or people who identify as belonging to diverse communities; working with children and young people; and, working with older people.
Using secondary consultation can help professionals to build their own knowledge, establish working relationships across organisations, assist in applying an intersectional lens to Structured Professional Judgement (see Foundation Knowledge Guide Section 9.5), and to ensure assessment and management responses provided to victim survivors are culturally safe.
Secondary consultation may lead to referral, or you may refer someone directly as a result of your risk assessment or management planning.
To determine which is the appropriate course of action, you will need to identify:
- What risks, needs or wellbeing issues are present that require response?
- What are the priorities, such as responding to risk, and how do these interact with the co-occurring priorities relating to wellbeing and needs, including the victim survivor’s views?
- What actions or interventions (by whom, within what time-frame) would make a difference to an individual’s safety, wellbeing or needs?
- The extent to which your organisation can facilitate these directly and what is your role.
- Identifying which other professionals and or organisations might be responsible for providing resources, skills, or practice expertise to respond.
If you are unsure which is the appropriate course of action for your role, you may wish to seek advice from your team leader or a senior practitioner to support you to determine which other professionals or services you could engage with in the circumstances.
Responding to risk, wellbeing and needs can support safety and promote stabilisation and recovery from family violence. Risk assessment and management (such as safety planning, secondary consultation and referral) will enable you to identify and address a range of risks, and related wellbeing and needs for victim survivors. Secondary consultation or referral may involve a range of services, such as specialist family violence services, Victoria Police, Child Protection, Child FIRST, or other advocacy, universal and general professional or therapeutic services.
There are a range of reasons for secondary consultation or referral. You should consider seeking secondary consultation with:
- Specialist family violence services to establish the presence or analyse the level of risk, such as where there is uncertainty based on the available information.
- Specialist family violence services where there is uncertainty about the identity of a perpetrator.
- Specialist family violence services on the development and/or actioning of risk management and safety plans and responses.
- Specialist family violence services with an expert knowledge of a specific diverse community and the responses required to address unique needs and barriers. Targeted services may also include community specific services, such as ethno-specific, LGBTIQ and disability services that focus on primary prevention or early intervention.
- Services that provide targeted culturally safe services or liaison support, such as a cultural safety advisor for victim survivors who identify as Aboriginal or belonging to a diverse community.
- Services that provide specialist support to children and young people.
- Services that provide specialist support to older people.
- Legal services.
- Any service or professional where their involvement in collaborative responses would benefit a victim survivor, such as co-case management arrangements.
You may seek to refer a victim survivor to:
- Victoria Police where a crime may have been committed.
- Child Protection or Child FIRST or other statutory services, as required.
- A specialist family violence service for a comprehensive risk assessment or management response, including consideration for a RAMP response.
- Other professionals with expertise or skill in supporting a victim survivor’s wellbeing or responding to identified needs.
Note, you should continue to work with the victim survivor following referral to understand if their level of risk changes or escalates, and seek secondary consultation as required, until the receiving service is successfully engaged.
5.2.1 You need to consider your legal permissions to share information for secondary consultation and referral
Secondary consultations should be considered in line with your authorisations to share information. Secondary consultation can occur without any identifying information being provided regarding the victim survivor (that is, providing de-identified information) to seek guidance on possible next steps.
If you think the secondary consultation may lead to a referral and require you to disclose relevant identifying or personal information, you must do so according to your legal permissions and responsibilities. In these circumstances, prior to undertaking the secondary consultation you should seek consent from an adult victim survivor, or the views of an adult, child or young person, if a child or young person is at risk of family violence.
Consent is not required to share information about a perpetrator as long as it is shared according to a relevant purpose under the Family Violence Information Sharing Scheme, or in accordance with another legislative authorisation. See Responsibility 6.
5.3 Responding to barriers
You should be mindful of barriers to service access that mean some victim survivors are less likely to follow up on a referral, particularly if they are not actively supported to connect to the next service (see Foundation Knowledge Guide). You should also be mindful of the effects of trauma, which may have significantly affected a person’s manner of relating to the world, their sense of autonomy and their capacity to actively engage with the receiving and other services (see Foundation Knowledge Guide Section 9.6)
People who are Aboriginal or identify as belonging to a diverse community and older people might be less likely to engage with receiving services for a range of reasons, including:
- actual discrimination and negative treatment, or fear of discrimination from professionals and services, which could be based on recent and past experience(s)
- language barriers
- physical and communication access barriers
- a lack of trust in services.
You should actively respond to any barriers identified. This may include exploring alternative service options for referrals, or addressing any issues, such as information sharing with specific services where confidentiality has been raised as a concern by the victim survivor. This may be of particular concern for people who identify with smaller or isolated communities.
You should discuss with a victim survivor the purpose and options for proposed secondary consultation and referral. Ask if they have previously experienced barriers to accessing services, such as being provided inaccessible or unsafe services or experiencing discrimination. Exploring options can also ensure a victim survivor is aware of what support is available to them. This can dispel concerns about whether funding is available to support their referral options, and what other support they may be entitled, to assist them to recover and stabilise following family violence or meet other wellbeing needs.
Victim survivors should be offered choices where possible in being referred to an organisation that specialises in working with their community. Aboriginal victim survivors, or people who have family members who are Aboriginal, may choose to use an Aboriginal or mainstream organisation. People from culturally, linguistically and faith diverse communities and LGBTIQ communities may also choose to access a specialist organisation. If there is no specialist service in your local area, you can support a receiving service to connect with a specialist service by secondary consultation to continue to facilitate safe engagement and service delivery.
You should ask a victim survivor if they have particular support approaches, needs or information you can provide to the receiving service in advance to support safe service delivery. This may include, for example, asking a victim survivor who is transgender or gender diverse if they would like you to share information about gender identity and their pronouns to ensure these are respected by the receiving service. You can also contact a service that you propose to refer a victim survivor to in advance in order to ascertain their level of competency in providing culturally safe services and ask directly about capacity to respond safely for the victim survivor’s individual identity and experience needs.
It is important to consider whether secondary consultation or referrals may lead to disengagement of the victim survivor and think about how to facilitate referral in a more supportive way. Reflect on guidance in Responsibility 1 to support safe engagement.
5.4 Seeking secondary consultation and making referrals
5.4.1 Referring or reporting to Victoria Police, Child Protection or Child FIRST
Professionals may also be subject to specific professional responsibilities in their role, including to report crimes and refer victim survivors to Victoria Police for further investigation, assistance and intervention.
As outlined in previous chapters, any agency, organisation or professional that identifies a victim survivor is at serious risk, including if there is an identified serious threat (see Responsibility 3), should immediately notify Victoria Police. This is also required when a victim survivor is NOT otherwise willing to receive assistance. You should also consider what other risk management actions are required in each circumstance, such as safety planning if reporting to Victoria Police may result in escalation of risk from a perpetrator.
If a crime has been committed, and there is no immediate danger, you should discuss with the victim survivor if you can support them to report to Victoria Police, or if they would like you to make a referral on their behalf.
Professionals have a range of obligations to report matters to Child Protection or Child FIRST. If you believe a child or children are in need of protection or you have significant concerns for the wellbeing of a child/ren or unborn child (after their birth), you must follow your obligations to report to Child Protection or make a referral to Child FIRST, as applicable (further detailed in Responsibility 4).
5.4.2 Secondary consultation with specialist family violence services
The purpose of secondary consultation with specialist family violence services is to seek support in:
- Understanding the level of risk and intersectional needs.
- Determining actions in line with the assessed level of risk.
- Determining whether a referral is required for a specialist family violence response.
Secondary consultation may result in a specialist practitioner supporting and working collaboratively with you to undertake intermediate assessment and management, or with you referring a victim survivor to the specialist service for them to complete comprehensive risk assessment and management. Secondary consultation with specialist family violence services can also assist with:
- Support to engage effectively and safely with victim survivors.
- Building a shared understanding of family violence risk.
- Information sharing to understand level of risk for the victim survivor/s.
- Joint monitoring of family violence risk and the opportunity to explore or monitor escalation/changes in the risk level.
- Convening coordinated or collaborative risk assessment or management support, as outlined in Responsibility 9, such as multi-agency meetings.
- Active referrals when the level of risk has been assessed as elevated/serious risk.
If The Orange Door(opens in a new window) operates in your local area, this is often the best point of first contact for secondary consultation. Alternatively, you can identify your local specialist family violence service by searching The Lookout(opens in a new window) website.
5.4.3 Secondary consultation with mainstream, universal and other specialist services
A range of professionals may be able to assist in supporting a victim survivor’s engagement with you for family violence risk assessment or management, or to respond to other wellbeing issues or needs. This may include seeking information from a professional already engaged with a victim survivor or perpetrator to inform your risk assessment or management planning.
This may also relate to an individual’s circumstances, age or identity such as to assist in safe engagement or to address barriers, structural inequality or discrimination an individual may have experienced (see Foundation Knowledge Guide Section 9.4). Secondary consultation could also be to support:
- Collaborative risk assessment, risk management or co-case management.
- Culturally safe engagement with Aboriginal people or people from culturally and linguistically diverse communities.
- Engagement with people who identify as belonging to diverse communities such as people with disabilities, people from LGBTIQ communities and people experiencing mental health issues (see Foundation Knowledge Guide for detail and definitions for diverse communities).
- Engagement with children, and young or older people.
Professionals that can assist with secondary consultation might include professionals who have existing professional relationships with an individual. For example, advocacy, universal and general professional or therapeutic practitioners including but not limited to teachers, general practitioners, drug and alcohol workers, mental health professionals, social workers, maternal and child health nurses, and childcare workers.
5.4.4 Referral
Referral is the process of connecting victim survivors (adult or child/ren) to information or services that are outside your organisation’s practice area. This includes early intervention when family violence first occurs, to avoid or respond to escalation or crisis and additional harm, and to support stabilisation and recovery from family violence. Referral is an important part of the risk management process.
Where you have identified a victim survivor to be at ‘elevated’ or ‘serious risk’, you should refer them to specialist family violence services for comprehensive risk assessment and management. Making referrals can also lead to increased understanding of risk through sharing of relevant information — including perpetrator behaviour — that can be used for ongoing risk assessment, management and safety planning.
Specialist family violence services triage responses to referrals, with actions taken for higher risk cases as a priority. Where you have an ongoing service engagement with a victim survivor and you have referred them to a specialist family violence service, you should continue to engage with the victim survivor about their experience of risk, i.e. to monitor their level of risk, and provide support as needed.
Referrals can also support wellbeing or needs of an individual, or strengthen protective factors, such as housing, financial security, connection to professional advocacy or therapeutic services, responding to health, child developmental or social issues. Referrals are made to meet a range of service needs. For example, an older person experiencing family violence might need access to advice and support including legal advocacy or financial counselling to respond to the impact of family violence.
5.4.5 Enabling successful referral
Responding to a victim survivor’s risk, wellbeing or needs includes a discussion with them about their priorities, concerns or barriers to engagement with other services. Safety issues should be identified and any approach or options for referral should not compromise their safety. To assist successful referral, consider:
- The level of distress a victim survivor is experiencing, and their readiness (personal and circumstantial) to receive and take up the referral.
- Experiences of trauma for the victim survivor, which may affect their capacity to actively engage with a receiving service (see Foundation Knowledge Guide Section 9.6).
- What other support the victim survivor may need to ensure they can access the service (interpreters, transport, childcare, speaking to a new worker while you are present etc.).
- Identifying services the victim survivor is already engaged with (which may be done through the ecomap exercise, see Responsibility 8, Appendix 15), who may be re-engaged, brought into the support network or alternatives identified.
- Providing options and choice in services — you can provide information about a range of options and services, recommendations and let the victim survivor decide which services they want to use.
- Providing support and prioritisation of referral options for the victim survivor responding to the level of risk, fear, safety and needs.
- Complete referral forms together with the victim survivor where appropriate
- Gaining consent/views (in accordance with the Child and Family Violence Information Sharing Scheme).
Sharing Scheme authorisations and privacy laws) to follow up with the referral to the organisation as required (e.g. your risk assessment of the child/ren may be dependent on the adult’s engagement with other parts of the service system, such as a drug and alcohol organisation or child and family services)
- Contact the agency receiving the referral to:
- Ensure it is appropriate
- Ascertain any waiting times
- Advocate for your client to receive service
- Provide relevant information to ensure the receiving service can meaningfully connect with the victim survivor
- Discuss roles and responsibilities
- Develop a case management protocol, if appropriate
- Managing expectations of the victim survivor regarding the options available and support they can expect to receive from each service, as well as maintaining contact during waiting periods.
- Sharing relevant information with other professionals and services to ensure safety and minimising the need for the victim survivor to repeat information they have previously disclosed (any risk assessments undertaken should form part of the referral).
- Where possible engaging the support of a case management service
- Checking information with the victim survivor that you intend to share with the receiving service to ensure it is accurate.
- Follow up with the victim survivor for feedback about the referral to ensure it was effective. Follow up can continue to support the engagement and ensure any issues that arise are addressed, and reduce likelihood of a victim survivor disengaging.
- Feedback processes with the receiving service or professional to support or respond to any engagement issues that may arise and to prevent disengagement.
Referral processes can occur by telephone, in face-to-face settings, by written communication (including e-mail), or a combination of these channels. A referral may combine aspects of each of these processes. For example, referrals may be warm/active or facilitated and informal (information only). Considerations in choosing which process to make a referral may include the victim survivor’s:
- Interpersonal style and ability to negotiate complex social interactions.
- Views on the proposed service options, including whether a specialist community service or mainstream service is preferred by the victim survivor
- Past experiences of trauma and disengagement due to structural inequality, barriers or discrimination which may need to be actively addressed
- Ability to provide and receive information (consider if this is relating to communication barriers or emotional or physical health, wellbeing, or permanent or situational factors).
- Ability to tolerate delays in service responses.
Table 1: Processes for making a referral
|
Informal referral (information provision) |
Provide verbal or written information about other services. Do not assume that the person will follow up on the information and make contact. If this type of referral is made, you should check at a later appointment if they have made contact and, if not, explore the reasons why. There may be various reasons for not making contact with the service. If this has occurred, you may offer to provide warm or facilitated referral to overcome any barriers. |
|
Warm (or active) referral |
Actively connect the victim survivor to the receiving service (for example, making a phone call together to introduce and share information). This enables three-way dialogue that is open and transparent to clarify issues immediately and outline the purposes and goals for the referral to the new service. |
|
Facilitated referral |
Provide relevant information to another professional or service (verbally or in writing). Make arrangements for the person to attend, and/or go with them to the agency to assist in building trust and rapport with a new professional or service and facilitate culturally safe services. This includes sharing information that prevents a victim survivor from having to repeat their story. You may also consider asking the victim survivor if they would like you to prepare a letter or other communication for them to take to other services that provides foundational information to enable safe engagement, such as about medical or mental health issues, medication, communication assistance needs, identity characteristics and pronouns. |
A number of considerations apply when making referrals. The central objective of making referrals is to first address the family violence risks and safety for the victim survivor (adult and child) and then to connect to services to address their needs and wellbeing concerns. You should consider and work with the victim survivor to reduce or remove barriers to engaging with the service being referred to, which might include:
- Fear of escalation of risk from the perpetrator, including if they become aware of service interventions and information sharing.
- Impacts from experiences of trauma.
- Physical, practical and communication access barriers.
- Previous negative experiences of services and forms of structural inequality and discrimination the person may have experienced that have led to disengagement.
5.4.6 What information should be contained in a referral?
Work with the victim survivor on completing the referral forms or letter. Discuss with them the information you intend to share, and seek their consent, or their views, as required.
When referring to:
-
Specialist family violence services:
This will include the completed risk assessment and risk management and safety plans.
-
Other professionals and services:
Relevant information from risk assessments or circumstances impacting risk, wellbeing or needs.
Consider including all relevant information for the purpose of the engagement, as well as information that will support safe engagement, such as information about the level of risk, a person’s identity, experience, wellbeing or other needs
You may also share information related to addressing barriers to service engagement previously experienced, age and developmental stage (if referring a child or young person), or any other barriers to actively address in the new service engagement.
See Responsibility 6 for information on determining what is relevant to be shared through information sharing.
5.4.7 Which organisations might referrals be made to?
Referral pathways may need to be wide- ranging but staged to accommodate the needs of each adult and child victim survivor. In the first instance, referrals should be focused on addressing any immediate risk, fear or safety. Referrals could include:
- Supporting a victim survivor to report to police, or referral to specialist family violence services, including for a RAMP response
- Child Protection or Child FIRST, where you identify serious concern for a child or young person, or as required under any mandatory reporting obligations, or there are other wellbeing concerns identified
- Referral to a legal service or to a court if the victim survivor wants to apply for an intervention order, or to seek legal advice
- Referral to a targeted specialist community service, such as services specialised in supporting Aboriginal people or people from diverse communities, or children, young or older people
- Universal or mainstream professional supports, including advocacy or therapeutic responses to provide supports for wellbeing or needs, or to promote or strengthen protective factors.
5.4.8 Good referral practices between professionals and services
Good referral practice needs services and organisations to embed, support and enable this practice through relevant policies, procedures and other guidance and resources. This can include:
- Maintaining a list of professionals or services that you or your organisation has good working relationships with or MoUs, and their roles and responsibilities, with the names of key people who might be of assistance
- Understanding eligibility and the intake processes of other services and organisations
- Establishing an understanding between services/organisations, documented in a Memorandum of Understanding or a referral protocol or pathways
- Developing and using referral forms that include agreed information, minimising the need to ask the same questions
- Providing advocacy support for victim survivors who require assistance accessing services
- Reviewing referral processes with other agencies to identify improvements
- Linking with Regional Integration Coordinators and Principal Strategic Advisors to understand local governance and strengthen networks between mainstream, universal and specialist family violence services.
5.5 Consent or views on secondary consultation and referrals
The purpose and requirements of the Family Violence Information Sharing Scheme are outlined in Responsibility 6, including seeking the victim survivor’s consent or views on information sharing and consent requirements.
Where identifying information is going to be shared, victim survivors should be involved in making decisions about referral and secondary consultation wherever possible. You should outline and clearly explain the service referral options and purposes for secondary consultation.
Ideally, victim survivors will consent to you sharing information with another person or service as part of making a report to Victoria Police, Child Protection, or a referral to another service provider. However, if they do not consent, the FVIS Scheme permits information sharing without consent in certain situations where relevant thresholds are met:
- A person experiencing family violence should be informed that you are able to share information about risk to children without consent, but that you will always let them know when this is going to occur, if safe, appropriate or reasonable.
- If sharing without consent, you must seek their views, if safe and reasonable to do so. Seeking views can inform how information is requested and from what professionals or services, and may inform you on how to do this safely.
For further information on information sharing for referrals, including where information can be shared without consent, refer to the Family Violence Information Sharing Guidelines.
5.6 Record keeping and referrals
You should make file records of information you share with other professionals and services, and details of referrals. You should also keep records of consent or views to information sharing and referrals, as required under the Family Violence and Child Information Sharing Schemes and other legal authorisations and privacy laws.
Further information on record keeping is outlined in Chapter 10 of the Family Violence Information Sharing Guidelines(opens in a new window), and Chapter 5 of the Child Information Sharing Scheme Guidelines(opens in a new window).
Responsibility 6: Contribute to information sharing with other services (as authorised by legislation)
Responsibility 6 chapter of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
6. Contribute to information sharing with other services (as authorised by legislation)
6.1 Overview
The guidance in this chapter is intended to be general as each individual victim survivor’s level of risk, circumstances, wellbeing and needs will require a unique response and will build on the outcome of risk identification, assessment or management (undertaken, or planned).
In situations involving children experiencing family violence, professionals can use the Family Violence Information Sharing Scheme to request and share information in order to assess and manage family violence risk, as well as the Child Information Sharing Scheme for broader safety and wellbeing issues.
Key capabilities
Professionals required to have knowledge of Responsibility 6 should be able to:
- Proactively share information relevant to the assessment and management of family violence risk, including under the Family Violence Information Sharing Scheme, privacy law or other authorisation at law.
- Proactively share information relevant to broader safety and wellbeing issues for children using the Child Information Sharing Scheme.
- Respond to requests to share information from other services.
The outcome of risk identification (Responsibility 2), assessment (Responsibility 3 or 7) or management (Responsibility 4 or 8), will inform the kinds of secondary consultation, referral or information sharing you should undertake.
Guidance which refers to a perpetrator in this guide is relevant to situations where an adolescent is using family violence.
Remember
Professionals and services are authorised to share information to inform risk assessment or management practice under a range of laws, including the Family Violence Information Sharing Scheme, the Child Information Sharing Scheme, the Children, Youth and Families Act 2005 and relevant Australian privacy laws. The guidance in this chapter will focus primarily on using the Family Violence Information Sharing Scheme and the Child Information Sharing Scheme where family violence risk is present.
Organisations should assist professionals and services to understand and apply these Schemes and other authorisations to share information applicable to their service.
6.2 Purpose of information sharing
Effective information sharing is crucial in keeping victim survivors safe and holding perpetrators to account.
Information can also be shared to promote the broader wellbeing and safety of children, which may or may not relate to their experience of family violence.
The Family Violence and Child Information Sharing Schemes aim to create a significant cultural shift in information sharing practice. These schemes are also underpinned by the MARAM Framework, as well as relevant best interests and developmental frameworks. Professionals in prescribed organisations all have a role in information sharing to improve risk assessment and management practice.
Many organisations, especially those with ongoing service engagement with perpetrators or victim survivors, hold information relevant to assessing and managing family violence risk or to promote the safety or wellbeing of a child.
Effective information sharing between professionals supports risk assessment and management by bringing together information that would otherwise be unknown. This information can be used by relevant professionals to remove or reduce risk (as far as possible) or prevent escalation.
Risk is dynamic and can change over time. Professionals with responsibility for ongoing risk assessment should continue to share information to support updating of risk management and safety plans for the victim survivor, as well as intervention action planning for perpetrators of violence. This is particularly important for victim survivors who are not directly engaged with specialist family violence services in an ongoing way, but only at points of crisis or escalation.
Information sharing often means victim survivors don’t have to repeat their story with each new service they engage with. It also enables new services to build on existing information.
6.3 Information sharing in structured professional judgement
Information sharing is a key enabler of the model of Structured Professional Judgement as it supports professionals to share information to inform risk assessment. Information sharing may be authorised under a range of laws such as the Family Violence Information Sharing Scheme, the Child Information Sharing Scheme, the Children, Youth and Families Act 2005 or other relevant Australian privacy laws.
Figure 1: Model of Structured Professional Judgement
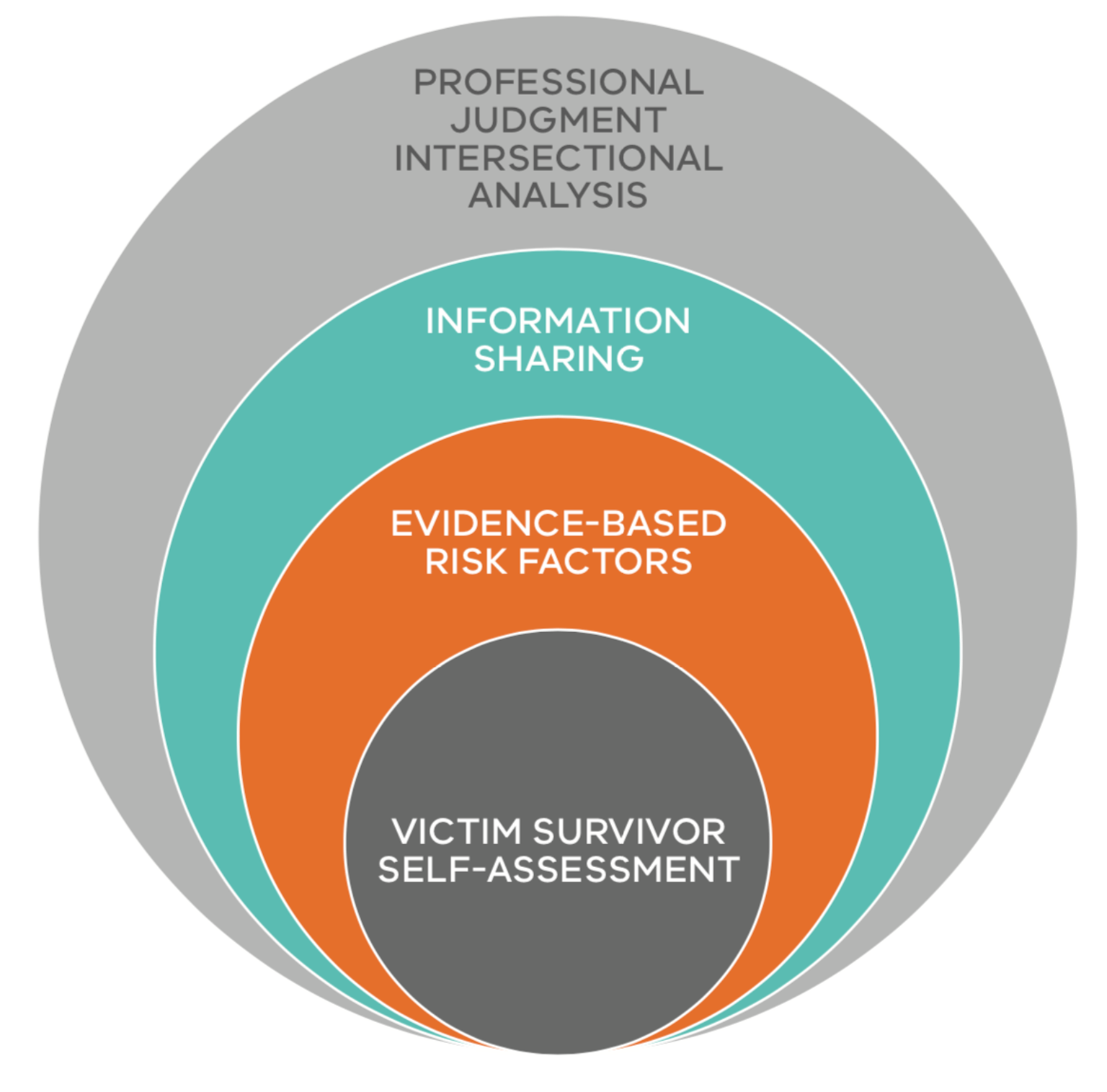
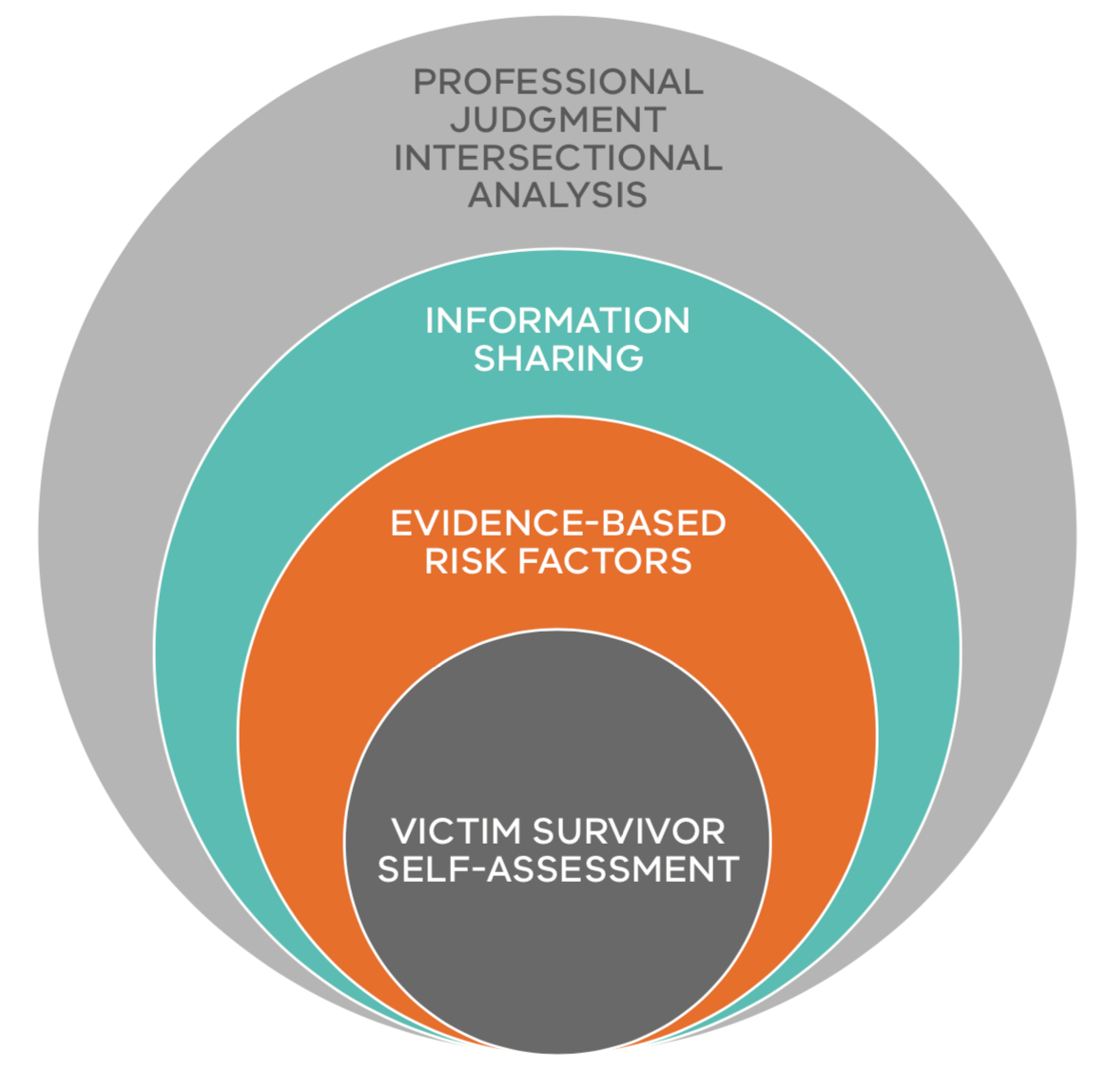{kind=link}
Sharing information assists professionals to identify additional risk factors or provide more information about known risk factors. This information can crucially inform the assessment of the level or seriousness of risk, and implementation of risk management responses as well as to promote the safety and wellbeing of children. Consider information sharing in each risk assessment you undertake, where services or engagement points are identified that may have information that would assist in the assessment or management process.
Key sources of information can be identified through consideration of protective factors or by using the genogram or ecomap exercises outlined in Responsibilities 7 and 8.
When assessing or managing risk to a victim survivor, consider how you might request and share information and ensure consent thresholds are met, where applicable. If consent for information sharing is not required, ensure that you take into account a victim survivor’s views if appropriate, safe and reasonable, particularly in relation to any past or recent experiences of service barriers or discrimination.
A victim survivor’s views expressed regarding information sharing should inform:
- Your approach to the information you request or share voluntarily.
- The professionals or services you are sharing information with voluntarily.
- How you might share information in response to a request.
Information sharing with other professionals and services should be used in conjunction with information gained from a victim survivor, including their self-assessment of risk, information about risk factors present and related circumstances, needs or wellbeing issues, that have been identified through risk assessment.
6.4 Reflecting on safe engagement, including for information sharing practice
Each victim survivor, both adults and children, should be considered individually for the services or supports they may need. This may be the first time a victim survivor has had their family violence risk, wellbeing or needs assessed, or they may have previously been connected to services. You should enquire about this to identify if there are any barriers to connection, or opportunities to reconnect to supportive services (see also Responsibility 4).
You should discuss options with victim survivors on the approach to referrals, and secondary consultation, including ongoing assessment and management. This will include your approach to prioritise and coordinate connection and referral to services. Prioritisation will be informed by your determination of the seriousness of risk, if you are responding to a crisis, and if connection to statutory service interventions are required. Responding to immediate risk is outlined in Responsibilities 2 and 4, and you may also use this guide to help you plan risk management responses and take action.
When seeking secondary consultation, making referrals or sharing information, you should be informed by an intersectional lens (See Foundation Knowledge Guide Section 9.4 and 9.5). In considering each service engagement, you should be guided by the individual’s identity and tailor your approach to referral, secondary consultation or information sharing accordingly. For example, if the victim survivor has let you know they are Aboriginal, identify as belonging to a diverse community, or are a child, young person or older person, consider if your service engagement would benefit from specialist advice or support.
Ask if the victim survivor would like to be directly connected to a service that specialises in working with individuals from their community group, or if they are comfortable with you sharing information with or connecting to that service for secondary consultation. The practice guide for Responsibility 1 will also assist with these aspects of practice.
Remember
Building and maintaining trust in the relationship with the victim survivor is essential to safe, ongoing engagement. It is particularly important to maintain trust and communication when connecting victim survivors to services and sharing information to promote their safety.
In most situations, referral does not mean you immediately cease your engagement with a victim survivor. Depending on your role, you will likely need to maintain engagement or continue to ‘check in’ with the victim survivor to support connection to a receiving service and respond to any issues that arise. This is also an important part of ongoing assessment and management of risk.
6.5 Legal authorisation to share relevant information
The Family Violence Information Sharing Scheme authorises organisations and services, prescribed through regulations, to share relevant information to assess and manage family violence risk.
Details of this scheme are outlined below and in the Ministerial Guidelines. Organisations may also have other permissions to share information to inform risk assessment and support coordinated and collaborative responses.
The Child Information Sharing (CIS) Scheme also allows organisations and services prescribed under that scheme to share information with each other to promote children’s wellbeing and safety1. This includes to promote the broader wellbeing and safety of children who experience family violence.
The CIS Scheme has been designed to complement the Family Violence Information Sharing Scheme. Refer to the guidelines for the CIS Scheme(opens in a new window) for further information.
Remember
If there is a serious threat to the life, health, safety or welfare of a person (such as serious risk of family violence), under the FVIS Scheme and privacy law you can share information, to lessen or prevent that threat without consent of any person. See the Office of Victorian Information Commissioner(opens in a new window) for further information.
As outlined in Responsibility 7, if serious risk has been identified through assessment via the MARAM Responsibilities for Practice Guide, this is considered to be an equivalent determination of ‘serious threat’ for the purposes of sharing information to lessen or prevent a serious threat under these Acts.
6.6 The family violence information sharing scheme
This section outlines key elements of the Family Violence Information Sharing Scheme (FVIS Scheme). Detailed guidance on the operation and use of the scheme are available in the Family Violence Information Sharing Guidelines.
Organisations and services that are prescribed under the FVIS Scheme are known as Information Sharing Entities (ISEs) and are authorised to share relevant information to assess and manage family violence risk2. The FVIS Scheme is intended to improve professionals’ and services’ ability to keep victim survivors safe and hold perpetrators in view and accountable for their actions and behaviours.
A subset of ISEs, known as Risk Assessment Entities (RAEs), have additional responsibilities to establish whether a risk of family violence is present, assess the level of risk posed and correctly identify the parties as the perpetrator or victim survivor through a comprehensive risk assessment.
A key component of the FVIS Scheme, is that information about an alleged perpetrator or perpetrator can be shared without their consent. Consent thresholds are further explained in Chapter 1 of the guidelines.
Some relevant sections of the guidelines are outlined below. However, you should refer to the guidelines for further information.
6.6.1 When can information be shared under the Family Violence Information Sharing Scheme?
There are two purposes for which ISEs can share information with each other under the FVIS Scheme:
- A family violence assessment purpose (to establish and assess risk):
The primary focus of a family violence assessment is on establishing whether a risk of family violence is present, assessing the level of risk the alleged perpetrator or perpetrator poses to the victim survivor, and correctly identifying the parties as the perpetrator or victim survivor.
- A family violence protection purpose (to manage the risk, including through ongoing risk assessment)
The family violence protection purpose means managing the risk of the perpetrator committing family violence, or the risk of the victim survivor being subjected to family violence. Information can be shared for this purpose when the presence of risk is known.
Managing risk involves removing, reducing or preventing the escalation of risk. As risk is dynamic and can change over time, information can be shared for ongoing risk assessment to monitor risk and escalation. For example, any ISE can request and share information from other ISEs to inform ongoing risk assessment and update risk management and safety plans with the victim survivor.
Remember
Any professional with a role in family violence risk assessment and management can undertake a risk assessment (in line with their role) under the MARAM Framework, such as screening, intermediate or comprehensive assessment. Information may be shared with all ISEs to undertake these functions to manage family violence risk.
Where it is not known whether family violence risk is present or the identity of a perpetrator is unknown or uncertain, then information may be shared with RAEs for an assessment purpose to establish risk or the identity of an alleged perpetrator.
If you have a reasonable belief that family violence risk is present and the identity of the perpetrator or victim survivor/s are clear (e.g. the victim survivor has identified the perpetrator), this would enable any ISE to share information under the FVIS Scheme for a protection purpose.
6.6.2 Talking about consent and information sharing with a victim survivor
In order to provide effective support to victim survivors it is crucial for you to build and maintain relationships of trust with them. An important way of achieving this is through open and transparent communication. This means making it clear that although you and your service will maintain confidentiality where possible, information sharing and other laws mean that relevant information may be shared without consent in some circumstances.
Chapter 9 of the Family Violence Information Sharing Scheme Guidelines provides information on the essential elements of consent, how consent can be given, how it should be documented and what to do when consent is refused or withdrawn.
Under the FVIS Scheme, various consent thresholds apply when information is being shared to assess or manage risk to adult and child victim survivors of family violence.
- Perpetrators and alleged perpetrators of family violence: Consent of an alleged perpetrator or perpetrator is not required when sharing their information under the FVIS Scheme (Chapter 3).
- Adult victim survivor: Consent is required to share information about an adult victim survivor (a person who is 18 years or over), unless the ISE reasonably believes that sharing confidential information is necessary to lessen or prevent a serious threat to an individual’s life, health, safety or welfare or the information relates to assessing or managing a risk to a child victim survivor (Chapter 4).
- Relevant third party: Consent is required to share information that identifies a relevant third party, unless the ISE reasonably believes that sharing confidential information is necessary to lessen or prevent a serious threat to an individual’s life, health, safety or welfare or the information relates to assessing or managing a risk to a child victim survivor (Chapter 4).
- Child victim survivors: Consent is not required from any person to share their information when you are assessing or managing risk for a child victim survivor (a child is someone who is under the age of 18 years, including infants and adolescents). However, where safe, appropriate and reasonable you should obtain the views of the child and/or other family members at risk of violence (including a parent who is not a perpetrator) prior to sharing their information (Chapter 5).
The Guidelines also provide information on having a conversation with an adult victim survivor about obtaining consent and limitations of consent (Appendix D) and a child victim survivor about their views and wishes (Appendix E) related to information sharing.
6.6.3 How can seeking consent or views inform your risk assessment or management planning?
Asking a victim survivor for their consent or views (as required) about what information is shared and the services you are sharing information with, can often assist you to understand more about the risk they are experiencing. This process can also highlight the barriers or discrimination a victim survivor may have experienced which may change the approach you take to secondary consultation or referral (see Foundation Knowledge Guide Section 9.4 and 9.5).
In situations where consent is not required (such as where there is a serious threat or if assessing risk to a child), you must seek the person’s views on what information is shared and the organisations or professionals you propose to share information with (noting that you are not required to seek consent or views from an alleged perpetrator or perpetrator to share their information).
A victim survivor’s views about information sharing can:
- Assist you to identify additional risk factors.
- Enable you to share information which would support culturally safe service from the receiving professional or service.
- Help you share information safely and mitigate future risk of unsafe information sharing by recording in safety plans any known issues with sharing to specific professionals or services.
Examples of where it may not be appropriate, safe or reasonable to seek views of a victim survivor are outlined in the Family Violence Information Sharing Scheme Guidelines(opens in a new window).
6.6.4 Information sharing under other laws
If you were already permitted to share certain information under existing privacy laws or another law before the Family Violence and Child Information Sharing Schemes commenced, you can continue to do so. The intersection of the FVIS Scheme and other laws is outlined in Chapter 11 of the Family Violence Information Sharing Guidelines.
6.7 Risk-relevant information
Understanding what information is ‘risk- relevant’ is central to family violence risk assessment and management practice. Also, information that is relevant for a family violence assessment or protection purpose can be shared under the FVIS Scheme.
Identifying what information is ‘relevant’ will:
- Be determined on a case-by-case basis for each victim survivor or perpetrator, depending on the family violence behaviours (risk factors) a perpetrator is using against a victim survivor, or each of their circumstances, or related wellbeing and needs to promote stabilisation and recovery.
- Be information that supports your assessment of current or future risk, which can include a perpetrator’s past behaviour. Information about a victim survivor’s past behaviour is less likely to be relevant.
- Depend on the purpose for which you are sharing the information, such as an assessment or protection purpose (see Section 6.6.1 of this guide and the Family Violence Information Sharing Scheme Guidelines for further information).
- Depend on your role and the role of the professional/service you are seeking information from or sharing information with.
- Depend on what action you want to take:
- Why are you seeking the information — how will this inform your family violence risk assessment or management role? (e.g. assessment or safety planning).
- What action do you want the receiving professional/service to take from your sharing the information?
Risk-relevant information may be information about a perpetrator (their behaviour or circumstances) or a victim survivor (the risk they are experiencing and their circumstances) or another person.
The information should be relevant to your decision-making for assessing or managing family violence risk, including stabilisation and recovery.
Information about perpetrator behaviour such as violence used against an adult or child, the presence of risk factors, or a perpetrator’s circumstances, are an important first point of reference for understanding what information is risk- relevant. Information that relates to any of the family violence risk factors is described in detail in the Foundation Knowledge Guide, and within the guidance on risk assessment in Responsibilities 3 and 7.
Relevant information may also relate to a victim survivor or perpetrator’s circumstances impacting risk management planning. These may include:
- Housing or employment of perpetrator (what is their location and whereabouts?).
- Health, mental health, or other wellbeing issues which influence behaviour, decisions or choices.
- Are there family law orders or intervention orders in place (e.g. exclusion conditions on intervention orders).
Some of these relevant circumstances may be identified through the risk assessment discussion with a victim survivor, or through consideration of the protective factors and safety planning. Further guidance on identifying relevant information about a perpetrator’s circumstances is outlined in Responsibility 7.
Risk management is defined broadly to include stabilisation and recovery, such as the impact of family violence on wellbeing and needs. Under the FVIS Scheme, this means risk-relevant information for a victim survivor, which includes information that relates to wellbeing and needs due to their experience of family violence.
Information relevant to promoting a child’s wellbeing or safety can also be shared under the CIS Scheme, including outside of the context of family violence. Information can be shared under the CIS Scheme if an ISE reasonably believes that sharing the information may assist another ISE to:
- Make a decision, an assessment or a plan relating to a child.
- Initiate or conduct an investigation relating to a child.
- Provide a service relating to a child.
- Manage any risk to a child.
Information may be sourced from:
- Disclosure and/or risk assessment with a victim survivor.
- Discussion from related third parties such as friends or family members.
- Victoria Police family violence incident information (your service may receive L17 referrals).
- Court records (that are not excluded).
- Other records from professional or therapeutic service and relevant databases.
The range of sources of direct disclosure will vary depending on your professional role. Other information can be requested through the schemes from other ISEs under the appropriate assessment or protection purpose, or other applicable authorisations.
If you are uncertain about what information is relevant to share, seek secondary consultation internally (within your organisation or service), or externally with a specialist family violence service. If you are concerned or unsure whether information is relevant, you can share information with a specialist family violence service through secondary consultation in a de-identified way.
Remember
You should be discerning about the information you are sharing. It is usually not appropriate to share ‘whole records’ without review of the content and scope of information contained within them, and you should be guided by the criterion above on the specific information that should be shared.
If working with the victim survivor you should seek their consent to share information, unless consent is not required, in which case you should seek their views, where appropriate, safe and reasonable to do so.
6.7.1 Sharing information relating to family violence risk for children and young people
Children should have their risk and related wellbeing and safety needs individually assessed as per guidance in Responsibility 3. Under the FVIS Scheme, information about any person that is relevant to assessing or managing family violence risk for a child can be shared by an ISE without the consent of that person.
However, where it is appropriate, safe and reasonable, you should seek the views of the child or young person, and a parent/carer who is not a perpetrator, on how their information is shared. These views should be taken into account when deciding what information should be shared, including what services you should voluntarily share this information with or how information might be shared when you are obliged to share. Where you have safety concerns about how, when and with whom information is shared, including where doing so may increase risk, this should be reflected in risk management and safety plans (see Responsibility 4).
You should make clear to parent/carers (generally mothers) that are not perpetrators, that if their information is shared despite their views, it is being shared to assess or manage risk to a child.
6.7.2 Method of information sharing
The FVIS and CIS Schemes do not dictate that information has to be shared in a specific way. It is common for information to be shared with another professional by a range of methods, including verbally (face-to-face), email and phone. This may depend on the policies of your organisation or the urgency of the request or sharing, and will often depend on whether there is an existing professional relationship or this is the first time you have made contact with a service or professional.
When the information sharing request is time critical, you can phone a professional or service in the first instance. You could then then choose to follow up by making the request or sharing the information in writing to enable you to document the request or sharing of information as part of your organisation's good record keeping processes. When sharing and storing information, organisations should follow their obligations for data security under privacy law, if applicable.
You should refer to your organisational policies on information sharing methods to guide you, including your authorisation to share under applicable information sharing laws and how to keep records of any information shared.
If you are uncertain, prior to sharing information, confirm by following your internal processes, such as consulting with a senior practitioner or team leader, or by secondary consultation, to determine if the information you are sharing is relevant to the purpose (for an assessment or protection purpose for the FVIS Scheme, or to promote the wellbeing of a child under the CIS Scheme). This will assist in the request process if the responding ISE raises questions about the relevance of information requested.
6.7.3 Collecting and recording information sharing
You should refer to your organisation or service’s policies and procedures on record keeping in relation to information sharing. The Family Violence and Child Information Sharing Schemes have specific record keeping requirements that are aligned.
The Family Violence Information Sharing Scheme Guidelines(opens in a new window) provide advice on what is required in Chapter 10.
The Child Information Sharing Scheme Guidelines also include information on record keeping and information management in Chapter 5.
As specified in the Ministerial Guidelines, ISEs should take reasonable steps to correct information recorded or shared about any person if an ISE becomes aware that the information is incorrect. This applies if the information is about a victim, perpetrator or third party.
Professionals should refer to their organisation’s policies and procedures to assist with correcting information. Inaccurate information should be corrected as soon as possible after you become aware the information is inaccurate and you should give prominence to any correction on the client’s file. This is particularly important if the information may put a victim survivor at risk or a victim survivor has been or may be misidentified as a perpetrator.
6.8 What's next?
Information sharing can continue to inform your actions for risk assessment and practice, depending on your role, under Responsibilities 3–4, or 7–8.
In some situations, it may be necessary to convene a coordinated response to family violence risk, or safety and wellbeing for children. If this is the case, refer to Responsibility 9 for further information.
Ongoing risk assessment and management is also a part of practice. You should regularly review the appropriateness of referrals and follow up with services on the success of the referral and how you can continue sharing information to inform your risk assessment or management approaches. For more information about ongoing risk management practice, refer to Responsibility 10.
6.8.1 Document in your organisation’s record management system
In addition to Section 5.6, it is important to document the following information in your service or organisation’s record management system:
- Copy of any risk assessment or safety plan you share with other services.
- Under what permission you requested or shared information e.g. Family Violence Information Sharing Scheme, Mandatory Reporting, other privacy law.
- What organisation or service was contacted for secondary consultation and who you spoke with.
- Method of request (email, fax, telephone).
- What information was requested, the date of request.
- If and what information was shared, the date, who the information was shared to.
- If a referral was made — to who and the purpose.
- Views of the victim survivor around secondary consultation.
- Outcomes of secondary consultation and referral.
1. Part 6A, Child Wellbeing and Safety Act 2005.
2. Part 5A of the Family Violence Protection Act 2008 (the Act). This information sharing scheme was introduced pursuant to recommendation 5 of the Royal Commission into Family Violence, which acknowledged that organisations that work with victims and perpetrators of family violence collect a wide variety of information in order to keep victims safe and hold perpetrators to account. The Commission also identified barriers that prevent information from being shared as effectively as it could be and found that the failure to share crucial information with frontline workers can have catastrophic consequences.
Responsibility 7: Comprehensive Risk Assessment
Responsibility 7 chapter of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
Appendix 11 contains the Comprehensive Assessment Tool as a stand-alone template.
Appendix 12 contains a genogram template and guidance on how to develop a genogram.
Appendix 13 contains the questions from the Comprehensive Assessment Tool with a table of practice guidance about each question, including questions for people who identify as Aboriginal or belonging to a diverse community.
7 Comprehensive risk assessment
7.1 Overview
This chapter should be used to guide comprehensive risk assessment of family violence.
This may be following a referral of a victim survivor who has been identified and assessed by another service, receipt of a referral from Victoria Police (known as an L17) or following direct contact and disclosure from a victim survivor.
Key capabilities
Professionals required to have knowledge of Responsibility 7, should be able to:
- Understand and apply all guidance on each of the previous responsibilities.
- Comprehensively assess the family violence risks, needs and protective factors for victim survivors (adults, children and young people).
This chapter uses all elements of the process of Structured Professional Judgement and applies an intersectional analysis to inform the assessment, building on the guidance in the Foundation Knowledge Guide and Responsibilities 1–3. A comprehensive risk assessment builds on questions about evidence-based risk factors in the intermediate risk assessment, with additional questions relating to:
- Presentation of risk factors for people who are Aboriginal or identify as belonging to a diverse community or at- risk age group (for example, older people).
- Experience of risk for children and young people.
See the Table 5, Section 7.5 for information on the structure of the tools.
This guide will enable you to:
- Form a professional judgement on the level or ‘seriousness’ of risk.
- Provide you with a comprehensive understanding of the experience and presentation of risk for the victim survivor, as well as an understanding of the protective factors.
- Understand the circumstances of both the victim survivor and perpetrator that can cause change or escalation of risk from the perpetrator.
Guidance on undertaking comprehensive assessment to determine risk for children and young people is in Section 7.7 of this chapter.
Remember
Guidance which refers to a perpetrator in this guide is relevant if an adolescent is using family violence for the purposes of risk assessment with a victim survivor about their experience and the impact of violence. Risk assessment and management for adolescents should always consider their age, developmental stage and individual circumstances, and include therapeutic responses, as required.
This guide also includes practice approaches where misidentification of the victim survivor and perpetrator may have occurred. This is further discussed in Section 7.15.
7.1.1 Who should undertake comprehensive risk assessment?
Comprehensive risk assessment is undertaken only by professionals with a specialist level of skill, knowledge and expertise in family violence practice. Specialist family violence practitioners provide services for family violence intervention with all or the majority of their work directly focused on family violence risk assessment and management practice.
For further information please refer to your organisation’s family violence policies and procedures and the MARAM Organisational embedding guide.
Remember
Generally comprehensive risk assessment and management by specialist family violence practitioners will be undertaken as part of a case management framework that includes engagement, risk and needs assessment, safety and action planning, intervention/implementation of plans, monitoring and coordination and review/ case closure.
7.2 Structured professional judgement in comprehensive risk assessment
Structured Professional Judgement is the practice approach model that underpins the comprehensive risk assessment to support you to determine the current level of risk, history and pattern of violence, and inform risk management and intervention (see Responsibility 8).
Comprehensive assessment is the direct asking of questions about evidence-based family violence risk factors that may be experienced by an adult, child or young person. The comprehensive assessment builds on guidance in Responsibilities 1–3 and supports a person-centred approach to assessment.
Structured Professional Judgement comprises:
- A victim survivor’s self-assessment of their level of risk, fear and safety.
- The evidence-based risk factors identified as present.
With further information to inform the assessment that you can gather from a variety of sources, including:
- Interviewing or assessing the victim survivor directly.
- Requesting or sharing, as authorised under applicable legislative schemes, with other organisations and services about the risk factors present or other relevant information about a victim or perpetrator’s circumstances.
Throughout this process and in the analysis of information to determine the level of risk, you should apply an intersectional analysis lens.
Figure 1: Model of Structured Professional Judgement
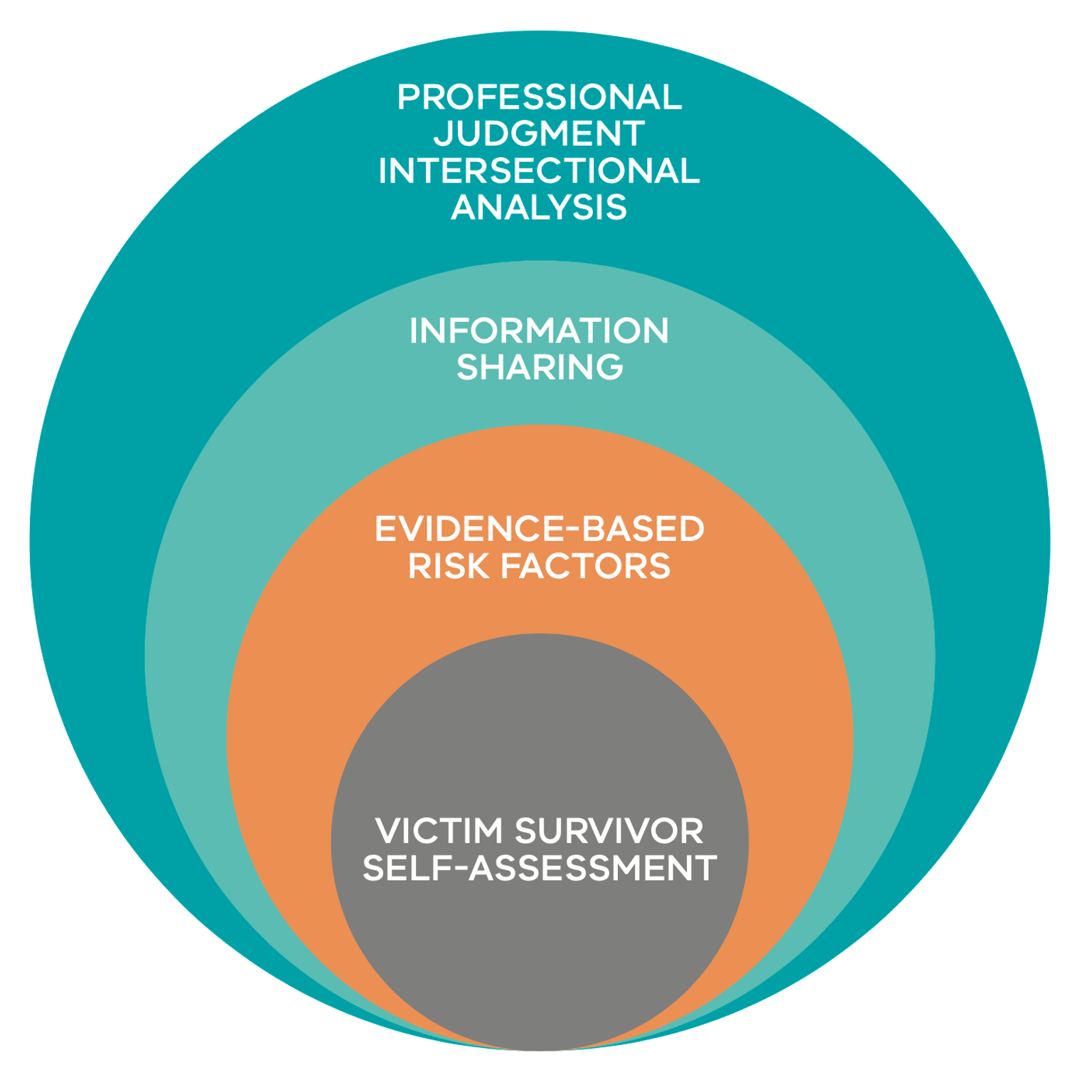
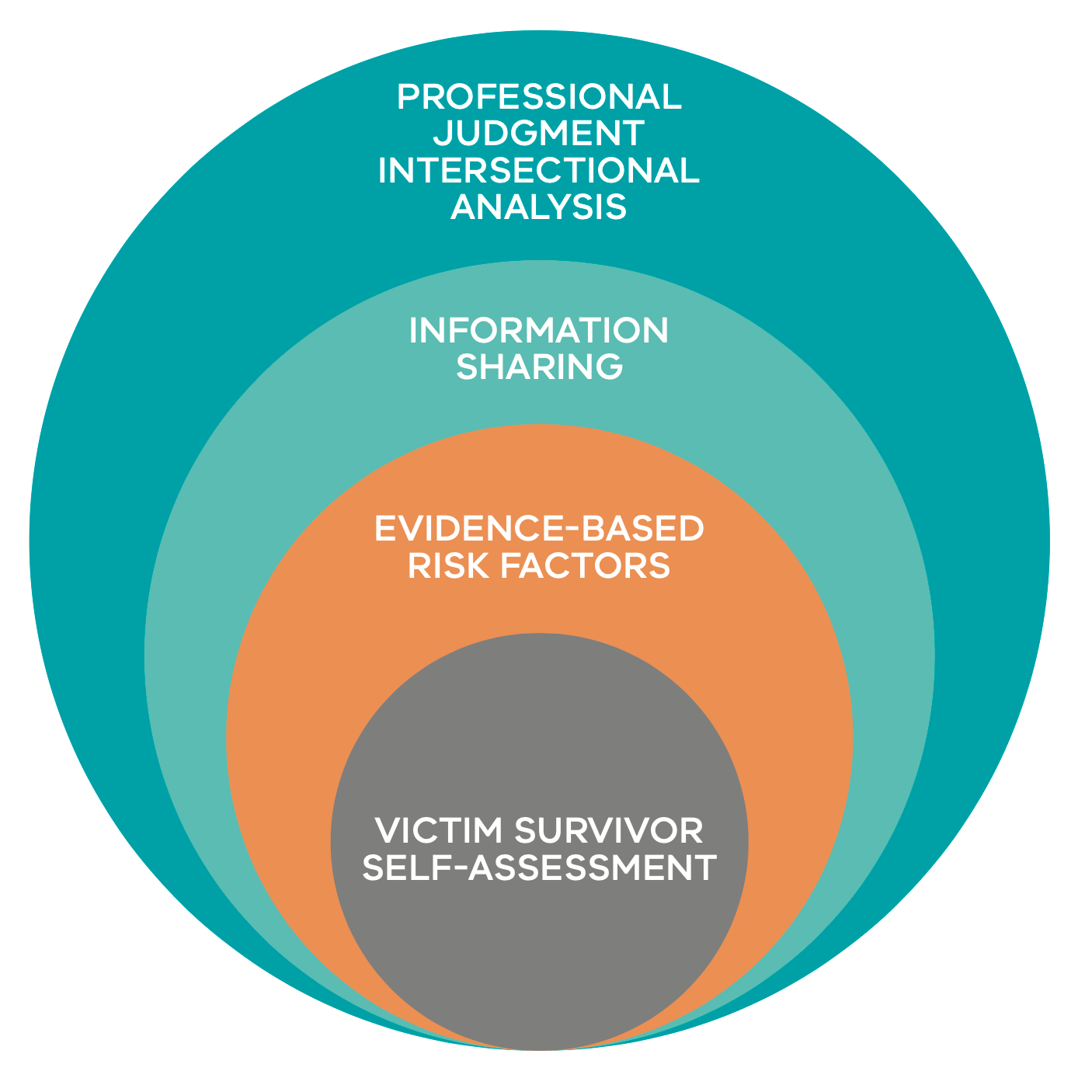{kind=link}
An adult victim survivor’s self-assessment of risk, fear and safety is central to the assessment process. Where limited information is available, a victim survivor’s self-assessment of fear, risk and safety may be relied upon to guide professional judgement about the level of risk. In the context of information known or gained through assessment and/or information sharing, you should be aware and consider if a victim survivor is minimising their self-assessment.
Assessment of evidence-based risk factors may also be informed by information sharing. Specialist family violence practitioners should be proactive in seeking and sharing relevant information to inform risk assessment and management. Information sharing and identifying risk-relevant information is more fully described in Responsibility 6.
Intersectional analysis is a key element of comprehensive assessment. Information must be considered in relation to the victim survivor’s identity, experience and impact of family violence risk. You should explore the context of barriers to accessing service responses, structural inequality and discrimination.
Using a person-centred approach is consistent with also using an intersectional lens and trauma-informed approach and helps to maintain a focus on the victim survivor and their experience. Understanding the individual’s experience and impact of family violence, as well as past service engagement and responses, will inform your professional judgement on the seriousness of risk. This understanding is also key to developing effective risk management and intervention responses.
7.3 Purpose of comprehensive risk assessment
Comprehensive risk assessment includes considering the risk, safety and needs of each individual separately, then collectively as a family unit and on the parent/carer- child bond and parenting, for example:
- each child and young person
- the parent (who is not a perpetrator)
- the parent (who is not a perpetrator) and child/ren together
- perpetrator behaviour.
The purpose of a comprehensive assessment is to:
- Determine the level or seriousness of risk and safety for each victim survivor.
- Understand a perpetrator’s pattern of abusive behaviour and circumstances to inform an assessment of whether the victim survivor is at an increased risk of being killed or almost killed (seriousness of risk), the likelihood and severity of future violence, as well as identifying imminent risk.
- Understand the full spectrum/ presentation and impact of risk, for each family member that is affected by the violence.
- Understand the level of risk at a point in time and changes in risk over time (where ongoing assessment is being undertaken).
- Explore the impact of family violence on a victim survivor(particularly children or young people) to inform short and long- term risk management options.
- Determine the most appropriate comprehensive risk management activities and to safety plan for each victim survivor.
Conducting a comprehensive assessment includes applying professional judgement to the following actions:
- Asking directly about the identity and experience of each victim survivor, other family members or people in their care and the perpetrator.
- Asking the adult victim survivor to describe their level of fear, risk and safety relating to the perpetrator’s behaviour towards them and any children. You may revisit this over the course of an assessment if you are also providing information about family violence risk which may support an adult victim survivor in determining their level of risk.
- Asking young people who are closer to adulthood about their self-assessed level of fear, risk and safety, if you believe it is appropriate for their age and developmental stage.
- Identifying the range of family violence risk-related behaviours a perpetrator is using by asking questions about known evidence-based risk factors.
- Assessing a child or young person’s risk independently and determining the most appropriate method (see Responsibility 3) by either asking questions:
- To a parent/carer who is not a perpetrator about the child’s risk, if direct communication with a child or young person is not safe, appropriate or reasonable at that time.
- Directly to a child or young person if it is safe, appropriate and reasonable using the Child Assessment Tool in Responsibility 3, Appendix 7. Note that young people who are closer to adulthood may be asked questions in the Adult Comprehensive Assessment Tool if you believe it is age and developmental stage appropriate.
- Asking questions about additional presentations of risk factors if a victim survivor identifies as Aboriginal or belonging to a diverse community or at- risk age group.
- Asking about the most recent violence, and the history of violence, by exploring patterns in previous episodes, changes in behaviour, frequency and escalation of severity. This includes what children experienced or have been exposed to.
- Identifying whether a crime has been committed (for example, physical or sexual assault, threats, pet abuse, theft, property damage, stalking and/or breach of an intervention order). See practice guidance on intermediate assessment in Responsibility 3, Appendix 8.
- Seeking relevant information from other services to assess the risk from the perpetrator in line with relevant information sharing authorisations (see Responsibility 6).
- Asking about any barriers or discrimination a victim survivor may have experienced that would impact on their experience of risk and/or ability to access services.
- Identifying protective factors that support safety and recovery, and exploring needs or wellbeing issues that might worsen the effects of violence for the victim survivor and affect the likelihood of experiencing continued violence.
- Undertaking an assessment to identify the perpetrator/predominant aggressor, if there may have been a misidentification or there is uncertainty about the identity of the parties1 (see Section 7.15).
- Using your professional judgement to determine the level of risk present and documenting the rationale for this determination.
Specialist family violence services are likely to have contact with victim survivors at points of crisis and need to quickly and effectively analyse available information to assess the level of risk and develop risk management and safety plans.
Remember
Risk assessment is a ‘point-in-time’ assessment. For specialist family violence practitioners, monitoring dynamic risk is a key part of ongoing risk assessment. This will support you to develop risk management activities and safety plans that are responsive to any changes in level of risk (such as escalation) or changed circumstances. These are discussed further in Responsibility 8.
7.4 Using genograms in comprehensive assessment
Basic and intersectional genogram symbols and guidance on how to develop a genogram are in Appendix 12.
The genogram is a graphic representation of a relationship, similar to a family tree, that details further information about relationships, hereditary patterns, identity and other family dynamics that may be important. Other details that may be included are how victim survivor/s see their relationship with the individuals listed in the genogram, remembering to also include positive aspects of relationships.
You may wish to use a genogram to better understand the victim survivor’s (adults, children and young people) circumstances and family. Developing genograms can also assist in building trust and rapport. Some victim survivors may find a visual picture confronting so use a genogram sensitively and in cases where you think it may be useful.
The genogram is an exercise also used to identify protective factors for the victim survivor when establishing a safety plan. The genogram tool helps the practitioner understand the victim survivor’s family structure and identify if there are key people that may strengthen the management of risk and implementing a safety plan. A genogram is useful during a risk assessment to identify who else may be affected by the perpetrator or if there are any additional perpetrators.
In developing a genogram, start with the family structure, and then broaden this by asking details about each person. Use the relevant symbols to visually determine any patterns arising in the family structure. Include a comment box next to the family names for additional notes relevant to that person such as:
- “Who are you closest to? Who are you not close to?”
- “How often do you see them?”
- “Where do they live?”
The victim survivor may want to think of any characteristics or habits their family members have that may be relevant to their safety needs. Consider the intersectionality of the victim survivor and family, such as cultural identities and values. Identify the experience of each family member, including where there has been experience of barriers to leaving the relationship.
This process can also identify any access requirements such as a child with a disability who may require regular support or medical intervention. Protective factors that are assessed would then be useful to incorporate into an ecomap.
7.5 The comprehensive assessment tool
Standalone templates for the:
- Comprehensive (Adult) Assessment Tool is in Appendix 11
- Child Assessment Tool is in Appendix 7.
The Comprehensive Assessment Tool is made up of questions related to the evidence-based risk factors and is supplemented with guidance on the related risk factors outlined in Appendices 8 and 13.
Comprehensive risk assessment often follows or builds on screening or intermediate assessment. You may have received a copy of a completed intermediate assessment in a referral from another organisation or professional. If so, you can review and use this information to inform your comprehensive assessment.
The Comprehensive Assessment Tool has additional questions, if applicable, relating to key risk factors for Aboriginal people or people who identify as belonging to a diverse community or at-risk age group (for example, older people).
Figure 2
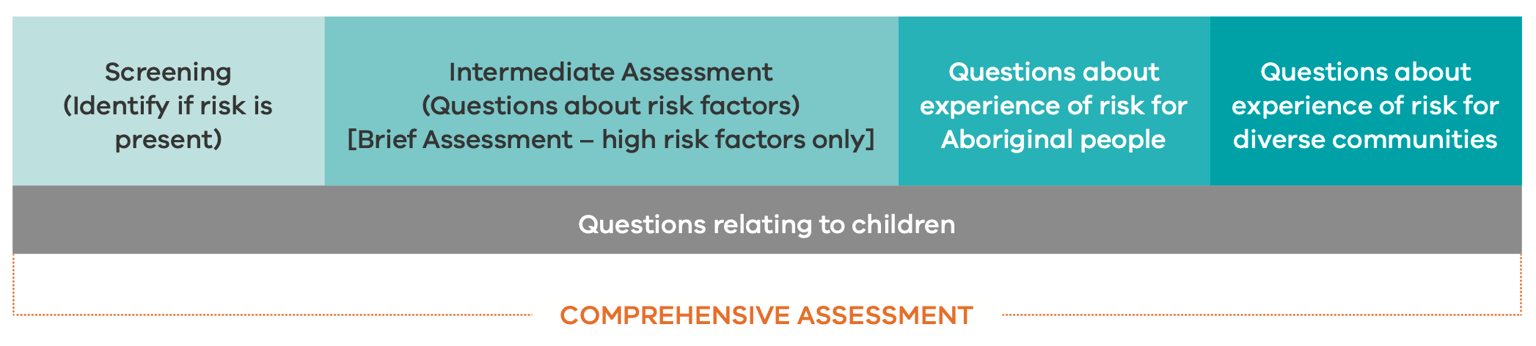
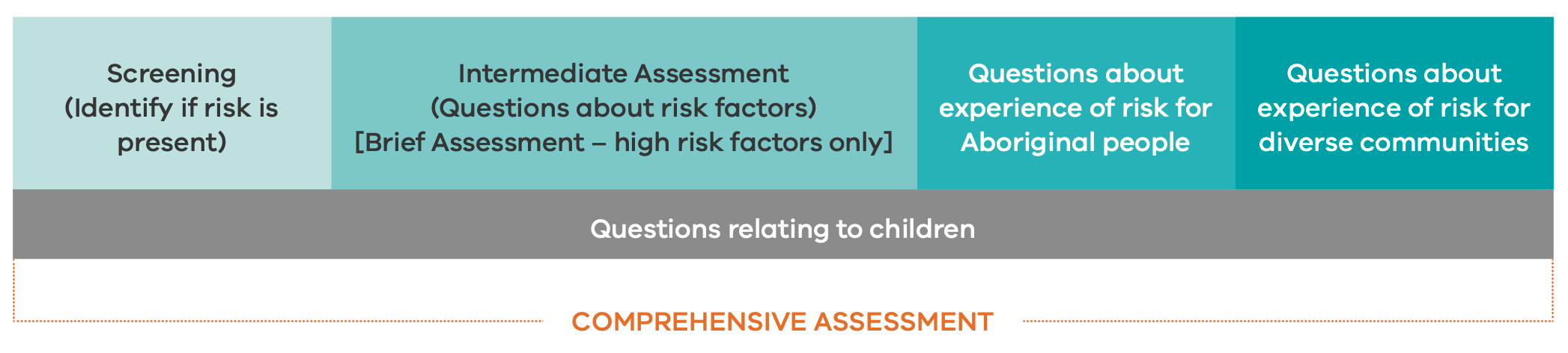{kind=link}
When undertaking comprehensive risk assessment:
- Assess an adult by asking them questions about their risk. Questions in the Comprehensive Assessment Tool are grouped according to:
- Risk-related behaviour being used by a perpetrator against an adult, child or young person.
- Self-assessment of level of risk (adult victim survivor).
- Questions about imminence (change and escalation), and
- Additional questions about presentation of risk for Aboriginal people and people from diverse communities.
- Assess a child or young person by asking questions directly about their experience of risk or through a parent/carer who may also be a victim survivor. Questions in the Child Assessment Tool include:
- A section about risk factors present from an adult victim survivor assessment. This enables you to carry over information about a parent/ carer’s risk and identify factors that are also relevant to the child’s assessment.
- Additional questions that can be asked to an older child/young person (if safe, appropriate and reasonable). These can be tailored in the language used to ensure they are also age and developmentally appropriate.
Note: Child and young person assessment tools and guidance will be developed for release in 2024. This will cover further risk factors outlined in the Foundation Knowledge Guide.
Remember
Children and young people should be heard throughout each part of the process, from screening, assessment, safety planning, needs assessment and risk management. Their voice can be heard by:
- Engaging with the adult parent/ carer victim survivor about the child’s experience of risk.
- Asking direct questions to the child or young person if it is safe, appropriate and reasonable to do so, that are appropriate to their age and developmental stage and the individual circumstances.
Supporting and strengthening the non-offending parent/carer-child bond and parenting capability is a key focus of specialist family violence practice, particularly where this has been undermined by the perpetrator’s use of family violence. For this reason, you may consider introducing questions relating to a child or young person’s experience of violence only as you develop rapport and trust with the parent/carer victim survivor, particularly if there are concerns about involvement with statutory services.
7.5.1 Responses to questions
The questions in the Comprehensive Assessment Tool are about the presence of family violence risk factors. The responses to questions are ‘yes’, ‘no’, and ‘not known’.
A ‘yes’ may be indicated if:
- The person discloses that the risk factor is present.
- You have noticed observable signs or indicators (see Responsibility 3).
- You have received the information from another source.
The context and circumstances of risk factors that are identified should be noted in comments (for example, if information is received from another source).
If you cannot ascertain the answer to a question, then use “not known”. This may be if you don’t have the opportunity to ask the question or if you don’t get a clear response. You should make a comment if you haven’t been able to ask the question.
You should let the person know that they can choose not to answer a question, if they do not want to. For example, “I am going to ask you a series of questions. All are important for assessing risk, however, you may choose not to answer any question I ask if you do not want to”. This is particularly important when communicating that information may be shared with others, particularly if there is a serious risk/threat (see Responsibility 6).
When you have a comprehensive understanding of risk, you can also explore the impact of risk to inform risk management and safety planning. This includes understanding protective factors which support safety and assist in addressing needs and wellbeing.
A comprehensive assessment should be reviewed and updated at each engagement with the victim survivor, to understand if there have been any changes and to identify escalation in risk over time. Focus on asking about changes in the perpetrator’s behaviour, including frequency and escalation, to assess whether the risk level has shifted.
7.6 Assessing risk
Risk factors outlined in the Foundation Knowledge Guide are reflected in the risk assessment questions contained in the Adult Comprehensive and Child Assessment Tools. Individual responses to each question will guide your assessment of the level of risk and corresponding approach to risk management (see ‘Risk Management’ in Responsibility 8).
Strong evidence shows that a number of risk factors are crucial indicators that the victim survivor (adults, children and young people) are at an increased risk of serious injury or death. These are high-risk factors. Children and young people’s risk should be independently assessed and informed by the risk level for an adult victim survivor, including potential risk of serious injury or death. Further guidance on assessing risk to children is in Section 7.7 of this chapter.
Remember
The level or seriousness of family violence risk is dynamic and may change over time due to changes in the perpetrator’s behaviour. It is important to regularly revisit and revise risk assessment with a victim survivor at each service engagement.
7.6.1 Levels of risk
There are three recognised levels of risk, ‘at risk’, ‘elevated risk’ and ‘serious risk’. Table 1 is replicated from Responsibility 3 for easy reference. Table 1: Levels of family violence risk
| At risk | High-risk factors are not present. Some other recognised family violence risk factors are present. However, protective factors and risk management strategies, such as advocacy, information and victim survivor support and referral, are in place to lessen or remove (manage) the risk from the perpetrator. Victim survivor’s self-assessed level of fear and risk is low and safety is high. |
| Elevated risk | A number of risk factors are present, including some high-risk factors. Risk is likely to continue if risk management is not initiated/increased. The likelihood of a serious outcome is not high. However, the impact of risk from the perpetrator is affecting the victim survivor’s day-to-day functioning. Victim survivor’s self-assessed level of fear and risk is elevated and safety is medium. |
| Serious risk | A number of high-risk factors are present. Frequency or severity of risk factors may have changed/escalated. Serious outcomes may have occurred from current violence and it is indicated further serious outcomes from the use of violence by the perpetrator is likely and may be imminent. Immediate risk management is required to lessen the level of risk or prevent a serious outcome from the identified threat posed by the perpetrator. Statutory and non-statutory service responses are required, and coordinated and collaborative risk management and action planning may be required. Victim survivor’s self-assessed level of fear and risk is high to extremely high and safety is low. Most serious risk cases can be managed by standard responses (including by providing crisis or emergency responses by statutory and non-statutory (e.g. specialist family violence) services. There are some cases where serious risk cases cannot be managed by standard responses and require formally convened crisis responses. Serious risk and requires immediate protection: In addition to serious risk, as outlined above, Previous strategies for risk management have been unsuccessful. Escalation of severity of violence has occurred/likely to occur. Formally structured coordination and collaboration of service and agency responses is required. Involvement from statutory and non-statutory crisis response services is required (including possible referral for a RAMP response) for risk assessment and management planning and intervention to lessen or remove serious risk that is likely to result in lethality or serious physical or sexual violence. Victim survivor self-assessed level of fear and risk is high to extremely high and safety is extremely low. |
7.6.2 Victim survivor’s self-assessment risk
This section builds on guidance in Responsibility 3, Section 3.7.5.
The questions in the section ‘Self-Assessment’ in the Comprehensive Assessment Tool explore the survivor’s view about their level of risk.
You should revisit the self-assessment at the end of the risk assessment process. The victim survivor can further assess their level of risk, based on your discussion regarding risk factors present, the information you provide about them and your concerns.
Evidence is clear that an adult victim survivor’s self-assessment of risk should be a crucial input to your assessment. Where self-assessment questions indicate that the adult victim survivor considers themselves (or any child victim survivor) to be at ‘high’ risk, they will be determined to be at serious risk, even if other risk factors have not been identified as present.
Self-assessment may cover questions relating to an adult victim survivor’s feeling about level of risk. This may include asking them to describe how they feel fear, such as:
- “How scared or afraid do you feel given what happened in the last incidence?” (such as ‘not afraid’, ‘afraid’ ‘very afraid’ or ‘extremely afraid’)
- “Do you think the violence will continue?”
- “How do you know when you’re not safe? How does your body respond to danger? Is the situation getting worse?”
A young person who is closer to adulthood may be asked to self-assess their risk.
If age and developmentally appropriate, an older child may also be asked about their level of fear, and the impact or anxiety they may feel relating to their experience of risk may inform your assessment. It might be useful to provide a scale, such as:
- “Are there times that you feel unsafe or scared?”
- “How unsafe do you feel? Can you answer this as a number out of ten, if 1 is a little bit scared, and 10 is very, very scared?”
- “Are there people in your family that you feel nervous or scared around? Who?”
- “Do you feel that way all the time or just sometimes? When?”
- “What is usually happening when you feel frightened? What do you feel frightened about?” (prompt for fears for self, mother, siblings or other family members, possessions, pets)
There is no current evidence base that a younger child’s self-assessment of risk is reliable in determining their level of risk. However, asking the child or young person about their experience of fear may support validation of their experience by supporting them to feel heard, and for you to consider in your risk management responses.
When children are too young to be interviewed or talked to about their experience of family violence, behavioural observation from other sources such as school and day care can assist in the assessment process, particularly observation about changes in behaviour.
You can ask an adult about their child’s experience of risk or fear, such as:
- “What do you notice about your children’s behaviour when violence is occurring?”
- “Have you noticed a change in their behaviour?”
Information from a parent/carer about how a child may be experiencing fear or risk may inform your assessment. However, each child’s risk should be assessed independently. An adult’s self-assessment of fear, risk and safety is also relevant to assessing the risk to a child.
There may be times when their self- assessment of their level of risk or fear may not align to your assessment of risk factors present and the level of risk to themselves or their children. This might be because they fear the consequences of disclosure or have become desensitised to high levels of risk and violence due to their experiences.
You must use all the information obtained from the assessment process (including information shared from other sources such as police) to determine how much emphasis to give to the victim survivor’s assessment of their situation.
Some victim survivors may be acclimatised to a level of risk or fear, often as a coping mechanism. They may indicate a low level of risk or fear if you have not yet established a level of trust or they are concerned about the involvement of Child Protection or other services. If the presence of risk factors indicates a level of risk which is inconsistent with a victim survivor’s own views about risk, fear or safety, you should sensitively enquire into their reasoning for the self-assessment. This may include providing information about the evidence base for risk factors, and your concerns about the level of risk from your assessment.
Remember
Many victim survivors fear having their child/ren taken from them by Child Protection. This fear might be particularly strong for Aboriginal women, women with a disability or serious mental illness, women from a multicultural, faith or linguistically diverse community, including women who are not permanent residents, and women who were either removed themselves or have had children removed previously. It is not uncommon for perpetrators to use threats to have children removed.
Directly acknowledge a victim survivor’s fears and be clear about your agency’s processes regarding duty of care. It is helpful to use a strengths-based approach, in which you affirm the victim survivor’s attachment to their child, and work towards establishing your shared commitment to the child’s wellbeing.
Victim survivors with a disability might benefit from additional specialist support or advocacy in this context. Secondary consultation with or direct involvement (with the victim survivor’s permission) of an Aboriginal or bi-cultural worker could help you to understand and respond sensitively to the depth of child-removal concerns held by Aboriginal victim survivors, or victim survivors from multicultural, faith and linguistically diverse communities. This is an important aspect of cultural safety.
7.6.3 Severity
This section builds on guidance in Responsibility 3, Section 3.7.5.
Severity can be explored by asking questions about current risk factors and history of violence. The presence of high- risk factors, the recency/currency of these behaviours being used, together with the likelihood and timing of future violence occurring, can assist in understanding seriousness of risk.
7.6.3.1 Static and dynamic risk factors:
Risk factors are recognised as static or dynamic. That is, how much they change (present/not present, frequency, escalation). Some risk factors are ‘highly static’, such as history of violence. Some are ‘highly dynamic’, such as alcohol/substance abuse/ misuse or access to weapons. The key to understanding seriousness of risk is to understand how risk changes or escalates over time.
To understand and analyse changes in risk or escalation over time, you should regularly revisit these questions with a victim survivor (ongoing assessment). Some victim survivors will also moderate how much information they provide, particularly if you are in the early stages of building trust and rapport. Further detail on ongoing assessment is in Responsibility 10.
Further information
Relating ‘serious risk’ to ‘serious threat’
The determination of ‘serious risk’ correlates to the test of ‘serious threat’ set out in the Privacy and Data Protection Act 2014 and the Health Records Act 2001. The test for these Acts relates to broader serious threat to life, health, safety or welfare of any individual which may occur within or outside the context of family violence. If a serious risk has been identified through assessment under the MARAM Practice Guides, this is considered akin to a determination of ‘serious threat’ for the purposes of sharing information without consent to lessen or prevent a serious threat under these Acts.
When high-risk factors indicating severity are identified as present, particularly if they are assessed as changing or escalating this may indicate that the risk of likelihood is also increasing or becoming imminent.
7.6.4 Likelihood and timing
Likelihood and timing are understood through an analysis of history and patterns of violence and changes to frequency and escalation.
Likelihood and timing should be explored by identifying risk factors that are ‘likely’ to happen ‘soon’ or at a known time, such as release of a perpetrator from correctional services. Likelihood and timing can be difficult to assess without a current/ known threat. An analysis of the current risk factors, changes to frequency and escalation, and a history of violence can provide strong evidence. Each identified risk factor should be responded to through risk management and action planning (including information sharing), appropriate to the identified severity and likelihood/ timing.
Timing is broader than the concept of imminence2, which is the proximity of threat or a known risk factor and evidence of likely immediacy that the risk will occur. Imminence may indicate how quickly and also what crisis or urgent risk management or perpetrator intervention responses should happen.
Table 2 (below) outlines the Comprehensive Assessment Tool questions, as well as guidance on the context and importance of the questions and suggested level of risk based on the individual’s response to these questions.
7.6.5 Frequency
Likelihood and timing can be further analysed by understanding frequency. You should explore if frequency has changed or escalated, particularly for identified high- risk factors.
If the answer to a question is no, no further exploration is required for that factor, and you can state that if this occurs in future, to keep you informed and seek further assistance.
If the answer to a question is yes, you can explore frequency by providing examples of time periods and asking, “How frequently?” to establish a baseline.
Frequency by itself is not always a significant indicator of the level of risk — you should further explore questions to understand if frequency has changed or escalated. This is particularly important for some high-risk factors. You can ask, “Has this changed in frequency or escalated recently? Over time?”.
Table 2 (below) is a guide for exploring frequency as a baseline to support identifying escalation or changes in risk factors being used. If a victim survivor provides an alternative way of describing frequency or change, you can be guided by their approach.
Table 2: An example of responses that may assist you to explore frequency include:
| Frequency description | Example of frequency (to support a shared understanding) | Action |
|---|---|---|
| Once only or | A few times per year | Provide information and resources, including to seek assistance if change or escalation in frequency or severity such as behaviour causing fear, occurs. |
| Rarely | ||
| Sometimes | Monthly / at least once a month / every few weeks Has the frequency or severity changed/escalated? | This may indicate elevated risk. You should continue with the assessment to understand if urgent risk management action is required, and/or consultation/referral for comprehensive assessment should be undertaken. |
| Often or | Weekly / at least once a week Daily Has the frequency or severity changed/escalated? | This may indicate serious risk. If this relates to high-risk factors, consider if urgent action is required, undertake risk management and safety planning, and/or seek secondary consultation/referral for comprehensive assessment and management. |
| Always/all the time |
It is also critical to understand the frequency of feeling afraid, in order to guide you on whether any immediate management responses are required.
7.6.6 Change or escalation in frequency or severity
After you have explored frequency, you can ask related questions about change in use of behaviours that might indicate escalation.
If risk has changed in frequency or by the nature of behaviours being used by a perpetrator, this would indicate escalation of risk. It is a strong indicator of seriousness of risk if the perpetrator is using more specific threats or increases the use and severity of violence.
After you have explored frequency, you can also ask related questions about change in behaviours/risk factors that might indicate escalation in either severity.
- If risk factors have changed in terms of frequency or in the nature of the perpetrator behaviours (for example, increased severity) this would indicate escalation of risk. It is a strong indicator of seriousness of risk if the perpetrator is using more specific threats or increases the use and severity of violence.
- You should also consider the scale of the escalation and the impact on the victim survivor.
Change or escalation in frequency or severity may also relate to the history of violence used and threats that the violence will occur again. For example, the frequency of the use of violence may be low, however, the threat is current/ongoing and severity level is high. This is particularly important for physical harm and sexual assault of victim survivors, which may have occurred in the past and there are current threats from the perpetrator that this violence will reoccur as a tactic of coercive and controlling behaviours.
7.6.7 Information sharing
As outlined in Responsibility 6, you should actively seek relevant information from other sources to inform your risk assessment. This information can be included in your assessment, and supplement information that is received from the victim survivor. You can include information received about risk factors as ‘yes’, ‘no’ and ‘not known’ in the comprehensive assessment and note the source in comments.
7.6.8 Determining seriousness of risk
Use the model of Structured Professional Judgement to determine seriousness of risk by considering the range of information available to you, as well as your analysis of how these elements interact. This process should be applied to both adult and child victim survivors.
Where considering risk for children, refer to additional guidance at Section 7.7 in this chapter.
Apply an intersectional lens to this model by ensuring each victim survivor’s identity and experience of structural inequality and discrimination is considered in relation to how this interacts with their experience of risk. Practice guidance on some of the common presentations for people who identify as Aboriginal or belonging to a diverse community are explored in Appendix 13.
Risk assessment relies on the elements of:
- A victim survivor’s self-assessment of their level of risk, fear and safety.
- The evidence-based risk factors identified as present.
With further information to inform the assessment that you can gather from a variety of sources, including:
- Interviewing or ‘assessing’ the victim survivor directly.
- Requesting or sharing, as authorised under applicable legislative schemes, with other organisations and services about the risk factors present or other relevant information about a victim or perpetrator’s circumstances.
These elements, and your analysis of their interaction with protective and circumstantial factors, support you to form a judgement on the level of risk.
The victim survivor’s self-assessment of risk is a key component of the risk assessment and should be considered at each assessment. Self-assessment of risk, safety and fear is often an accurate source of information on the seriousness of risk, even if other risk factors have not been identified as present during assessment.
When a victim survivor indicates that:
- Some of the risk factors are not present or are rarely present.
- That the high-risk indicators are not occurring.
Then their risk level is determined to be at a lower level and a corresponding lower level response is recommended.
Each risk factor that is threatened or identified as present, should be considered in the context of their severity, timing and likelihood of actually happening, particularly high-risk factors. These are described above 3 as:
- Severity: the risk will result in significant consequences. That is, it is likely to result in a victim survivor being killed or almost killed (such as serious injury), and may be indicated by the presence of high- risk factors. When high-risk factors are identified as present, particularly if there has been a change in frequency or escalation, this would indicate a serious level of risk.
- Likelihood and timing4: the chances that the risk will actually happen, or it is likely the risk of harm will occur, as well as how soon the threat is likely to occur or if the threat is ongoing. Likelihood may be assessed with an understanding of the history and pattern of violence used and exploring change in frequency or escalation over time.
You can consider risk factors in the context of protective factors. These are not used to understand risk mitigation but should inform seriousness of risk and its impacts, and risk management planning.
You should apply an intersectional analysis lens to risk factors identified, and whether the presentation, impact or responses to any risk factors should be specifically responded to through your risk management response.
Together this information — reflecting on the description of each risk level on the actions required of you or other services to mitigate the identified risk (at Table 1, above) — will support your decision-making on the level of risk present, and your risk management planning.
7.7 Assessing children and young people
You may work with children and young people directly or indirectly and this will vary on a case-by-case basis. Several factors may influence direct interaction with children and young people including, the age and developmental stage of each child or young person, their circumstances, and whether direct service access is available (for example, an adult victim survivor may be accessing services while the child/young person is in school).
Working with children and young people can include:
- Risk and needs assessment for each child or young person via the parent (who is not a perpetrator).
- Risk and needs assessment directly with the child or young person.
- Addressing children and young people’s needs individually, and in conjunction with the parent (who is not a perpetrator), including increasing protective factors.
Remember
Children and young people can be affected by family violence even if they do not directly witness it. You should always ask the parent/ carer victim survivor about what any children or young people who live with them (or who have contact with the perpetrator) are experiencing.
The impact of direct and indirect experiences of family violence is commonly called ‘child abuse’. However, you should be aware that this is often an outcome of family violence behaviours being used by the perpetrator against the child (directly) or they are witnessing or being exposed to the impacts on a parent/carer and their relationship.
Where family violence risk factors are being used by a perpetrator each adult and child family member should be assessed for their experience of family violence risk.
The purpose of a family violence risk assessment for children and young people is to identify and manage risks that the family violence poses to their safety and wellbeing. Risks can present and impact on children and young people differently, depending on their age and developmental stage, as well as particular circumstances.
These risks may include:
- If an adult has been identified as a victim survivor, children and young people are also likely to be victim survivors in their own right, either directly or indirectly experiencing violence.
- The possibility that a sibling, grandparent or extended family member is perpetrating family violence against them.
- Children witnessing or overhearing the violence causes fear and other harm.
- Children and young people are not usually passive bystanders. The perpetrator may draw them into the abuse, using coercive tactics such as criticism and undermining. Alternatively, the child or young person may intervene to protect the other parent or find other ways to try and manage the violence.
- Family violence impacts the health, mental health and emotional wellbeing of children and young people. Tactics of abuse may also include undermining parenting, negatively impacting the relationship of the child or young person with their parent/carer who is also experiencing family violence.
- A number of factors can influence the impact the family violence has on the child or young person’s welfare such as individual characteristics, attachment to parent and protective factors such as a supportive school, friendships and extended family members.
- The perpetrator may not return children from shared care arrangements, or in some circumstances may abduct children.
- The possibility of destructive behaviour between siblings.
- The capacity of the perpetrator for change to stop the family violence and to support a healthy relationship that meets the emotional and developmental needs of the child.
The risk and needs of children and young people can be different to those of the adult person experiencing family violence. Each child in the family may also be affected differently and react differently to dynamics of family violence. You should understand a child or young person’s experience in the context of their development, daily life, sibling, parental and peer relationships, and connection to culture and community. Also consider the impact of family violence on the family functioning, such as financial abuse, the disabling of the child’s mother through violence, the need to constantly re-locate etc.
Establish if Child Protection or child and family services have been, or are, involved. If the adult victim survivor tells you that their child has been hurt or injured or are showing signs of significant trauma, follow your obligations to report to child and family services or Child Protection if there is significant concern such as physical or sexual abuse of children.
7.7.1 Approaches to assessing children or young people
Your assessment must focus on the risk and needs of the children or young people.
The Child Assessment Tool in Appendix 7 includes questions that can be asked:
- Of a parent/carer about a child/young person.
- Directly to an older child or young person if age and developmental stage appropriate.
It also includes questions that may be asked of younger children if age and developmental stage appropriate.
You should also consider if there are multiple family violence perpetrators and who might be a supportive adult if both of the children’s parents/carers are using family violence behaviours.
Remember that it is ideal if an older child or young person can be directly asked about how safe they feel and what they need in order to feel safe. A trauma- informed approach should be used which understands the child’s behaviour in terms of their experiences of abuse and fear. Considerations for children must be appropriate to their developmental stage and include:
- Their own views of their needs, safety and wellbeing.
- Their current functioning at home and school and in other relevant environments.
- Their relationships with family members and peers.
- Their relationship with the perpetrator.
- Their relationship with other people experiencing family violence in the household, particularly if it is their mother.
- Their sense of cultural safety, where relevant.
- The level of support available if they are a child with a disability.
- Their developmental history, including experiences of family violence or other types of abuse or neglect.
Consider if the child or young person is at risk from people outside the family, such as in the community, in clubs or other social engagements. This may indicate there is an environment of polyvictimisation (that is, multiple sources of harm, including outside of the family) that may connect to a child’s family violence risk. The Foundation Knowledge Guide outlines risk factors of a child’s circumstances which may support you to identify external risk.
If external risk factors relating to a child’s circumstances are present, this may also indicate the presence of family violence. If a child or young person is experiencing risk in the community, consider how this is cumulatively impacting them, and also how you might manage both causes of risk.
Rapport is particularly important as a child or young person will need to have some confidence in you before answering the risk assessment questions. Use child friendly activities and age and developmental stage appropriate supports for talking with young children (refer to Responsibility 1).
Work to create a place of emotional and physical safety for the child before asking assessment questions. Start by asking prompting questions such as:
- “What are the things that make you feel happy or that you like to do?”
- “Who supports you?”
- “What are the things that make you feel safe?”
7.7.2 Other considerations in assessing risk to children and young people
To understand the impact of violence on children and young people, you should maintain a lens on the parent/carer-child bond (usually a mother who is also a victim survivor) and parenting. You should:
- Ensure you do not blame the child or young person or parent/carer (who is not a perpetrator) for family violence or its impacts.
- Strengthen parenting and the parent/ carer-child bond, which may have been undermined by the perpetrator.
- Hold perpetrators accountable, by placing responsibility for the use of violence with the perpetrator, not the child/young person or parent/carer (who is not a perpetrator).
- Advocating to services and systems, in partnership with the parent/carer who is protective, so that they are not held responsible for the perpetrator’s actions and behaviour or its impact on children and young people.
- Recognise and respond to the direct and indirect impact on children and young people including emotional, social, educational challenges, and attachment or bond with the parent/carer (who is not a perpetrator).
There may be some barriers to parent/ carers engaging and disclosing risk to children and young people. These may include parental shame, fear of statutory intervention and child removal, seeing questions as intrusive and undermining, particularly if a perpetrator has used violence to attack the parent/carer-child bond.
Remember
Your assessment will be more accurate and complete if children and young people have direct input. For example, you might note there are a range of potentially supportive adults in a child’s life. However, the child themselves is best placed to tell you if they see these adults as supportive, and the degree to which they feel safe or trust them.
7.7.3 Parental guilt and shame
A parent’s sense of guilt and shame about their own and their child’s experience of family violence might have a significant impact on their ability to engage with you and the assessment process. You need to be able to draw on a parent’s knowledge of their child for the assessment and should do so in ways that do not reinforce guilt and shame or reduce their engagement. Parents/carers can minimise the impact of violence on a child, due to fear or concern about child removal.
You should outline the purpose of the assessment questions so that the parent/ carer can understand the importance and scope of the questions and what you will do with the information. Explain to the parent/ carer the importance of understanding the risk of each family member individually, as well as risk for the family unit. Also, explain that this will support your risk management and safety planning responses.
Your role is to assist them to take an objective look at the child’s experience, feelings and needs. It can help to:
- Acknowledge any shame or guilt that the parent/carer might be feeling.
- Reinforce the perpetrator’s responsibility for the violence and its impact of violence.
- Outline the shared responsibility of all adults in a child or young person’s life to contribute to their safety and that they cannot individually be held responsible for keeping the child or young person safe.
- Emphasise the need for the child to be safe and supported, and briefly outline what might be needed for this to happen with assessment being a key step in this process.
A parent’s feeling of shame can arise at any time while you are talking. As the discussion progresses, the enormity of the impact of family violence on a child might become more apparent to the parent/ carer. Take care to maintain engagement by recognising and responding to signs of shame.
For Aboriginal people, colonisation, dispossession, and current and past policies and practices have created a deep mistrust of people who offer services based on concepts of ‘protection’ or best interest. By acknowledging these thoughts and feelings you can support and advocate for Aboriginal parents/carers to maintain and strengthen parenting and bond with their children, when you are also required to report the behaviours of the perpetrator to statutory services.
Be aware of victim-blaming beliefs and perceptions such as misconstruing actions which are protective with responsibility for the child or young person’s experience of risk and its impacts, including for adult victim survivors who are living with or share parenting responsibilities with the perpetrator.
7.7.4 Communicating risk for children or young people to their parents
It is imperative for you and the adult victim survivor to understand the impact the family violence is having on any children in the family. A good place to start is by asking adult victim survivors whether they believe the children are safe in the family home. Adult victim survivors may need support to understand this.
Sometimes a parent/carer can be guided to a greater understanding with questions, such as:
- “How do you think (child’s name) would describe life at home?”
- “What changes do you think (child’s name) would like to see made at home?”
- “Have you noticed how the children are after (perpetrator’s name) has been violent to you?”
A parent/carer may seem unaware of the impact on, or level of risk for the child or young person or may have a view of the level of risk that differs from your observation or judgement. If this occurs, you could:
- Ask what behaviours they have noticed in their child/ren — is there anything worrying them about those behaviours?
- Discuss the different behaviours that children are showing and whether any of them are of concern (e.g. inability to sleep, problems fighting with other children, bed-wetting etc.).
- Provide resources on the impact of family violence on children and young people.
- Ask them about the ways in which they have worked to protect their children. Make sure that these protective actions are clearly documented. Explore further whether protective actions that have previously worked are now no longer working.
- Encourage them to discuss the issue further with a worker who works closely with children.
Your role is to validate and understand the experience of victim survivors and support the adult victim survivor (who may be a parent/carer) to validate and understand their children’s experience of the family violence. Exploring this together is an important aspect of ongoing intervention with a parent/carer and child victim survivors and must be considered in planning for risk management.
7.8 Assessing violence by a child or young person against a family member
7.8.1 Overview
Violence can be used by a child or young person against any family member, including a parent, sibling, or other family member. A young person may use violence toward their intimate partner. This is often referred to as adolescent family violence.
Remember
Under the Family Violence Protection Act 2008 ‘child’ is defined up to age 18 years.
‘Young person’ is not defined in legislation and may be up to age 25 years.
Violence used by young people is sometimes described as ‘adolescent family violence’. However, the age group of children and young people can extend outside of the ‘adolescent’ age period of 12 to 18 years.
The behaviours used by a child or young person may reflect the full range of recognised family violence risk factors. Children and young people that use violence may themselves have also experienced or are continuing to experience family violence.
The terminology ‘child or young person who uses violence in the home’ should be used instead of perpetrator. Family violence by children or young person has different characteristics and unique responses are conceptualised and practiced for this vulnerable cohort. Use this terminology in practice to support engagement of families and parents/carers who may not want to talk about their children as abusive or violent. Using the term ‘perpetrator’ may create a barrier if there is a degree of parent/carer shame, self-blame, denial or fear of criminal, service or statutory involvement. It also does not adequately respond to situations where a young person has also experienced family violence.
Children and young people who use violence often experience complex behavioural, mental, physical and emotional issues, such as:
- Neurobiological harm caused by developmental trauma (exposure to family violence or neglect).
- Emotional harm caused by recent exposure to family violence, abuse, abandonment or chronic neglect, substance abuse, family breakdown, unresolved grief and loss.
- Undiagnosed mental health issues.
Children and young peoples’ use of violence may co-occur with substance use, health issues or education/social disengagement, which increase existing emotional dysregulation.
Children and young peoples’ use of violence towards family members has both similarities and differences with adult- perpetrated family violence. Adolescent family violence is gendered with the majority of violence being used by male children and young people. However, female children and young people also use violence, and fathers and other adult and child family relatives may be victims. The drivers of this form of violence is also from a sense of entitlement to gain power and control. Similarities lie in the fact that the majority of victims are female (mainly mothers and often single mothers).
More male than female children and young people are involved in using violence towards a family member, but the pattern is not as marked as in adult violence. The general pattern is for girls to begin at an earlier age and grow out of the use of violence and abuse, while boys may begin later but the violence may increase with age and may also begin to present in their intimate relationships. Where there are other children in the family, there is a high probability that they will be experiencing violence, as well as their parent/s. Research suggests that abuse of parents/carers tends to begin with verbal abuse before escalating to other forms and can increase in both frequency and intensity without intervention.
While violence by an adolescent is clearly a form of family violence, the risk assessment practice should reflect both their use and experience of violence, and risk management responses need to be clearly differentiated from the response to adult perpetrators. Remember that children and young people are still developmentally young, and you should consider their protection, safety and developmental needs, as well as how to address their offending behaviour. A therapeutic and holistic response which addresses risks and needs as well as the sources of violence and abuse are recommended over a criminal justice response.
A key focus of effective interventions should be family connection, as well as the child or young person’s wellbeing and safety within the context of the violence they are using. Similar to adult perpetrators, responses should focus on responsibility and accountability and you should be aware of the behaviours that may minimise, justify, deny or seek collusion from you or others for their behaviour, or impute blame on others for their behaviour.
Challenges arise for all workers (including police) in finding an appropriate balance between safety for family members and responding to the needs of the child or young person involved in abusive and violent behaviours. The focus on maintaining family connection should prioritise the safety of all family members, and restorative processes may be used to support sustainable change.
7.8.2 Underlying factors and context to adolescent family violence
Assessment and management of risk requires an understanding of the underlying factors and context for the violence. Adolescent violence is very diverse and can be made up of a range of patterns. For children and young people this may include:
- Also being victims of violence from an adult family member (usually their fathers or father figure). Young people may actively use violence against an adult perpetrator of violence as a form of protection for themselves or another family member.
- Having grown up experiencing violence which has become normalised.
- Modelling and learning that violence is a way of resolving conflict and exerting power and control over others. For example, becoming a ‘proxy’ abuser towards their mother with encouragement from their father or step- father.
- General and developmentally low capacity for emotional and behavioural self-regulation.
- A strong sense of entitlement, particularly as young people move from childhood, which is characterised by parents responding to needs and desires, to adulthood. Young people may use violence and abuse when their inappropriate behaviour and demands are challenged as they become teenagers.
- Escalation of violence is associated with problematic substance use, as well behavioural issues related to school/ social disengagement (refusal or removal).
- Having a disability, such as autism, intellectual disability and acquired brain injury, can exacerbate use of family violence behaviours. There is a resulting over-representation of young people with these issues in this cohort. Where family violence is a pattern of coercion and control, behaviours due to cognitive, emotional regulation or other related cognitive impairments should also have a disability and medical needs response.
- Young boys in particular may become unsafe in their behaviours with family members (particularly their mothers) as they grow and become physically stronger.
- Use of sexually harmful behaviours, including toward mothers and vulnerable younger siblings, including where a young person has experienced family violence or sexual abuse themselves.
Responses to adolescents’ use of violence should cover a range of areas, including attachment, communication, discipline practices, parenting confidence and relational frustration, such as:
- Support for adolescents to improve their communication, problem-solving skills and emotional regulation skills. This could include teaching adolescents to separate emotions from behaviours, and providing space for self-soothing and conflict resolution.
- Being aware and providing support for any health and wellbeing needs, such as social/education engagement, learning issues, drug or alcohol misuse/abuse, mental health issues, or therapeutic responses to their experience of violence or abuse.
- Supporting parenting confidence to work with adolescents to reduce their violent behaviours such as:
- Better recognizing unhealthy patterns.
- Moving from destructive to constructive forms of communication.
- Reducing engagement with conflict or ‘walking away’ to prevent escalation.
- And use of positive disciplinary strategies, such as boundary setting and consequences for abusive behaviours.
- Supporting engagement with criminal justice processes where, as much as possible, responsibility and accountability are promoted.
- Offering appropriate supported accommodation options when the family is not safe if the adolescent remains in the family home. This should be alongside continued support to respond to their behaviours and needs and if possible, to maintain family connection.
7.8.3 Working with other family members affected by a child or young person’s use of violence
The assessment of the child or young person’s risk to family members is essential to set the engagement context. Comprehensive assessment can be undertaken with adult and child family members who are not using violence to understand the risk factors present and the unique family circumstances. Siblings and other children in the home will need to have their risk independently assessed, either directly, if age and developmentally appropriate, or through a parent/carer who is not using violence (usually their mother).
Family members experiencing violence, particularly parents/carers, may be reluctant to report violence from a child or young person towards themselves. There may be deep feelings of shame or fear of the consequences, both for themselves and the young person, if authorities and organisations are involved. Your approach needs to be sensitive and non-judgemental. You will need to be well informed about the range of services that may be available to all family members, including the child or young person using family violence.
A further consideration is exploring whether there are issues of adult family violence. The child or young person may be both a victim survivor and using violence, and the adult family violence will need to be responded to as outlined in other parts of this guidance.
7.8.4 Working with the child or young person using violence
As with children and young people who are victim survivors, children and young people using violence should be directly asked about their behaviour and its impact on other family members. This should maintain a trauma-informed, age and development stage appropriate lens, as well awareness of the needs and circumstances.
The engagement with the child or young person will be dependent on their context and lived experience. For example, if they have a disability, cognitive impairment or developmental delay, problematic drug or alcohol use, or experiences of being a victim survivor of family violence. Preferably, more than one person should be present when interviewing the young person. This could be via collaborating through secondary consultation or a co-case management arrangement. The appropriate ‘team’ should be tailored to the age and developmental stage of the child or young person and should include any relevant service supporting them in other presenting issues.
Note: Practice guidance for working with young people who use violence is currently in development.
This will be done by asking questions about experience of risk of other adult and child family members who are not using violence.
7.9 Inclusive practice and applying an intersectional lens when assessing risk
Applying an intersectional analysis lens when assessing risk means understanding that a person may have experienced a range of structural inequalities, barriers and discrimination throughout their life. These experiences will impact on their experience of family violence, how they manage their risk and safety, and their access to risk management services and responses. A person’s identity and experiences of structural inequality and discrimination will influence how they might:
- Talk about and understand their experience of family violence, or presentations of risk.
- Experience trauma or relate family violence to their experience of barriers, structural inequality, and discrimination.
- Understand their options for service responses or who they may seek services from.
- Explain impacts of the violence they experience.
Remember
Each common question and section of practice advice outlined in the Comprehensive Assessment Tool (Appendix 13) responds to one aspect of identity or experience. However, people are multi- faceted and may identify with a range of identities or experiences. You should consider each aspect and look at the person’s whole identity and experience. Think about how these inform your assessment of the level or ‘seriousness’ of risk, and your response.
Where an individual has identified as Aboriginal or belonging to a diverse community or is an older person, there are additional questions in the Comprehensive Assessment Tool (Appendix 13) which can be asked about their experiences of risk.
While an in-depth understanding of another person’s identity may not be possible, be open to the ways that victim survivors might present and ask about and engage with them in ways that are responsive to their lived experiences. You should explore how experiencing structural inequality or discrimination (outlined in the Foundation Knowledge Guide) creates barriers and impacts access to services. You should acknowledge this and work with the victim survivor and other services to actively address these.
This guidance addresses the most common presentations of key risk factors, but does not cover all presentations. If you encounter issues not addressed or the victim survivor indicates a number of areas of diversity, consider secondary consultations with appropriate support agencies to assist you to provide supportive and culturally respectful service responses.
You should also note that there may be multiple perpetrators. This additional consideration should inform how you ask questions about behaviour being used and by whom.
You could lead in to these additional questions with a statement such as:
“You have let me know you identify as [name community or group]. We ask additional questions as risk can present in a number of ways and this will assist me to understand if that is occurring for you.”
“This information supports me to determine your level of risk and how we will respond.”
7.10 Assessing for traumatic or acquired brain injury as a result of family violence
Risk assessment questions and risk management strategies relevant to traumatic brain injury (TBI) or acquired brain injury (ABI) and family violence is an emerging area of practice. The Intermediate and Comprehensive Assessment Tools have follow-up questions related to risk factors that are more likely to be associated with TBI from physical harm and loss of consciousness (for example, from strangulation or choking).
This includes the demographic questions on disability (adults, children and young people) which may result in the victim survivor informing you that they have an ABI diagnosis. This may prompt you to consider seeking assessment for potential diagnosed or un-diagnosed traumatic brain injury. You should also consider this in assessment of seriousness of risk and risk management planning.
If an undiagnosed brain injury is a possible issue arising from the risk assessment, practitioners should be careful not to jump to conclusions. Support victim survivors to access specialist neuropsychology care via a referral from their GP as an important part of the risk management plan. This will ensure that they are appropriately assessed for an accurate diagnosis and provided with specialised treatment and resources to support their recovery.
7.11 What should you keep in mind when asking risk assessment questions?
Remember:
- Although the risk assessment tool has ‘yes’, ‘no’ or ‘not known’ answers, context of the risk being experienced should be documented in comments. When asking questions, it is preferable to use a conversational manner to ensure the victim survivor feels understood and supported to tell you about their experiences.
- It is appropriate for you to refer to people using family violence and children by name when asking questions about them, and to ask the questions in a natural manner, rather than interrogation.
- Throughout the assessment and management process you may explore ambivalence about the relationship with the perpetrator. This could include decisions about remaining in or leaving the relationship, as well as any barriers, fears or issues that may be worrying the victim survivor.
- When speaking to children about risk, ensure that appropriate child-friendly resources are available to help children communicate. It is also important to be mindful of your tone of voice, and to speak gently and reassuringly. Consider starting your conversation with an acknowledgement that they might feel scared and nervous about speaking to an adult they don’t know, or don’t know very well.
- Assess all children and young people in ways that are appropriate to their circumstances and age and stage of development. Primary school-aged children can be asked the simple, direct questions suggested in Appendix 7. For young people who are nearing adulthood, and where it is developmentally appropriate, a mix of the questions for adults and children might be suitable.
- Information about disclosures of abuse, such as physical/sexual abuse may require you to make a notification to Child Protection. This may be in partnership with parent/carer victim survivor, where safe to do so.
7.11.1 Level of risk: an ongoing discussion
You must communicate to the victim survivor that the nature of risk is dynamic and can change over a short period of time. For example, a person may be at lower risk if the perpetrator is incarcerated, but if they are released then the risk may escalate.
Every time you conduct a risk assessment, consider how and when the risk assessment will be reviewed. For example, review dates and follow up can be documented as part of the safety plan. Communication and information sharing are key to effectiveness in risk management. The victim survivor needs to communicate any issues of concern or likely scenarios where risk might escalate, and you must share information about the possibility of risk escalating.
Reviewing risk assessments proactively and reactively is a critical element of risk assessment and risk management.
7.12 Identifying protective factors
Reflect on protective factors from Responsibility 3.
Explore with the victim survivor what ‘protective factors’ there are for them, and any children. It is possible that such factors may mitigate the risks the person is exposed to.
While the presence of protective factors should be taken into account in making the risk assessment, it is important to plan risk management for risks which cannot be negated by a victim survivor’s actions.
7.13 Using an ecomap in comprehensive assessment
A template for completing an ecomap is in Appendix 15.
An ecomap is a useful tool to identify protective factors for victim survivors. The ecomap can act as a visual tool for both you and a victim survivor to identify social and personal relationships that may enhance safety and lessen the risk of further harm.
The ecomap can also identify services or social connections that the perpetrator may be linked in with, also see Section 7.14. This allows you to access information from these services using the Family Violence Information Sharing Scheme to strengthen risk management and safety planning for the victim survivor.
When using the ecomap with a victim survivor you can also identify services that may be missing and that can be used as a protective factor to increase a collaborative response to risk and safety.
Guidance on using an ecomap is further outlined in Responsibility 8.
7.14 Identifying relevant information about a perpetrator's circumstances
A perpetrator’s circumstances can be relevant to inform your determination of the level of risk, as well as your risk management and safety planning actions. Areas covered under protective factors can be considered as relevant to understanding the circumstances of a perpetrator.
A useful exercise may be to use the ecomap template in Appendix 15, to provide a visual diagram of the connections for a perpetrator to support your decision- making on risk management and information sharing.
7.14.1 Table 3: Identifying information relevant to a perpetrator’s circumstances
| Identifying information relevant to a perpetrator’s circumstances | |
|---|---|
| Systems intervention | Is the perpetrator:
Does the perpetrator:
|
| Practical/ Environmental | Does the perpetrator:
|
| Identity / Relationships / Community | Does the perpetrator:
|
Consider if a perpetrator’s circumstances are relevant on a case-by-case basis. This depends on the presenting risk, the pattern of risk over time identified through assessment with a victim survivor or information identified through another source.
Considerations for identifying information relevant to a perpetrator’s circumstances may be relevant to be requested and shared for an assessment or protection purpose if authorised under the Family Violence Information Sharing Scheme. For further detail, see guidance in Responsibility 6.
7.15 Determining the perpetrator/predominant aggressor and misidentification
Perpetrators and victim survivors of family violence are sometimes misidentified. Correctly identifying perpetrators of family violence is a critical component of risk assessment and risk management. Incorrect identification has serious implications for the safety and wellbeing of victim survivors in multiple and compounding ways and can affect their journey through the service system as well as the support and resources they can access. Properly assessing family violence risk in the specific context of the relationship helps ensure that perpetrators are visible, able to be challenged about the violence and are ultimately held accountable.
This guidance provides information and practice tips to ensure that perpetrators and victim survivors of family violence are correctly identified, and that any misidentification is corrected in a timely fashion. This guide builds on the information provided in the Foundation Knowledge Guide and the MARAM Framework(opens in a new window), as well as correction of information under relevant information sharing guidance in Responsibility 6.
7.15.1 Responding to perpetrators who report or are assessed to be experiencing family violence
The research and evidence demonstrate that relatively few men5 in heterosexual relationships are solely experiencing family violence (including intimate partner violence). Men are much more likely than a female partner to use a number of repeated, patterned forms of violence to dominate and control over time. This pattern is a common and known problem in heterosexual intimate partner violence but can also be present in any other form of family violence.
A perpetrator/predominant aggressor can present as a victim survivor. This presentation is often persuasive because:
- Victim survivors may use force in response to violence, as a protective behaviour. This may later be interpreted as ‘evidence’ of a pattern of violence on their part.
- Perpetrators/predominant aggressors may claim injuries that are likely to have been received from the victim (often an intimate partner) in self-defence (for example, scratches or bite marks) as evidence of experiencing family violence.
- When unable to portray the victim as the ‘sole aggressor’ and themselves as the sole person experiencing family violence, perpetrators can describe their partner’s actions (of self-defence / response to violence) as ‘tit-for-tat fighting’, perhaps by saying that ‘they give as good as they get.'
- A victim survivor experiencing fear or terror will sometimes make decisions (including the use of force), which might add to the perpetrator’s portrayal of them being hysterical or out of control.
- Descriptions of women’s behaviour, particularly, are built on the broader social history and context which is often biased, where women have often been portrayed as less credible than men. This can have particular resonance if men present as calm, charming, eloquent and ‘in control’.
The extent to which perpetrators in these situations believe that they are partly or solely the victim survivor, versus the extent to which they know they are not a person experiencing family violence, can vary.
Perpetrators who admit to using violence often try to justify or minimise their violence, or to blame their partner — perhaps for ‘provoking’ an attack or giving him ‘no way out’. They might refer to their partner as being overly-sensitive, irrational, hysterical, a danger to themselves, or even mentally ill when trying to minimise their own behaviour to others. These characterisations of women can be reinforced by social norms that do not support equitable relations between women and men.
For these reasons, in all circumstances where a man is initially assessed as or claiming to be a person experiencing family violence in the context of a heterosexual intimate partner relationship, you should refer him to a men’s family violence service for comprehensive assessment or to the Victims of Crime Helpline. His female (ex)partner must always be referred to a women’s family violence service for assessment, irrespective of whether they are thought to be the victim survivor or the perpetrator.
Keep in mind that heteronormative beliefs and incorrect assumptions can lead someone to misidentify the perpetrator or otherwise mis-characterise family violence in same-sex and/or gender diverse relationships. You should always take into account the issues outlined in assessing whether a person is using or in need of protection from family violence in the following section.
7.15.2 Assessing for the correct identification of the perpetrator (predominant aggressor)
In some circumstances, it can be difficult to establish whether a person is using violence or is in need of protection from family violence. For example, each adult in a relationship might claim to be experiencing violence from the other.
Keep in mind perpetrators construct themselves as victim survivors and report the victim survivor as either the perpetrator or equally involved in the perpetration of violence as a technique to manipulate the criminal justice system and other processes. This behaviour makes it difficult for law enforcement attending a family violence incident, and subsequently the courts and other services responding to family violence, to correctly identify who the predominant aggressor is.
It is extremely important to ensure the perpetrator/predominant aggressor is correctly identified for risk management, as a victim survivor wrongly designated as the perpetrator may not have access to needed services. Under information sharing legislation, once a person is identified as a perpetrator of family violence, relevant information about them can be shared widely without their consent.
The assessment for the person who is the perpetrator/predominant aggressor may be complex. Therefore, it is important that when risk assessment is undertaken in the context of family violence, practitioners must look beyond an individual incident to understand the history and the context of abuse.
There are a number of factors that practitioners should keep in mind when attempting to understand who is the perpetrator/predominant aggressor, including considering:
- The history of family violence between the people involved, a history of violence to other family members or previous partners and whether either party might be acting in self-defence.
- The collection of evidence from others outside the relationship (such as children and other family members).
- The language being used by the individuals (perpetrators tend to minimise or deny their involvement and are unable to sympathise with the victim survivor’s emotions, whereas victim survivors will often excuse or take responsibility for the violence).
- The nature and severity of injuries (including whether injuries may be self- inflicted).
- The power dynamic in the relationship and any vulnerabilities.
- The context in which power and control may be being established (e.g. through social, cultural or geographic isolation).
- Evidence in relation to parenting and attempts to protect (or harm) children
- The extent of fear, who is most fearful and what tactics of control, threats and stalking have occurred.
- The presence of alcohol use by perpetrators and victim survivors, as victim survivors are more likely to be arrested when they have been using alcohol even if they are not the predominant aggressor.
- Evidence of other forms of violence such as financial abuse and evidence of intimidation (text messages, online messaging and social media).
It is critical to remember that family violence involves a pattern of power and control. It is different to relationship conflict.
7.16 What's next?
Comprehensive Assessment of the level or seriousness of risk, and types of risk factors present will inform your decision-making on what to do next. Guidance on undertaking comprehensive risk management is outlined in Responsibility 8.
For example, next steps could include:
- Immediate action (calling police on 000 or making a report to Child Protection or Child FIRST/child and family services).
- Secondary consultation or information sharing (seeking or sharing) to further inform your assessment (Responsibilities 5 and 6).
- Safety planning and comprehensive risk management.
You may also seek to coordinate risk assessment and management responses with other relevant services, including ongoing risk assessment and management, covered in Responsibilities 9 and 10.
7.16.1 Document in your organisation’s record management system
- Consent and confidentiality conversation outcome.
- Each risk assessment you undertake, the level of risk for each victim survivor and reasoning.
- Adult victim survivor’s own assessment of fear, risk and safety.
- Children’s details and if present — also if children’s own assessment has been completed.
- Where and when assessment took place (telephone, meeting at office or police station etc).
- If interpreter or any other communication aid used.
- If a support person was present and their relationship to the victim survivor.
- Contact details for the victim survivor, including method of contact (such as text before call) and time it may be safe to make contact.
- Protective factors present for adult or child, and any relevant circumstances that are current or anticipated to change.
- Genogram if used to understand family structure and relationships.
- Ecomap if used to identify services involved or gaps.
- Perpetrator details and any relevant information around their circumstances that are current or anticipated to change.
1. See the MARAM Framework, definition of predominant aggressor.
2. ‘Imminence’ has been removed from the PDPA
and HRA, which now requires that a threat be only ‘serious’ before information can be shared to ‘lessen or prevent a threat to an individual’s life, health, safety or welfare’.
3. Adapted from Office of the Victorian Information Commissioner, Removal of ‘imminent’ from the IPPs and HPPs, page 4
4. ‘Imminence’ is no longer a consideration for sharing information under the Privacy and Data Protection Act 2014 and Health Records Act 2001.
5. This guidance refers to the known evidence-base relating to the experience of cis-gendered men and women in heterosexual relationships or other family relationships.
6. Vaughan, C., Davis, E., Murdolo, A., Chen, J., Murray, L., Quiazon, R., Block, K., & Warr, D. (2016).
Promoting community-led responses to violence against immigrant and refugee women in metropolitan and regional Australia. The ASPIRE Project: Research report (ANROWS Horizons 07/2016). Sydney: Australia’s National Research Organisation for Women’s Safety.
7. Segrave, M (2017) Temporary migration and family violence: An analysis of victimisation, vulnerability and support. Melbourne: School of Social Sciences, Monash University.
8. DIBP 2016: 24, see also s270.2A of the Criminal Code
9. Segrave, M (2017) Temporary migration and family violence: An analysis of victimisation, vulnerability and support.
Melbourne: School of Social Sciences, Monash University
10. Healey, Lucy. Voices Against Violence: Paper 2: Current Issues in Understanding and Responding to Violence Against Women with Disabilities (Women with Disabilities Victoria, Office of the Public Advocate and Domestic Violence Resource Centre Victoria, 2013).
11. Australian Institute of Family Studies (2016) Research Report No.35 https://aifs.gov.au/publications/elder-abuse
Responsibility 8: Comprehensive Risk Management and Safety Planning
Responsibility 8 chapter of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
Appendix 14 contains the (Adult) Comprehensive Safety Plan template.
Appendix 15 contains the ecomap template which can be used to help identify protective factors.
8. Comprehensive risk management and safety planning
8.1 Overview
This guide should be used when family violence has been established and a comprehensive risk assessment has been completed for an adult, child or young person.
This guide will assist specialist family violence practitioners to apply their advanced skills in working effectively with victim survivors, including acting to respond to the outcomes of comprehensive risk assessment and undertake comprehensive risk management, safety planning and case management.
Key capabilities
Professionals required to have knowledge of Responsibility 8, should be able to:
- Understand and apply all guidance on each of the previous responsibilities.
- Confidently and competently plan and undertake a range of risk management activities with victim survivors (adults, children and young people).
- Actively monitor family violence risk and respond to changes in risk levels through adjusting risk management activities and safety plans.
- Proactively share and gather information on family violence risk including building a shared understanding of a person’s family violence risk with other support agencies.
Specialist practitioners who use this guide should also be familiar with the Foundation Knowledge Guide, Responsibilities 1–7, and continue to Responsibilities 9–10.
Comprehensive risk management is the process of responding to identified family violence risk. It includes developing, monitoring and actioning safety plans and risk management activities with victim survivors (adults, children and young people). It also includes a focus on ongoing review and assessment (see also Responsibility 9) to respond to the dynamic nature of risk, and collaborative information sharing to understand risk/s from the perpetrator.
This chapter builds on the guidance on safety planning and identifying protective factors in Responsibility 4, with additional risk management guidance relating to:
- Safety planning in an emergency, in the home, when not ready to leave, when leaving and post separation.
- Engaging with the justice system.
- Providing appropriate risk management for Aboriginal people, or people who identify as belonging to a diverse community.
- Providing appropriate risk management for children and young people.
- Risk management is the focussing of responsibility for the risk on the perpetrator’s behaviour and supporting the victim survivor in the development of actions that may reduce harm, or in some circumstances to remove themselves from harm.
A central part of risk management is also providing a proactive response to remove or reduce threat of future harm posed by the perpetrator. Responses may be initiated by interventions of a range of services, including police or courts, and can include referral options and criminal and civil responses. The aim of responses is to reduce risk and provide support for stabilisation and recovery. This can be accomplished through responding to address safety issues and building and reinforcing protective factors.
8.2 Developing a comprehensive risk management strategy with victim survivor
The risk management process should respond appropriately to the assessed level of risk, the form of violence that is occurring, as well as likelihood/timing of risk.
An important part of safety planning and risk management is to work with the victim survivor to understand practical and structural barriers they face and to increase protective factors. You should use professional judgement and work in partnership with the victim survivor to maximise safety in ways that are collaborative, supportive and appropriate to the level of risk.
In developing a risk management plan your discussion with the victim survivor may include:
- Talking about their experience of risk and centring responsibility for the risk and its impacts on the perpetrator’s behaviour.
- Exploring the victim survivor’s self- assessment of risk posed by the perpetrator and protective factors (such as through the ecomap exercises as a discussion aide).
- Considering each child or young person and weighing the risk from the perpetrator, the impact of the abuse, and the protective factors in place for each individual child/young person, in how you plan for each individual and the family as a whole.
- Responding to your determination of the level of risk and specifically action planning for key risk factors that have been identified as increasing the likelihood of the victim survivor being killed or being seriously harmed by the perpetrator, such as high-risk factors which have changed or increased in severity or frequency which indicate escalation of risk.
- Exploring the risk management strategies the victim survivor has already tried. Identify those that continue to work and which ones are no longer helpful or need to be changed to meet current circumstances.
- Asking about the victim survivor’s experiences in engaging with services to date, and what organisations/types of services have been involved (police, health, housing, immigration, legal organisations, schools etc.).
- Exploring practical and other needs that may impact on their safety planning and ability to remain safe. These may be housing, health, education needs, children’s needs, employment, finances, relationships with family and friends, pets, and/or the potential loss of community.
- Exploring the victim survivor’s experience of violence caused by the perpetrator, or other historic trauma, and what barriers have affected their ability to leave the relationship (if they wish to do so).
- Understanding the victim survivor’s strengths, needs and goals to support their safety and recovery, and their child/ ren, in the week/month/year ahead.
- Exploring the perpetrator’s involvement with the service system and identifying areas that may hold information relevant to risk management. This could be.
- done through undertaking the ecomap activity described in Section 8.2.1 and applying it to what is known about the perpetrator’s engagement with services and community.
- Working with the victim survivor to increase protective factors should include the following considerations and a discussion of possible options (see introduction to protective factors in Responsibility 3).
Table 1: Protective Factors and Risk Management — Areas for Discussion
| Protective factor domains | Factors | Areas to cover |
|---|---|---|
| Systems intervention | Legal issues | Discuss legal needs and legal assistance which can contribute to improved safety and security including intervention orders, parole conditions and options. |
| Practical/ environmental | Safe housing | The type of accommodation the victim survivor has and its location may be important determinants of safety for adults, children and young people. Discuss the accommodation required to keep victim survivors safe. This includes immediate (e.g. emergency) and long-term accommodation. |
| Financial security (access to money, employment or education) | Income and financial security can act as barriers to leaving the relationship and/or long-term recovery. Discuss current income arrangements, income support required, and explore other sources of funds, and resources. If the victim survivor is employed, discuss whether they feel safe at work (from the perpetrator), whether their employer and co-workers are aware of the family violence and if they understand the dangerousness of the perpetrator, and or are able to provide some support. Discuss how family violence can affect the victim survivor’s work. Ask whether the perpetrator has ever threatened co-workers. | |
| Health (including mental health) | Discuss any health concerns related to physical injuries, chronic illness, general medical issues and mental health issues for all members of the family. Explore whether they have been able to access health services independently, and whether they require assistance to contact services. | |
| Immigration issues | Discuss any immigration issues. Clarify the immigration status of all family members and any additional risks this may pose. | |
| Food security | Make sure that the family has sufficient food and that food security is not being compromised due to financial security issues. | |
| Transport | It is important that victim survivors consider their safety in transport/travel. Discuss with the adult victim survivor their access to transport and explore ways of enhancing safety. With older children and young people who may travel independently, discuss ways they can stay safe. | |
| Telecommunication safety | It is important that victim survivors understand how technologies can be used by the perpetrator to increase risk, and other technologies available that may provide protection. Discuss with victim survivors what steps they can take to ‘stay safe technologically’. | |
| Connection/ sense of belonging to community and access to community | Many victim survivors have been isolated by the perpetrator and lack access to any social, familial or community support/social networks. Discuss the relationship (if any) of the perpetrator with extended family members and friends, and whether the perpetrator has ever threatened them. Discuss the social network of children and young people and consider ways to keep them connected socially while staying safe. Explore whether the victim survivor is connected or can re-connect with extended family members, friends, community and/or social networks. If there are children/young people in the family, engagement with school is protective. Discuss where they attend school, kindergarten or childcare and plan for ways to continue engagement and keep children and adult victim survivors safe in these spaces. Identify key support people to call on in an emergency. | |
| Connection to advocacy/ professional/ therapeutic services | Discuss referral options with the victim survivor and make referrals as appropriate to meet safety and recovery needs of all members of the family, including children and young people. | |
| Positive and friendly care environment (particularly for children and young people) | Structure, routine, predictability and open communication contribute to a care environment that supports resilience and recovery. Discuss with the victim survivor in what ways they have stability in their environment or what the opportunities are to establish stability. Discuss the capacity for children and young people to be engaged in educational opportunities including safe access to educational facilities without the perpetrator breaching intervention orders by approaching them at school. | |
| Strengths-based | Culture and identity | It is important to discuss with victim survivors how their Aboriginal identity or other cultural identity is valued, affirmed, and respected and whether they have opportunities to learn about, express and live out their Aboriginal or cultural identity and maintain connections with their culture. Discuss whether, for example, identity is respected and affirmed within their family or the community. |
| An individual’s personal skills and emotional resilience | Discuss with the victim survivor their strengths and acknowledge their efforts in staying safe. Explore what their coping strategies have been and what supports they may need for longer term recovery. | |
| Planning for intervention that may increase risk | Any intervention with the perpetrator can increase risk. Violence often escalates once a perpetrator’s use of violence becomes known to others. This may be a perpetrator reacting/responding to an intervention that has changed the power and control dynamic. This could be either as retaliation or an effort to regain control. An effective response to family violence should anticipate an escalation of the perpetrator’s violence in safety plans and risk management strategies. Discuss this with the victim survivor. |
8.2.1 Using an ecomap to explore protective factors
Ecomaps are used to understand an individual’s and/or family’s connections and can provide important information. You may wish to use an ecomap to better understand the victim survivor’s (adults, children and young people) circumstances. By understanding connectivity to protective factors, you can better assist with safety, risk management and recovery planning.
An ecomap template is available at Appendix 15. Ecomaps can be used in conjunction with genograms.
Developing an ecomap with a victim survivor can support the consideration of protective factors and other circumstances.
An ecomap is useful for identifying social and personal relationships of a victim survivor with their environment. The ecomap is a visual tool designed to help the victim survivor identify supports. These supports may have not been identified in the past and may contribute as a protective factor to lessen the victim survivor’s risk of further harm from the perpetrator.
Once the services and community that support a victim survivor have been identified, outline how to further collaborate with those services to manage risk and also identify any gaps where you can then increase supports. It can also be useful to establish if the perpetrator is also accessing these services, supports and community, as you would then need to manage and safety plan around this risk.
Unpack the perpetrator’s behaviours with the victim survivor and then use the tool to consider any issues that may contribute to managing risk and developing a safety plan. A practitioner may then identify a service or organisation that could provide information to enhance a safety plan or risk management strategy for the victim survivor. For example, if you have identified the victim survivor has an intervention order but are unsure if this has been served on the perpetrator. You can then use the Family Violence Information Sharing Scheme (if authorised) to request an update from the police on the current status of the intervention order.
8.3 Risk management when initial contact is limited
Initial contact with a victim survivor may be brief. However, there may still be opportunities for risk management during a short initial interaction.
If you believe a victim survivor is in immediate danger, the first responsibility is to try to ensure their safety. You may decide to:
- call the police — (ideally with victim survivor’s permission)
- call an ambulance
- arrange emergency support and assistance.
You could request or share information as authorised under the Family Violence Information Sharing Scheme, Child Information Sharing Scheme, or other relevant authorisation, about a perpetrator to support intervention and risk management.
Provide the victim survivor with immediate advice to increase their safety (e.g. information on how to escape a dangerous situation). If the victim survivor is not in immediate danger from the perpetrator, you may undertake a more detailed risk assessment and management, including safety planning. This can occur over the phone, or you could arrange a face-to-face meeting at the office, or a convenient and safe location.
8.4 Risk management for post-separation violence or where no separation is planned
The risk management plan will vary depending on whether the victim survivor has already separated, is planning a separation and/or is experiencing post-separation violence. The advice in this section is also relevant where the relationship or co-habitation is otherwise ceasing, or if this is not planned, in non- intimate partner family violence situations.
Consider the role of the formal system (police, courts, housing, family violence practitioners, children and youth workers, lawyers, drug and alcohol workers and specialist workers in relation to diversity).
If the victim survivor is planning to separate/ cease the relationship in the future, risk management requires a thorough process of preparation so that they can leave safely. Plan how to manage the other compounding risks and needs, the risks to any children, other dependents, and risks from the perpetrator, such as access to finances.
Risk management and safety planning when the victim survivor does not wish to separate/cease a relationship may be more complicated and will need more careful planning, particularly in relation to how the perpetrator will be engaged or managed (or not). Areas that should be covered in your engagement approach are outlined below.
Table 2: Engagement approach if the victim survivor does not wish to separate
| Engagement approach | Areas to cover |
|---|---|
| Respect the decision | Maintain a person-centred approach and accept the decision. If you have determined that a serious risk level is present and the victim survivor requires immediate protection, consider discussing what interventions may be required, including if there are children/young people or other dependents at risk. |
| Honest engagement | Provide information and guidance on the range of risk factors present and seriousness of risk assessed to ensure the victim survivor is well- informed in their decision making. |
| Support choices | Be clear about potential consequences of choices, such as escalation of violence from a perpetrator, and avoid expressing frustration at decisions you may not agree with. Encourage engagement and identify protective factors. |
| Expectations management | Provide information and advice which manages expectations of what your service is able to provide and how it works with other services and authorities to manage risk posed by the perpetrator. |
| Understand the context of the decision and barriers to leaving | Explore the reasons that the victim survivor is committed to the relationship. Some victim survivors experience significant barriers to leaving due to a range of supports that they may receive from a perpetrator, and are seeking support for the violence to stop, rather than leave the relationship. Other barriers may relate to one or more protective factors (see Table 1) which you may be able to work with the victim survivor to address. Reasons may relate to: Heightened fear of escalation of violence from the perpetrator if they leave. This is a serious risk factor and should be taken seriously. Risk management and safety planning should be thorough in how it responds to this. The victim survivor may believe they are responsible for violence — this needs to be addressed and responsibility placed with the perpetrator. Fear of isolation, practical barriers to leaving, fear of loneliness or responsibility for the wellbeing of the perpetrator, or of others not accepting the breaking of relationship commitment — If appropriate, consider introducing ideas about the journey of change which may normalise the idea of leaving and providing information about impacts to children. Explore options to mitigate barriers that may be preventing a decision to leave. |
| Understanding communication options and connectedness | Explore how a victim survivor is communicating with other people or services outside of the relationship, and their connection to community. Understand isolating and engagement factors and build on protective factors. |
| Identifying if the perpetrator is willing to engage | If so, provide appropriate referral and consider collaborative risk assessment and management with specialist perpetrator services. |
| Safety plan | Develop safety plans with the victim survivor (adults, children and young people) which reflect the assessed level of risk, building from existing protective factors or strengthening these, and responding to barriers identified. |
| Welfare checks | Consider if welfare checks can support monitoring of escalation or change in risk, readiness to engage in further planning or responding to other changed circumstances. When considering this option note that unexpected or unrequested welfare checks can escalate risk. |
| When to intervene (sometimes without informing victim survivor) | Whilst it is always important to consider the views of a victim survivor, this should be balanced with the determined level of risk. Consider the level of risk to the victim survivor and whether this has reached a level where intervention is required, such as ‘serious risk and requires immediate protection’. Consider the current or potential harm to child/young person victim survivors and whether this impacts on your decision to intervene. Statutory requirements may require an intervention in some circumstances. Where a victim survivor does not want you to intervene, you may still need to do so and can discuss this with them to ensure you are aware the reasons for this and how this informs your assessment and management responses. You should also weigh the likely outcome and risk that may arise from an intervention and actively plan for the intervention to respond to any potential escalation of violence from the perpetrator. |
8.5 Risk management for a victim survivor who is not ready to engage
For a range of reasons, some victim survivors may not be ready, or may refuse assistance to address family violence risk. Engagement approaches for responding to this situation are outlined below and can support future engagement and safety.
Table 3: Supporting a victim survivor who is not ready to engage
| Engagement approach | Areas to cover |
|---|---|
| Open door | Any form of engagement should be encouraged. Let them know that your service will engage with the victim survivor on their own terms and they can return at any future time. |
| Ethical engagement | Approach engagement from an ethical standpoint. Often you can’t ethically intervene without consent or engagement from a victim survivor until a threshold of risk is met (such as serious risk, including serious risk and requires immediate intervention) and/or a child/young person is at risk. |
| Collaborative risk assessment or management through other services | Victim survivors may be engaged with a range of services — there is great value in secondary consultation through these services. Consider collaboration with an engaged service to facilitate assessment, management and safety planning through another professional. |
| Risk management of perpetrator | If a victim survivor is not ready to engage, risk management of the perpetrator may still be an option. Consider the form and level of risk, and the impact any intervention may have on the victim survivor. Ensure interventions do not increase risk and/or plan to mitigate this. |
| Risk assessment through information sharing | Consider requesting or sharing information about the perpetrator to understand history and spectrum of presenting risks. |
| Communication is intervention | All opportunities to communicate information and options for assessment and management of risk are interventions and can build readiness to engage further. In some situations, you may share information about a perpetrator with a victim survivor to manage their safety. Consider how this is done and whether it may increase risk to any person. Also communicate clearly to the victim survivor that the information should only be used to manage their safety and outline risk that may be raised if used inappropriately. |
| Ensure information available | Provide links to resources for self-education, if a victim survivor is not ready to engage directly with a service. This may support future engagement. |
| Respond to ‘seeking something’ | Some victim survivors may engage and only want limited support, may not be aware of what support is available, or may be seeking information only. This should be responded to with respect for the level of engagement sought and the agency of the victim survivor. Connect victims to the information or assistance they are seeking to support future engagement. |
| Responding to barriers to engagement | Some victim survivors may have had negative experiences engaging with some services and statutory services. These can be explored and responded to, supporting future engagement and removing or reducing any potential structural barriers to access or likelihood of future experiences of discrimination. |
8.6 Risk management for a victim survivor who is not ready for assistance
When a victim survivor is assessed as being at elevated risk, serious risk and/or requiring immediate protection, but chooses not to engage in safety planning or to respond to support for risk management, you must make every effort to ensure:
- You have their contact details in case you need to contact them in the future about their safety.
- You have advised them how to contact police at ‘000’ and the state-wide crisis services.
- You have provided clear information on their current assessed level of risk.
- They have a clear understanding of their rights under the law and in relation to their own safety and that of any children/ young people involved.
- You have explained what a safety plan is and provided the option for developing a plan.
- You have documented the risk assessment.
- You have provided them with information on appropriate and relevant options for support and counselling.
If you believe the victim survivor is at serious risk and/or requires immediate protection and that the victim survivor and/ or their children (where applicable) may be seriously harmed by the perpetrator, you should inform the police or other relevant authorities. The consent of the victim survivor is not required in this instance, but you should make every effort to encourage them to plan for ways to increase their and any children’s safety, and to explain your concerns, role and responsibilities.
In some circumstances the rights and/or agency of children/young people may be compromised. It is important to keep sight of and represent the needs of children and young people as victim survivors in their own right, including when engaging with adult victim survivors.
8.7 Safety plans
A Comprehensive Safety Plan template is in Appendix 14. This plan builds on the Intermediate Safety Plan (adult) template and includes capacity to risk manage individual risk factors, identify interventions, assign actions and coordinate/collaborate with other professionals and services.
Safety planning involves discussing with a victim survivor what actions you can take or coordinate with other services to manage risk from the perpetrator and meet their needs. Plans should be documented, and identify actions, individuals and organisations responsible, and timelines. Safety plans require regular review and updates based on ongoing risk assessment.
Safety plans are developed in partnership with the victim survivor. Responsibilities for actions are shared between the victim survivor, the specialist family violence practitioner (case manager), and a range of other professionals that have a role to provide services or interventions.
The safety plan should be documented and all parties to the plan should have a copy. If it is unsafe for the victim survivor to keep a copy at home, consider an alternative place for them to keep the safety plan.
The following sections cover safety planning for an emergency, safety in the home and leaving the home. Areas that may require more in-depth planning are discussed in more detail, including access to money and financial security, intervention orders, technology safety, transport and route options, and informing people and organisations about the violence.
8.7.1 Safety planning for an emergency
Discuss the importance of emergency planning with the victim survivor, including what they and their children will do, and where they will go in case of an immediate danger. The safety plan may include the following:
- Pre-programme their phone with emergency number(s). Discuss when and how they would call police, including discussing alternatives if they can’t use their phone because of the perpetrator’s actions (such as breaking or tracking a phone).
- Set up an alert system (e.g. code or signal) for neighbours, children, family, or friends so that they know when to call police.
- Plan what to do in an emergency with the child/ren and young people, either as their own safety plan and/or as part of the adult victim survivor’s plan.
- Identify a safe place for the victim survivor to go if in danger, and how to get there. The victim survivor may go to the house of a neighbour, friend, or family member with the children, or send the children to these places
- If the victim survivor is living with the perpetrator, identify a space in the house that is lowest risk that they can move to where they may be able to prevent the perpetrator from accessing and can phone police for assistance, and which may afford an escape option.
- Identify a friend, family member or neighbour who can assist in an emergency, and how to make a plan with them to be a contact point.
- Let neighbours, co-workers and others know about the situation and what to do if the perpetrator arrives at the residence.
- Prepare a bag with key belongings — extra sets of car and house keys, clothes, essential items including medication and prescriptions.
- Store valuables and important documents (or copies) in a safe place (e.g. at the home of a family member or friend).
- Keep a copy of any intervention order at hand to show to police
- Consider alternative communication methods if victim survivors don’t have mobile phones or access to other technology (e.g. if connectivity is an issue or accessibility technology is required), and practice memorising phone numbers. Consider if a mobile phone can be provided for use in an emergency.
- Any mobile app or website with external communication could be useful as a tool in an emergency (for example, LGBTIQ victim survivors may use apps such as Grindr to get emergency support).
8.7.2 Safety in the family home
Discuss options for increasing the safety of the property if the victim survivor has separated from or is not living with the perpetrator and is staying in the family home.
These may include:
- Applying for a family violence intervention order to prevent the perpetrator from coming near the family home or places frequented by the victim survivor (adults, children and young people), including schools and childcare centres.
- Speaking to the landlord (if applicable) about security enhancements and/or changing the lease agreement.
- Changing locks to external doors, installing locks on selected internal doors, installing security chains and deadbolts, installing window locks.
- Installing security systems including alarms, lighting systems, and CCTV, and monitored alarm systems, at home and on a mobile.
- Repairing any damage to doors or windows, installing security screens on doors.
- Increasing the visibility in the front and back yards of the family home.
- Obtaining legal advice if the house is owned by the perpetrator or owned by the victim survivor and perpetrator.
8.7.3 Leaving the family home
If the victim survivor leaves the family home, they and their children may require assistance to find alternative accommodation. The type and location of accommodation will depend on the level of risk, the location of their family, friends and support services, and the connections they have with work and community (including the children’s schools).
You should discuss whether it is safe to tell the perpetrator that they are leaving as doing so can increase risk. Discuss when might be a safe time to leave. For example, when the perpetrator is not at the family home, is at work, or away, or when the victim survivor has to leave the family home for a reason perceived as ‘legitimate’ by the perpetrator, such as picking the children up from school, going to a medical appointment, or going to work.
The safety plan may require the following:
- Planning the departure, identifying items to take, organising police presence during the move, storage arrangements, removalists, child minding etc.
- Assisting the victim survivor to access emergency and/or refuge accommodation in the short term (if required).
- Technological safety such as ensuring location settings are not active/ potentially replacing a phone and having a car screened for tracking devices.
- Assisting the victim survivor to live with family members or friends in the short term.
- Ensure the victim survivor has key identity and financial documents (or copies of) including proof of relationship documents for victim survivors who may face immigration issues.
- Assistance to obtain a new property, including application for housing, and/or provision of rental assistance. Connection to tenancy advice and advocacy support.
- Assisting with relocation costs such as material aid, transport, storage.
- Applying for a family violence intervention order.
- Discuss further safety planning if there is a risk from extended family, identified third parties at risk or community members. This may be a particular risk for Aboriginal victim survivors, and victim survivors from culturally, linguistically diverse and faith communities.
- Additionally, where there is an identified threat to any third person (including if they are not within the family, but their risk is related to the family violence occurring), the third person should be notified they are assessed as at risk and they should have their safety managed.
8.7.4 Access to money and financial security
Discussing access to money is an essential part of risk management and safety planning.
The safety plan may require the following:
- Identifying ways the victim survivor can access money in an emergency. This may include ensuring access to assets such as valuable jewellery.
- Support or information to enable them to remain connected to current employment or education.
- Referring the victim survivor to financial and legal services to explore options
- Securing documentation (or copies of) which may be required to establish a financial ‘identity’ such as birth certificates, passports, and other legal documents.
- Setting up or changing access to banking arrangements.
- Assisting the victim survivor with:
- Applying for income support with Centrelink, if eligible.
- Information on obtaining child support from the perpetrator.
- Obtaining concessions for utilities and other costs as appropriate.
- Access to material aid and emergency relief.
- Accessing compensation through Victims of Crime Assistance Tribunal, if eligible.
- Accessing compensation through Workcover, Victims of Crime, TAC, Medicare, or insurance policies, if eligible.
- Advocating, as required, to obtain low- cost health services (e.g. bulk billing, mental health plan).
- Financial counsellors can provide support to access resources, applicable hardship policies and information in response to family violence, such as financial abuse and the impacts of separation and planning around financial instability.
8.7.5 Technological safety
It is important to inform the victim survivor their use of technologies can be exploited by the perpetrator to increase risk.
Discuss with victim survivors what steps they can take to ‘stay safe technologically’.
These may include:
- Acting normally if the victim survivor believes their device/s have been accessed by the perpetrator until technology safety can be re-established.
- Using computers or devices unknown to the perpetrator (e.g. in a public library or community centre/service) which can reduce the risk of perpetrators knowing the victim’s whereabouts, and other personal information.
- Obtaining/using new devices if a perpetrator has accessed an old device and this has been used to track or monitor the victim survivor.
- Creating a new email and/or Facebook account which is unknown to the perpetrator and use an anonymous username. Use strict privacy settings on new social media accounts, without identifying public photos.
- Accessing devices which send emergency messages, and/or which record events (e.g. if approached by a perpetrator or have the ability to screen-shot messages that can be saved to a file hidden under another app). Devices include BSafe, SafeTcard.
- Turning off their mobile when not in use, disabling location services, acquiring a new or additional mobile, and using landlines where possible. Children and young people’s devices should also be considered.
- Checking for spyware. Some signs of spyware may include slow battery, programs operating in the background, slower speeds, or the perpetrator knowing more about communication or movements than the victim survivor is sharing.
- Using phones in a way that does not show ‘numbers called’ on the bill and ensure that there is an answering machine to record unwanted or illegal calls by the perpetrator.
- Changing/creating passwords and PIN numbers for any protected accounts, e.g. banking. Do not use birth dates, children’s or pets’ names, favourite foods, colours or singers. If you are worried you may forget your new passwords leave a list of them at a safe place, like a trusted family member’s home.
- Setting up new accounts if they have been irreparably accessed and controlled. Always log out and sign off when not using any device.
- Checking access to devices and accounts of any children/young people, including school-based apps designed to be assessed/used by all parents/ carers, which may be used as a method of tracking an adult or child victim’s movements.
- Being selective with future contacts, including on social media, only adding actual friends and removing anyone who may not be trusted not to communicate with the perpetrator.
You can access further information on supports through smartsafe.org.au.
8.7.6 Transport and routines
Explore what access to transport victim survivors have. Discuss with the victim survivor their usual travel routes and routines and explore ways of enhancing safety.
These may include:
- Changing modes of travel.
- Always having a charger and mobile phone, and emergency contact numbers ready to dial.
- Letting friends, family, or co-workers know where the victim survivor is, and when they expect to arrive home, at work, or other places.
- Ensure safe transport of children/young people to and from school, pre-school, or childcare.
- Ensure that older children who travel independently can do so safely
- Vary travel routines. For example, not frequenting the same shopping centres and other places or changing how and when you leave home or work, or options for picking up children from childcare arrangements, any other repetitive behaviour that the perpetrator may be aware of.
8.7.7 Informing people and organisations
There may be a number of people and organisations in the lives of victim survivors that need to be aware of the risks posed by the perpetrator. This may include extended family members, friends, neighbours, workmates, people in the community and the children’s school(s). Each individual and organisation need to have a clear understanding of what actions to take if they are contacted by the victim survivor, or if they encounter the perpetrator.
The safety plan may include the following:
- Identify key people and organisations in the lives of the victim survivor and children, who can help support them and increase their safety.
- Inform neighbours, extended family members and friends. Clarify expectations and communications.
- Inform employers and co-workers, as well as education providers if applicable, about the risk and safety plan information relevant to them around monitoring and support.
- Explore options of support that an employer could offer — counselling, pay checks going to a different bank account, family violence leave, flexible working and/or security arrangements.
- Provide information to children’s school(s), including a copy of any orders designed to protect the children from the perpetrator, instructions about what to do if the perpetrator comes to pick up or see the children in contravention of the order, a photograph of the perpetrator and description of the car. Discuss not providing information that could increase risk.
8.8 Justice system
When developing risk management strategies with the victim survivor, identify, work with and advocate for effective and timely responses from justice and statutory bodies, including police and courts. This might include:
- Sharing relevant information with police that might assist with investigations and possible criminal charges against a perpetrator.
- Advocating for an intervention order to be sought against a perpetrator by police on behalf of a victim survivor (adults, children and young people) and supporting the application process, where possible (refer to Section 8.8.1).
- Sharing relevant perpetrator information with a victim survivor where it is safe to do so. This information might assist them to manage their risk, or that of their child, including assisting in obtaining an intervention order or impact decision making around child living arrangements or other contact arrangements with a perpetrator.
- Referring victim survivors to appropriate support to seek advice regarding Victims of Crime entitlements, or other financial assistance such as enforcements of fines.
- Requesting information from Corrections Victoria to determine if a perpetrator is in prison. Information may include any programs they are undertaking, their release date and assessing what risk management actions will be required to manage family violence risk.
8.8.1 Intervention orders
Intervention orders are a primary risk management strategy, as they provide legal constraints on the behaviour of the perpetrator. Intervention orders can protect a victim survivor’s children (who may also be victim survivors).
Family violence intervention orders (FVIO) are court orders made pursuant to the Family Violence Protection Act 2008 (Vic). A FVIO is a legally enforceable court order that aims to provide protection to protected persons from a family member who is perpetrating family violence.
An application can be made by: police; a victim survivor; any other person with the written consent of an adult victim survivor; a parent of a child victim survivor; a person with written consent of the parent or leave of the court; or the child over 14 years with leave of the court; or if the victim survivor (adult or child) has a guardian, the guardian or any person with leave of the court. In certain circumstance the court may make and order on their own motion for children affected by family violence. This occurs where an order for a parent is not made but the court requires the child be protected.
Types of FVIO include:
- Interim intervention orders: these are temporary orders that can be made before the respondent (the person that the order is against) is served with the application for an intervention order. The interim order does not take effect until the respondent has been served with a copy. The interim order remains in place while the application for an intervention order is before the court, the order remains in force until the court makes another order.
- Final intervention orders: these can be granted by the court if the respondent does not contest the application, or the Magistrate has heard all the evidence presented to the court. They generally expire after 12 months but can be longer.
The National Domestic Violence Order Scheme (NDVOS) allows a family violence intervention order made in one state or territory to be recognised and enforced across Australia. This includes both interim and final intervention orders, family violence safety notices and police intervention orders. For more information please refer to the Magistrates’ Court of Victoria(opens in a new window) website.
A personal safety intervention order (PSIO) is another alternative which may be more appropriate in some circumstances. A PSIO is an order made by a Magistrate to protect a person from physical or mental harm caused by someone who is not a family member. This can include where a perpetrator is using a third party as a proxy to cause harm to a victim survivor, in relation to new partners or where a victim survivor may choose a PSIO as an alternative, such as where a victim survivor who is from the LGBTIQ community does not want to publicly identify as being in a family-like relationship with the perpetrator.
Discuss with the victim survivor the advantages and possible risks of an intervention order, the available conditions and the urgency of obtaining an order.
There are common fears and misconceptions about intervention orders that you may need to address:
- Explain that taking out an order does not make the perpetrator a criminal, and that they may only face criminal proceedings for breaching the order.
- Some victim survivors may fear that an intervention order will damage the perpetrator’s chances of obtaining citizenship or permanent residency.
- Older victim survivors with children as perpetrators may be reluctant to ‘get them into trouble’.
Understand and address the victim survivor’s concerns about intervention orders and decide together whether an intervention order is an appropriate risk management strategy.
If the victim survivor wants to make an application, the following steps may be appropriate:
- Discuss with the victim survivor the possible conditions of the order.
- Assist a victim survivor to make an application for an intervention order, via a court registrar, the police, or a legal service.
- Accompany the victim survivor to court for hearing the application.
- Refer the victim survivor to a legal service which can support the application.
- Discuss with the victim survivor appropriate support services at court such as specialist family violence practitioners and targeted community supports.
- Discuss whether the victim survivor may face pressure to lift the order including possible pressure from extended family/ community.
- If the victim survivor is facing immigration issues, an intervention order can form evidence to apply for a family violence protection visa. Consult with specialists who have expertise in this area if necessary.
- Address any other concerns that may influence the victim survivor’s decisions around making an application.
You may also be supporting a victim survivor who has had the police take out an order on their behalf. In some cases, this may be against the victim survivor’s wishes. The police do not need the consent of the victim survivor if they have fears for their safety. You may need to work with the police and victim survivor to come to an agreement about the conditions and possible actions to protect the victim survivor. For example, the perpetrator may blame and threaten the victim survivor to withdraw an application, and as a safety measure the police can communicate to the perpetrator that they have made the application and not the victim survivor.
8.8.2 Victoria Police
Police have an important role in risk management strategies for victim survivors, including through their engagement with perpetrators. Police responses to family violence incidents are described in the Victoria Police Code of Practice for the Investigation of Family Violence, the Victoria Police Manual and supported by dedicated Family Violence Practice Guides and are prescribed under the Family Violence Protection Act 2008.
When police attend a family violence incident, they may intervene and take a number of actions to immediately manage risk. The following options are available to police in their investigation and response to family violence:
- Criminal option — acting under appropriate legislation to bring perpetrators before the court. An example is arresting a perpetrator for intentionally causing injury pursuant to section 18 of the Crimes Act 1958, conducting an interview pursuant to section 464 of the Act and then charging the perpetrator and determining whether bail with conditions is appropriate according to the Bail Act 1977.
- Civil option — acting according to the Family Violence Protection Act 2008. This may mean seeking an interim intervention order, an intervention order or issuing a family violence safety notice. Police may make an application to a Magistrates’ Court for an intervention order on behalf of the affected family member or assist the affected family member in seeking an appropriate order from the court.
- Referral — an option that police follow in all cases. It includes police providing advice and referring parties to appropriate services who can give necessary support and assistance as required.
Each of these options is discussed as part of a range of responses below.
Family Violence Response Model1
The model includes a structured frontline response to reports of family violence supported by a specialist response by Family Violence Investigation Units (FVIU). The FVIU detectives work closely with other family violence specialist resources including FV analysts for each FVIU and co-located Family Violence Court Liaison Officers.
Frontline Risk Assessment
The Family Violence Report (FVR), previously referred to as a family violence ‘L17 Form’, is an evidence-based risk assessment and risk management tool. The questions provide an objective guide to the risk management, with the highest risk cases being referred to the FVIU. The Family Violence Report reflects the principles in the MARAM.
The FVR looks at two elements to support case prioritisation of high-risk cases:
- The identification of family violence risk factors, including high-risk factors.
- The additional scored component of the tool which enables identification of cases that are at an increased risk of repeat family violence between the same two people within 12 months.
- It is important to note that the score, which may note a case as ‘high risk’ based on risk of repeat family violence alone, does not by itself refer to risk of an affected family member of being killed or seriously injured. Victoria Police members are trained to also consider high-risk factors in their prioritisation of cases.
Frontline response
Police attending a family violence incident manage the immediate risk to all parties, including children. There are a range of criminal and civil options available to police depending on the nature of the incident. This may include a family violence safety notice (FVSN), family violence intervention order, or an application and warrant. Steps that can occur following a FVSN or FVIO include:
- FVSNs generate an application for an intervention order, and last for up to 14 days which is usually sufficient time for a court to hear the application.
- Perpetrators who are charged may also be excluded by bail conditions.
- Police may also arrest and detain the perpetrator for questioning.
- Police may prosecute cases and may make other applications for intervention orders on behalf of a victim survivor and recommend conditions of intervention orders.
If the perpetrator cannot be located following police attendance at a family violence incident, police make arrangements to keep the victim survivor safe. This may involve assisting the victim survivor to obtain support and accompanying victim survivors to emergency accommodation.
Following investigation at an incident, the police also make referrals to specialist family violence services, and other services (e.g. Child FIRST). Referrals by police to community-based organisations are made using the FVR.
Family Violence Investigation Unit risk assessment and risk management for highest risk cases
Victoria Police has a structured case prioritisation and response model (CPRM) for family violence investigations providing the FVIUs with a consistent structured process to identify, further assess and frame management of cases where there is the highest likelihood of imminent and severe risk of future harm. The CPRM supports the operationalisation of the principles of the MARAM in a policing context. Both the FVR and the CPRM are important processes to ensure that identified risks are targeted to have the most impact.
The specialist detectives focus on investigation and collaboration in high- risk cases and will develop a proactive risk management plan for the respondent and the affected family member/s (including children).
Frontline resources and FVIUs conduct proactive risk management strategies to improve the safety of the affected family member/s and impact the behaviour of the perpetrator. Management strategies include but are not limited to the targeting of compliance with court-sanctioned conditions, engagement with the victim and the perpetrator, engagement with the FV sector for safety planning and support, and identifying and supporting those identified with accessibility needs or as particularly vulnerable in their interaction with the justice system.
Sexual Offences and Child Abuse Investigation Team (SOCIT)
Where sexual offences or child abuse is disclosed in the context of family violence, the matter will be investigated by the local specialist Sexual Offences and Child Abuse Investigation Team (SOCIT).
The mandatory organisation-wide training for the implementation of the FVR will ensure that SOCIT members have an understanding and expertise in family violence risk assessment in addition to their specialist roles in sexual offence investigations.
8.8.3 Court Services Victoria
Court Services Victoria incorporates all state court jurisdictions including Children’s Court, Magistrates’ Court, Victorian Civil and Administrative Tribunal, Victims of Crime Assistance Tribunal, Koori Court, County Court, Supreme Court and Coroner’s Court — of which family violence is a large component of cases.
Courts play an important role in the justice system by providing key decisions in accordance with the law to enhance the safety of those experiencing family violence and ensure perpetrators are held accountable for their actions. Therapeutic courts also provide additional services and support, which forms a connection to the broader family violence service sector.
Victims of Crime Assistance Tribunal:
The Victims of Crime Assistance Tribunal (VOCAT) is available for victim survivors who, as a result of a violent crime, require financial assistance. The tribunal can provide financial assistance for:
- counselling and other medical expenses
- safety-related expenses such as home security
- funeral costs
- loss of income
- special financial assistance
- dstress and dependency.
Koori Court
Koori Court is a court for Aboriginal and Torres Strait Islanders who have taken responsibility and pleaded guilty to a criminal offence. The Koori Court has been developed to reflect cultural issues and operates in a more informal way. The accused must choose to have their case heard in the Koori Court.
Court Support Services
Court Services Victoria provides a range of other services and programs at locations across the State, including:
- Specialist Family Violence Applicant and Respondent Practitioners: Practitioners provide specialist family violence support at court by engaging with a portion of victim survivors and respondents to provide non-legal process related advice, assess immediate safety risks, develop safety plans and make appropriate assessments and referrals to community agencies, Men’s Behaviour Change Program providers and court-mandated counselling services. Located at larger headquarters like Magistrates’ Courts and Melbourne Children’s Courts.
- Umalek Balit: A court-based Aboriginal family violence and victim support program, providing culturally safe and relevant service for Aboriginal and Torres Strait Islander families who attend the Melbourne and Mildura Magistrates’ Court for family violence related proceedings within the civil, criminal and Victims of Crime Assistance Tribunal jurisdictions. The service assists with addressing the specific barriers Aboriginal and Torres Strait Islander peoples may face when attending court.
- LGBTIQ Applicant and Respondent Practitioners: a service providing tailored responses to the needs of the LGBTIQ communities to support the delivery of a professional, non- discriminatory, accessible response to family violence, prioritising victim survivor safety and perpetrator accountability. Located at the Neighbourhood Justice Centre.
- Court Network: provides non-legal support, information and referral to people attending court.
- Court Integrated Support Services (CISP) and CISP Remand Outreach Program (CROP) aimed at increasing referral and access to crisis and therapeutic support services.
- Assessment and Referral Court (ARC) list: for accused persons who have a mental illness and/or cognitive impairment.
8.8.4 Corrections Victoria
Corrections Victoria provides risk management of family violence perpetrators at a number of stages, including alleged perpetrators on remand, and convicted perpetrators who are incarcerated, or living in the community (e.g. on community-based orders, parole).
Corrections Victoria aims to change the entrenched attitudes of perpetrators, that condone or normalise violence against women and other family members, through internal programs and practices, and by referring men to a Men’s Behaviour Change Program.
While perpetrators are in custody, Corrections Victoria may also monitor behaviours to help ensure that victim survivors are not threatened or abused. Corrections Victoria also has the opportunity to help ensure that perpetrators do not re-offend when released, through setting parole conditions, information sharing and other strategies. Corrections Victoria has an important role in providing information and advice particularly in relation to high-risk and recidivist offenders and attending RAMP meetings.
Once sentenced offenders are assessed by Corrections Victoria for risk of re- offending and areas of criminogenic need, appropriate interventions are designated. Corrections Victoria has developed a number of targeted programs to address family violence offending, in order to reduce the risk of offending while perpetrators are in prison or in the community and reduce the risk of re-offending when prisoners are released.
Corrections Victoria family violence strategy is based on:2
- Identifying family violence perpetrators within the Corrections system, assessing their needs, and identifying appropriate strategies. The assessment is based on tools and indicators similar to those used in the MARAM Framework.
- Providing targeted programs and services to perpetrators.
- Providing support through risk assessment and management planning to prisoners and offenders who are victim survivors.
- Changing clients’ attitudes while they are within the Corrections environment.
- Working in collaboration with other services.
8.9 Safety plans for children and young people
Much of the information in this section is adapted and refreshed from the Department of Health and Human Services resource Assessing children and young people experiencing family violence.
A safety plan template for older children and young people is at Responsibility 4, Appendix 10. Safety plans should be tailored to the circumstances and needs of all people in the family experiencing family violence. While children and young people’s safety and wellbeing is linked to the safety and wellbeing of the adult victim survivor (usually the mother), they may also have differing safety and wellbeing needs and, where it is appropriate, may need their own safety plan.
If a safety plan is developed for a child/ young person, their parent/carer (usually the mother) should be aware of it. The plan should align with the parent/carer’s safety plan. Ideally, the safety plan should be developed with the support of the parent/carer and can be an opportunity to strengthen the child or young person’s relationship with their parent/carer. Some young people will want an independently developed safety plan.
The development of a safety plan is an opportunity to talk with children and young people about their experience of living with family violence. However, you should engage sensitively, as it may create a heightened sense of anxiety for some children/young people. When a safety plan has been completed, you should allay fears and explore issues that may need to be addressed.
Children and young people will need opportunities to practice and rehearse their safety plan.
Ambivalent feelings that children/young people may have towards the perpetrator (usually but not always their father) may surface during safety planning and may also include confusing feelings about the non-offending parent/carer (usually mother). Safety planning can be an opportunity to explore these feelings.
You should tailor a safety plan to the needs and developmental stage of children and young people. It might include:
- Actions and contact numbers for how to get help safely and quickly.
- Identifying trusted people in the child/ young person’s network of relationships who can help them.
- Ensuring that they have the telephone numbers of trusted adults they can call in an emergency.
- Working with the child or young person about how to contact emergency services or a taxi service.
- Technological safety — exploring online safety and how to develop skills to safely use the internet and devices safely, including phones.
- Exploring how the young person responds when they feel fearful or unsafe (this will include for some young people the actions they could take when spending time with the perpetrator).
- Identifying services that the child or young person might like to access for ongoing help. This could include their local GP, school counsellors, youth centres, a sporting club or other activity that they are connected to or may want to be connected to in the future.
When helping the child or young person develop or rehearse their plan you might ask questions such as:
“What would you do if you were feeling scared?”
“If someone was getting hurt, how would you call the police or an ambulance?”
“Do you sometimes notice that Daddy is getting angry? What are the things that you might do when this happens?”
Safety planning with children and young people may involve you talking about your legal responsibilities to make reports to Child Protection or referrals to Child FIRST, or The Orange Door if required.
You should also explore how children and young people feel and how to act when their parent/carer is being hurt, or when they have been hurt themselves. It is important to provide a number of messages to children and young people. A helpful acronym is SAFE:
- Stay out of the fight.
- Ask for help.
- Find an adult who will listen.
- Everyone knows that it’s not your fault.
If you establish an ongoing relationship with the child or young person, you should discuss their attitudes to the use of abuse and violence in relationships and healthy ways in which people, including children/ young people, can act when they do not get what they want or when there is a problem to be solved with another person.
The table below outlines considerations for safety planning with children and young people including guidance for age and stage appropriate approaches.
Table 4: Considerations for safety planning with children and young people
| Age | Considerations including developmental factors3 | ||
|---|---|---|---|
Infants and younger children (0–5 years) | May have their safety plan contained within the adult victim survivor/carer’s plan. | When safety planning with young children (3–5 years) you should have the parent/ carer present. Affirming to the child that everyone wants them to be safe and they are not to blame are important messages for them to hear and for the parent/carer to deliver. Practice Tip: There may be times when a safety plan for a child under the age of 3 is needed. Children at this developmental level should have their parent/carer with them for this discussion. Because the child at this developmental level is often too young to openly discuss the safety plan, incorporate the child’s safety plan into that of their parent/carer. | Factors4 to consider for children developmental level years 3 to 5:
|
Older children and young people (6–18 years) | Children and young people should be included in the development of the safety plan wherever possible, including to reflect their views and wishes. The child or young person’s age and developmental stage will influence the level of involvement they have in this process. This ensures they understand the purpose of the plan and enables them to feel empowered — providing a direct response to their experience of family violence. It may not be possible to create a safety plan directly with an older child or young person, such as if the child is not present. You can develop safety plans on their behalf by talking with the parent/carer who is not using violence. It also may not be possible to create a safety plan for a child or young person in consultation with a protective parent. In this situation, it is important to still consider the impact of your planning on any parent/carer in their life (who is not using violence). | 6–11 years of age: Work together with the child to define and understand what family violence is. Affirm that everyone wants the child to be safe. If you are working with both a parent/carer and child or young person, safety planning with children at this developmental level can be more effectively done with the parent/carer present. You can use the template plan with older children and young people of this age. 12–14 years of age: The full participation of the parent/carer in developing the safety plan may not be needed or desired by the young person. You can suggest they share their safety plan with their parent/carer. You can use the template plan with older children and young people of this age. Another option is to create a simple written agreement with the young person stating what they could do and where they could go if they feel unsafe. 15–18 years of age: Young people often have a greater ability to keep themselves safe in comparison to younger children but may need help in identifying their own resources and developing a realistic safety plan for themselves. At this developmental level, full participation of parent/ carer in safety planning may not be needed or desired. Suggest they present and share their safety plan with their parent/carer. At this age, males especially may feel they can protect their mother by intervening in the violence in some way. While respecting their feelings about this, encourage discussion and highlight that this may put them and their mother at more risk — or talk about the father’s behaviour requiring system intervention and that it is not the child’s responsibility. The safety planning template for either a child and young person or adult can be used, working directly with the young person. | Factors to consider for children developmental level years 6 to 11:
Factors to consider for children developmental level years 12 to 14:
Factors to consider for youth developmental level years 15 to 18:
|
8.10 Risk management for an adolescent who is using family violence
A holistic and therapeutic response to risk management requires a high level of collaboration between services. Adolescents who use family violence may also be victim survivors of family violence and interventions needs to explore and address this.
Police, youth housing, Child Protection, disability services, alcohol and drug services, education, family services and family violence services all have a role to play with different children and young people. Several areas have specific programs for young people and their families that are designed to respond to adolescent violence. These services may also be used for secondary consultation.
Remember, family violence safety notices and holding powers can only be applied to those aged over 18 years. However, police can take out an intervention order which has conditions that respond to the behaviours being used by the child or young person.
8.11 Managing risk across the community with an intersectional lens
As per risk assessment with an intersectional lens, applying an intersectional analysis lens when managing risk means understanding that a person may have experienced a range of structural inequalities, barriers and discrimination throughout their life. These experiences will impact on their experience of family violence, how they manage their risk and safety, and their access to risk management services and responses.
A person’s identity and experiences of structural inequality and discrimination will influence how they might:
- Talk about and understand their experience of family violence, or presentations of risk.
- Experience trauma or relate family violence to their experience of barriers, structural inequality, and discrimination.
- Understand their options for service responses or who they may seek services from.
- Explain impacts of the violence they experience.
Remember
People are multi-faceted and may identify with a range of identities or experiences. You should consider each aspect and look at the person’s whole identity and experience. Think about how these inform your approach to risk management and safety planning.
Where an individual has identified as Aboriginal or belonging to a diverse community or are an older person, there are additional practice considerations which can support more effective risk management.
The guidance below addresses the most common barriers or structural inequalities experienced by Aboriginal people and people who identify as belonging to diverse communities. If you need, seek secondary consultations with appropriate targeted community support agencies to assist you to provide supportive and culturally respectful service responses.
8.12 Risk management considerations for Aboriginal victim survivors
Some additional risk management considerations for Aboriginal people may include:
- The importance of cultural safety and connections to culture and community. For example, consider how housing or intervention orders affect a victim survivor’s ability to stay connected to family and community.
- Ask what family or community members are supportive and may be able to assist if needed.
- Confidentiality can be a big concern for the victim survivor, including not wanting gossip or to be made to feel 'shame.'
- Ask if there are any concerns about calling police or emergency services. You may also need to address any fear of engaging with police or emergency services arising from previous experiences.
- Understanding they may be cautious about engaging with government, statutory authorities and justice agencies.
- Taking extra time to talk about safety for children, how you can support and advocate for them, and taking into account how distrustful the victim survivor may be about Child Protection.
8.13 Risk management consideration for diverse communities and at-risk age groups
Some additional risk management considerations for people from diverse communities and at-risk age groups (including older people) are outlined below. This is not an exhaustive list as every person’s circumstances and relationship with the perpetrator/s and their family, community and culture are different.
8.13.1 For victim survivors from culturally, linguistically diverse and faith communities
- You may need to explain how the law/ police systems work. You may also need to address any fear of engaging with police or emergency services arising from previous experiences in Australia or overseas.
- You may need to provide information/ awareness of Child Protection
- There may be multiple perpetrators — safety planning needs to address the risk for each perpetrator and how their behaviour impacts the victim survivor, individually and collectively.
- It’s important to explore the adult victim survivor’s relationship with adolescent children. Some adolescent children may be using violence.
- Discuss cultural or religious beliefs that the victim survivor believes would prevent them from leaving. There may also be community pressure, stigma, taboo etc. about leaving the relationship. Impacts of leaving may be far reaching, including on support networks, such as a perpetrator using networks to inflict violence towards family members overseas.
- Support engagement with migration agents about general issues with visa status and consider if you need to refer on or consult with them for information on family violence protection visas.
- Some victim survivors may want to return overseas; this will require exploring options, risk and safety planning. Consider if there are children who are living in Australia and seek advice around this from legal and immigration services, as applicable.
- Consider postal addresses regarding immigration information as migration correspondence may be sent to an address associated with the perpetrator.
- Consider available resources. For example, jewellery may be a woman’s only form of financial independence — if so, discuss options to take jewellery if planning to leave.
8.13.2 For LGBTIQ victim survivors
- Safety planning should consider family of origin and family of choice and how people in each family may be either involved in the family violence or are able to be a supportive person to the victim survivor.
- Specifically affirm and recognise a person’s identity, including in how you plan with them, such as connection to appropriate and safe services and how you facilitate this, such as confirming they are comfortable with you sharing their preferred pronouns in referral.
- Consider if the use of family violence is targeting an area of a person’s identity, such as their gender or sexuality and seek to respond to these specifically in risk management, where possible.
- Risk management should support the victim survivor to be further connected to support systems, where possible.
- Ask if they would like to connect to W/Respect, an integrated LGBTIQ family violence service, or consider if you should seek secondary consultation from that service.
- Ask if there are specific concerns about information sharing or barriers/access to services you can address.
- If there are children in the family, be aware of the complexity of child-caring arrangements for rainbow families. Biological parenthood is not just based on pregnancy — one partner may be an egg donor and claim biological parenthood on that basis.
- An LGBTIQ victim survivor may not feel safe to access mainstream services, including emergency services.
- Safety planning for LGBTIQ victim survivors may require creative eco- mapping of social and other supports:
- How do you feel about calling the police? Who would you feel safe talking to in an emergency?
- Where do you work? Who can you rely on in that neighbourhood?
- Discussing who is safe in the victim survivor’s family of origin or choice, or broader social network
- Discussing social contacts that the perpetrator doesn’t know (doctors, children’s play network)
- Places you can go in an emergency might include well-lit public places: restaurants, community centres, library
- Who do you know who you could stay with, and for how long?
- What other community support can you consider in emergencies — for example, a range of community and social media?
- Are there any issues relating to medication or support aides that you can address, such as where these have been restricted or removed from the victim survivor by the perpetrator.
8.13.3 For older victim survivors
- Be aware of concerns the older victim survivor may have that might impact their capacity to act on a component of the plan.
- Emergency planning may need to include an urgent application to VCAT if the appointment of a temporary guardian is needed (for example, the Public Advocate) or a temporary administrator such as the State Trustees Limited to protect property and assets.
- Consider whether a referral is needed for a specialist assessment to determine capacity by a geriatrician or GP.
- Consider whether a referral is needed to a local Aged Care Assessment Service (ACAS) to assess for aged care services — particularly if a family member is a carer who is perpetrating violence and the victim survivor needs additional supports in place to be able to be safe.
8.13.4 For victim survivors with a disability
- Consider engaging with the Department of Health and Human Services’ Disability and Family Violence Crisis Response to access crisis support for victim survivors with a disability (adults, children and young people). This can contribute to appropriate short-term funds for disability-related supports such as attendant care, hire of equipment, sign/ Auslan interpreting and transport costs.5
- Consider communication and mobility needs, and/or care requirements to determine what supports are needed. Both adult and child/young person victim survivors should be asked if they have a disability and risk management should address these needs individually.
- A safety plan should be in an accessible format if required and be readily accessible by the victim survivor. For example, if the person has limited English or a cognitive impairment, design their safety plan to address any barriers. Keep plans short and stepped out. Ask the person if there are other people in their family, friends or other supports in the community who may be able to help with executing a safety plan.
- Victim survivors who have a cognitive impairment, such as an acquired brain injury (ABI) or a potential ABI, may have difficulties in interacting with services, retaining information about safety planning, and keeping track of the services or court matter involved. Adapt support and risk management strategies, if necessary, to reflect more intensive case management work that may be required.
8.13.5 For victim survivors with mental health issues
- Family violence can exacerbate existing mental health issues for victim survivors. Symptoms can include nightmares, flashbacks, emotional detachment, insomnia, avoidance of reminders and (‘triggers’) and extreme distress when exposed to these, irritability, irritability, hyper- vigilance (watching for anger and signs of violence), memory loss, excessive startle response, clinical depression and anxiety, and loss of appetite.
- This may affect the victim survivor’s capacity to retain information, access and interact with services. Consider asking a victim survivor if you can describe any of these effects to other services to minimise potential triggers and difficulties when engaging with other services for safety planning.
- Use a trauma-informed approach in safety planning. This includes sensitively asking about current or previous trauma events, being alert to triggers and understanding that it may not always be appropriate to ask certain questions or proceed with certain discussions that may retraumatise the person.6
- Consider specific safety planning strategies for access to medication if the person is on medication, such as by having spare medication or scripts at a friend’s house.
- Be mindful of trust barriers and work to overcome these. A victim survivor with mental health issues might only trust a professional that has already assisted them. Consider discussing who the victim survivor trusts or who is in their ‘trust group.’
- Mental health professionals commonly provide letters for a person who is travelling internationally, describing mental health conditions and medication a person is taking. A similar process could be used to assist with safety planning and facilitating referral.
8.13.6 For victim survivors in rural and regional communities
- Risk management should respond to any geographical and telecommunication isolation issues. You may need to provide alternative communication methods.
- A victim survivor who is thinking about leaving the relationship or home may consider how to plan this over a period of time through other ‘legitimate’ community, service or employment pathways. For example, you can work with the victim survivor by attending the school or medical service to engage and plan for their exit.
- Risk management should consider confidentiality issues and the perceived or real influence a perpetrator may have in the community or on social and community associations. This includes possible stigma for a victim survivor who lives in a small community.
8.14 What's next?
Consistent with Responsibility 4, consider if you need to refer or seek secondary consultation with any services to support actioning the safety and risk management plan (see Responsibility 5), and record as required in the Comprehensive Safety Plan template in Appendix 14.
Specialist family violence practitioners also play a vital role in coordination of risk management responses and ongoing risk assessment and management, covered in the next chapter (Responsibilities 9 and 10).
8.14.1 Document in your organisation’s record management system
It is important that you document the following information in your service or organisation’s record management system:
- Individual safety plan for adult or child victim survivor.
- 000 and 24/7 crisis services explained, and details provided.
- Key workers or supports for the victim survivor.
- Key protective factors (trusted person identified).
- Justice system interventions (intervention orders, police statements).
- Referrals made for any additional support (i.e. InTouch, Seniors Rights).
- What organisation or service was contacted for secondary consultation to support comprehensive safety plan.
1. Victoria Police implemented a new Family Violence Response Model (FVRM) in 2019.
2. Corrections Victoria
3. Table information adapted from Safety Planning with Children and Youth: A Toolkit for Working with Children and Youth Exposed to Domestic Violence, Ministry of Justice, March 2013, British Columbia, Canada.
4. All factors taken from Cunningham, A., Baker, L., (2004) What About Me! Seeking to Understand a Child’s View of
5. Department of Health and Human Services, 2019, Disability and family violence crisis response.
6. S Fernbacher in Meadows et al, Mental Health in Australia: Collaborative Community Practice, Oxford University Press Australia (2012).
Responsibility 9: Contribute to coordinated risk management
Responsibility 9 chapter of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
9. Contribute to coordinated risk management
9.1 Overview
This guide supports professionals to understand the role of coordinated risk management, and linkages to ongoing collaborative risk management (covered under Responsibility 10), as an integral part of family violence responses.
This guidance will enable you to identify the processes required for effective multi-agency collaboration and risk management.
Multi-agency collaboration supports a shared and consistent understanding of family violence risk and enables proactive and timely interventions. Collaboration should include keeping the perpetrator’s pattern of behaviour and whereabouts in view and actively monitoring risks posed by the perpetrator. This may be done through information sharing and engagement with the victim survivor.
Key capabilities
All professionals should have knowledge of Responsibilities 9 and 10, and be able to:
- Contribute to coordinated risk management as part of a multi-disciplinary and multi-agency approach. This includes proactively requesting and sharing relevant information to facilitate coordinated risk management (see also Responsibility 6).
- Have an ongoing role in collaboratively monitoring, assessing and managing risk over time including identifying any changes in the assessed level of risk. This includes ensuring risk management and safety plans are responsive to escalation of risk and changed circumstances.
- Participate in joint action planning, coordination of responses and collaborative action including enacting and monitoring safety plans.
Where engaged, specialist family violence practitioners will provide leadership of coordinated risk management, monitoring of risk and collaborative action planning.
9.2 Coordinated risk management and ongoing risk assessment in structure professional judgement
You should continue to use Structured Professional Judgement to inform your approach to determining seriousness of risk, including through coordinated and collaborative management and ongoing risk assessment. Each element of Structured Professional Judgement can be considered collaboratively with other professionals who contribute their knowledge and expertise to the assessment process. This includes considering sharing relevant information (when authorised to do so) under the Family Violence Information Sharing Scheme, the Child Information Sharing Scheme or other relevant legislation.
Figure 1: Model of Structured Professional Judgement
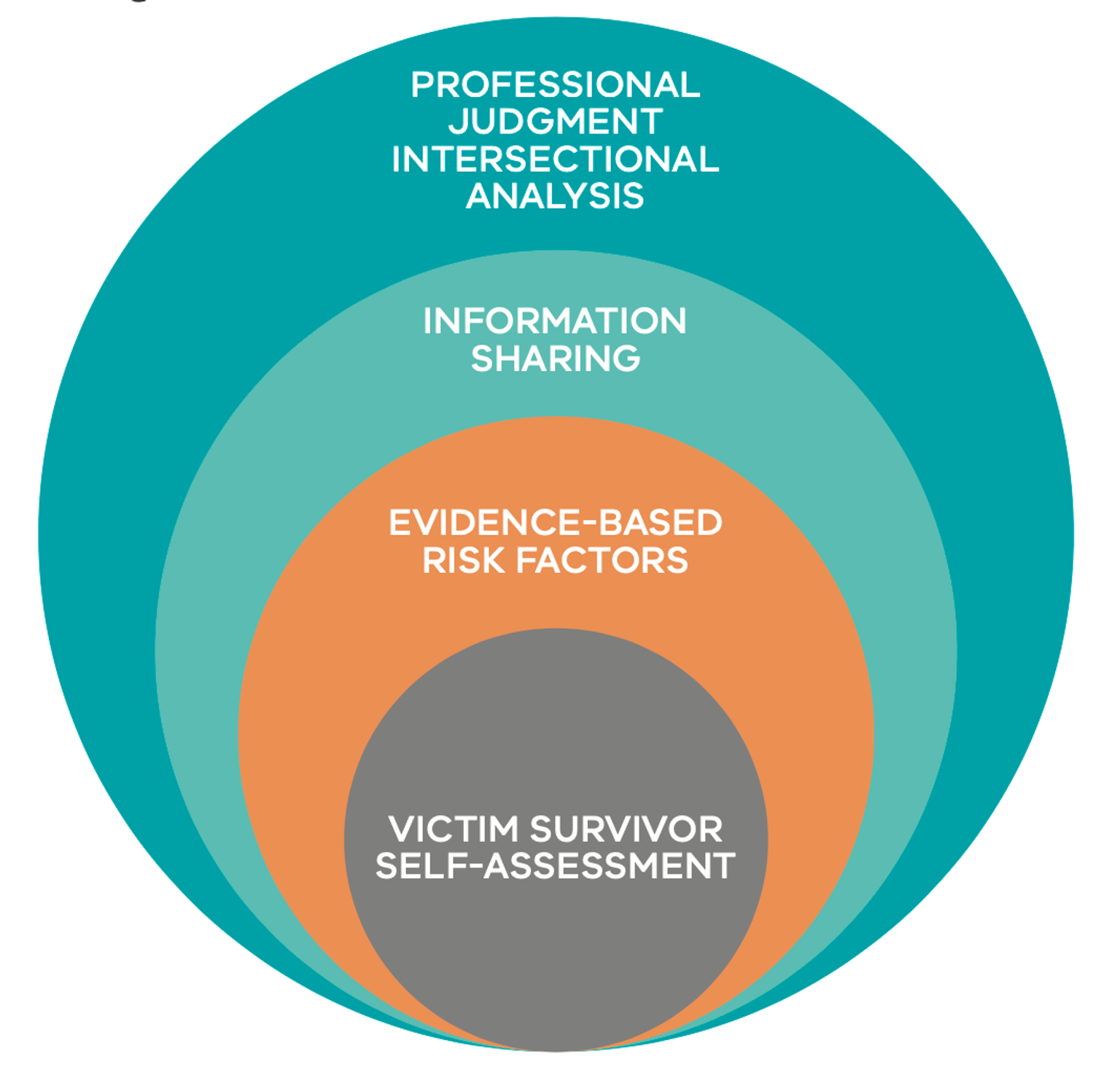
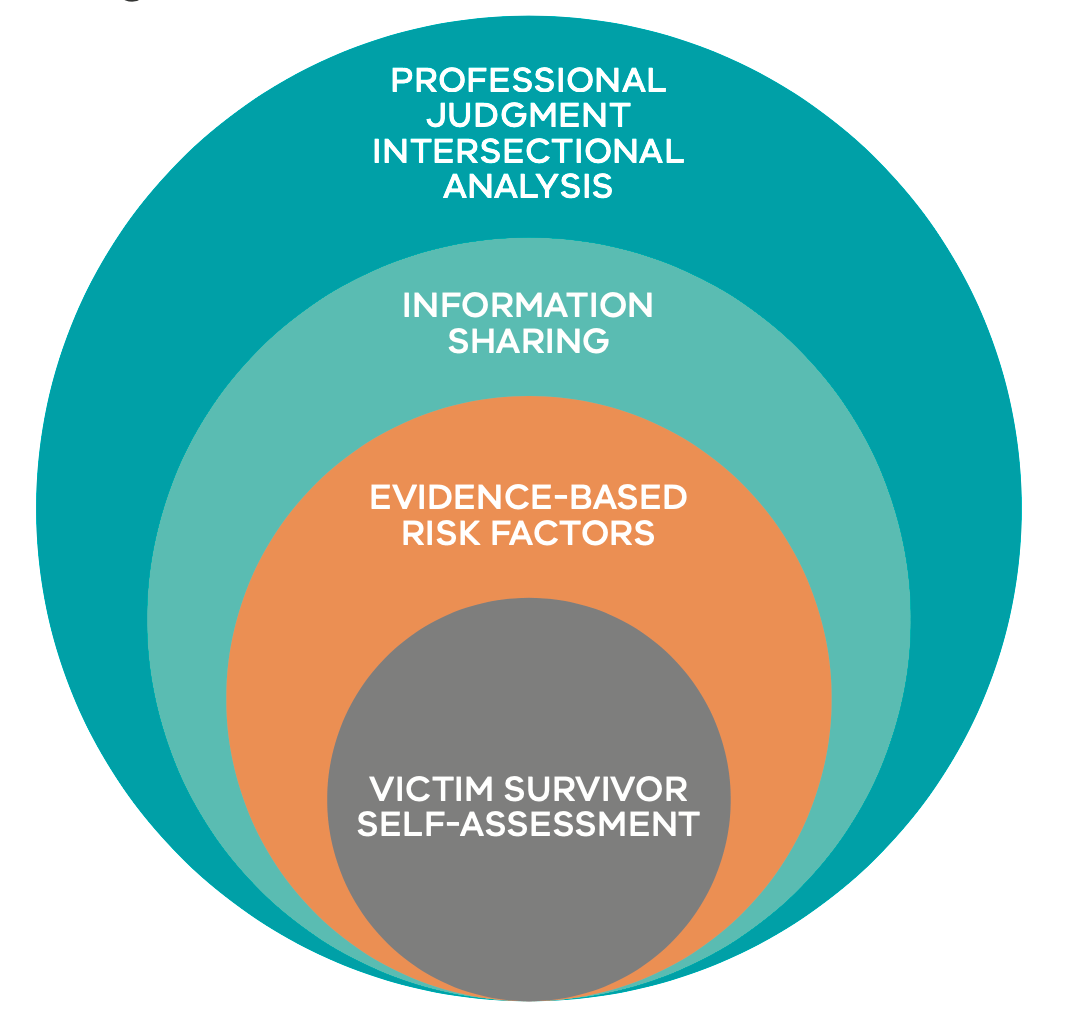{kind=link}
Review guidance in Responsibility 6 about sharing information with other services or professionals, including the relevant consent thresholds when sharing information about the perpetrator or the victim survivor. Identify key professionals and services who you may seek to engage in coordinated and collaborative risk assessment and management through consideration of the protective factors and the perpetrator circumstances. Consider using the genogram or ecomap exercises outlined in Responsibilities 7 and 8 to assist in this process.
You should consider the victim survivor’s experience and their views of the services and professionals you are engaging with or are likely to engage with. Consider what the victim survivor has discussed with you about any past or recent experiences of structural inequality, barriers or discrimination. This information should inform the approach and/or options you choose on the professionals or services you seek to engage with.
To respond to the dynamic nature of family violence, risk assessment should be integrated into the ongoing risk management process, including in coordinated processes. This is particularly relevant when considering guidance in Responsibility 10. Regularly check in with the victim survivor and seek or share information (as authorised) with organisations involved in risk assessment and management, such as the police, Corrections, and a range of community-based organisations.
9.2.1 Collaborating with a victim survivor
Reflect on person-centred practice, including across Responsibilities 3 and/ or 7 and in Section 9.3 of the Foundation Knowledge Guide.
You should inform the victim survivor that you are involved with a coordinated collaborative risk assessment and management process, when safe, reasonable and appropriate, including what services are involved. This will support a person-centred approach in your practice, as well as ensuring the victim survivor is empowered and supported to share their views.
It is critical that the victim survivor feels supported, informed and has agency of decision making regarding their options wherever possible, to support effective engagement and outcomes. Keep in mind the adult victim survivor’s self-assessment of their level of risk when determining seriousness/level of risk through Structured Professional Judgement.
You must explain the nature of ‘risk’ to the victim survivor, that it is dynamic, and can change quickly and over a short period of time. Inform the victim survivor if through your collaboration with other professionals or services you become aware of changes which may affect their level of risk.
Discuss with the victim survivor how and when the risk assessment will be reviewed. If risk has changed, review the safety plan with the victim survivor to support them to put it into action, if required.
Ask the victim survivor about any issues, concerns or scenarios where risk might escalate and seek consent to share information with other professionals about the possibility of risk escalating.
9.3 What is coordinated risk management?
Coordinated risk management is when multiple professionals and organisations act together to assess risk and plan to mitigate family violence risks for victim survivors (adults, children and young people). This includes maintaining visibility and a shared understanding of the perpetrator’s behaviours, tactics and whereabouts.
Risk assessment should be undertaken as part of any coordinated risk management approach. This involves collating and analysing information from various services or sources. Each coordination meeting should include sharing of relevant information to assess the level of risk, including information about the risk posed by the perpetrator, any specific threats or issues and the perpetrator’s circumstances.
The outcome of the risk assessment will inform the risk management strategies that are developed and actioned. Professionals involved will have a specific risk management role and actions to take. Depending on your role, this may range from information sharing only, to specific targeted actions to support a victim survivor’s safety and/or engaging or intervention with perpetrators.
The table below describes four key risk management components that are part of a coordinated response.1
Table 1: Key risk management components
|
Category |
Description and actions |
|---|---|
|
Monitoring of risk and safety |
Risk assessment is conducted continuously so that risk management and safety strategies can be adjusted over time to respond to changes in risk. Changes in escalation, frequency or presentations, as well as the circumstances of a victim survivor or perpetrator all impact the assessment of risk level. This monitoring should ideally be done by several services and professionals working together in a coordinated case management process. |
|
Facilitate engagement of support services |
Delivery of health and social services to empower and support stabilisation and recovery of victim survivors. This might include providing legal, employment, accommodation or educational opportunities and support, as well as responding to people’s broader health and wellbeing needs. Consider the domains of support outlined in the guidance on protective factors in Responsibility 3. |
|
Maintain perpetrator visibility and action interventions |
Supervision and monitoring of perpetrator’s behaviours through information sharing, coordinated risk management processes and appropriate behaviour change programs. This includes ensuring that perpetrators are aware of and comply with the conditions of intervention orders. Victim survivors’ safety is promoted by focusing attention on the behaviours of the perpetrator. |
|
Undertake safety planning |
This is the most important step in the risk management process. Safety planning aims to minimise the impact of violence, including where violence is continuing. It involves mobilising resources to actively protect against future violence, as well as reducing the severity of its impact by building resilience and supporting stabilisation. Safety planning can be performed by several professionals or services working together and should be led by or developed in partnership with the victim survivor. |
The continuum of coordination or collaboration approaches professionals and services may take is outlined below2. The approach will be determined by the circumstances and risks in each case.
Table 2: Levels of engagement in coordinated or collaborative practice
|
Levels of engagement |
|||||
|---|---|---|---|---|---|
|
Service / practice autonomy |
Collaborative practice |
Streamlined referrals |
Cooperation |
Coordination |
Integration |
|
With networking |
Formalised networking arrangements and organisational policy development |
Incident- based processes |
Including regular communication around clients and common goals |
Agreed plans and protocols |
Single system with sub- units and cross-unit accountability |
9.4 Contributing to collaborative risk management
Remember
Collaborative risk management assists professionals and services to maintain a focus and shared understanding on the actions and behaviours of a perpetrator that are causing risk.
Collaborative risk management practice can also support professionals and services to plan for the safety, stabilisation and recovery of a victim survivor.
Your role in liaising with other key services will depend on the professionals or services involved in the risk management functions. These services can be identified in reviewing an ecomap, protective factors or perpetrator’s circumstances. Further information is outlined in Section 9.2 above.
In coordinated approaches to collaborative risk management, professionals and services agree to:
-
Share and collectively analyse relevant information for ongoing risk assessment.
-
Contribute to developing risk management strategies and actions.
-
Report on the progress of specific agreed actions.
-
Notify any increases in risk using a timely system of alerts (red flags) if there is a recognised increase in the level of risk, or if a planned risk management strategy is not implemented or fails.
Specialist family violence practitioners have a lead role in collaborative risk management. These services routinely orchestrate ongoing clear communications between professionals or services providing support to the victim survivor, and to the perpetrator. This may include establishing communication protocols to facilitate information sharing and timely notification of changes in risk.
In a coordinated risk management approach, a professional or service should be nominated to lead coordination. In many cases this will be a specialist family violence service that is undertaking case management support. Some of the actions and responsibilities for this approach are outlined below.
Each professional or service should ensure they are authorised before sharing relevant information about victim survivors and perpetrators (see Responsibility 6) for risk management (protection) purposes. You should review your organisation’s policies to ensure you have authorisation to contribute to coordinated risk management, and that your actions can be resourced appropriately.
Table 3: Approach to coordinated risk management
|
Coordinated risk management processes |
Responsibility and actions |
|---|---|
|
Maintaining regular contact with the victim survivor. |
If a range of services are involved or providing support, identify who is the primary professional or service responsible for doing this. Ensure the victim survivor is informed of the outcomes of case coordination meetings and these are reflected in the safety plan. |
|
Using Structured Professional Judgement to analyse and determine the level of risk posed to the victim survivor from the perpetrator’s behaviour. |
Identify who will record and maintain documentation of coordinated risk assessment. |
| Receiving notification if a family violence incident occurs. | Message that it is a shared responsibility to notify other services if relevant to their role. |
| Ensuring other organisations update and share information when they consider that the level of risk has changed. | Message that it is a shared responsibility to notify other services if risk or circumstances have changed for a victim survivor or perpetrator. Notify if these changes may impact the risk management response or actions of other professionals or services, or the shared understanding of the level of risk. |
| Monitoring the completion of actions against a safety plan. |
Identify who will monitor and follow up to ensure agreed actions are completed. Identify who will review the safety plan to update, as required. |
| Obtaining confirmation from professionals or services when victim survivor needs have been met. | Identify who will monitor and follow up to ensure agreed actions are completed. |
|
Obtaining information from other sources about the perpetrator (whereabouts, activities, behaviours). |
Identify who will coordinate information requests if other sources of information are identified as relevant, and document requests in case management systems. |
| Maintaining a list of organisations and the type of information they hold (e.g. perpetrator whereabouts, activities, attitudes and behaviours) and expected reports to you. | Collectively review the victim survivor’s protective factors or ecomap, the perpetrator’s circumstances, or undertake the ecomap exercise for a perpetrator in Responsibility 8. |
| Establishing communication protocols with key organisations that can monitor perpetrator’s behaviour, risk and circumstances. |
Consider collectively if this is supported by existing protocols or whether new protocols should be established. Depending on the professionals or services involved, and the timeframe for the case coordination, this may be through existing ongoing protocols, or ad hoc and less formal protocols for a time limited period or an individual case. Consider if the perpetrator’s circumstances support identification of professionals or services who have access to relevant information (e.g. housing services, Centrelink, family services, drug and alcohol, and mental health services, men’s services). Schools can potentially provide critical information about changes for the child / young person and their family and should be included where appropriate. |
|
Receiving notification when designated safety plan actions are completed. |
Message that it is a shared responsibility to notify when actions are completed and identify who will update records and documentation to indicate that this has occurred. |
9.4.1 Document in your organisation’s record management system
It is important that you document the following information in your service or organisation’s record management system:
-
Services involved in the collaboration of risk management and safety planning.
-
Actions required of each service.
-
Additional or new information surfacing from collaboration.
-
When case coordination meetings are held.
-
The responsibility of ongoing risk assessment.
-
The victim survivor being informed of any updates.
9.5 COORDINATION OF RISK MANAGEMENT
9.5.1 Case coordination
Specialist family violence practitioners will often lead and conduct case coordination. Case coordination may include meetings to review risk and develop and organise risk management actions. In other instances, specialist family violence workers may participate in case coordination led by other professionals or services. These processes are important for building trust, clarifying roles and responsibilities, developing mutual understanding and knowledge of effective risk management strategies, developing creative action plans, and strengthening mutual accountability.
Case coordination draws on the collective wisdom of multiple professionals and services. It can include opinions and professional judgement, in addition to information which is shared between professionals and services. This collaborative process increases knowledge about the perpetrator’s whereabouts and level of risk they pose, facilitates more creative risk management strategies, and is responsive to changes in the level of risk.
Professionals taking part in a multi-agency coordinated approach to risk management should:3
-
Contribute knowledge, expertise and actions to develop a jointly developed risk management plan for victim survivors.
-
Try to reach consensus in decision making about risk and management responses.
-
Enable proactive outreach and risk management of perpetrators. For example, professionals and services should have a plan to reduce or remove risk and for specialist practitioners to engage with the perpetrator about their abusive behaviour, whilst keeping them connected and in view.
-
Assign service or professional responsibility for working directly with victim survivors on risk and safety, as well as other needs that may strengthen protective factors.
-
Focus on lessening the risk of further violence and providing ongoing support to victim survivors.
-
Ensure that meeting minutes are taken of case conferences and that safety plans are documented.
-
Record all follow-up actions such as timeframes, responsibility for tasks, monitoring and reviewing case, risk management and safety plans and give a copy to coordination team members, as relevant.
9.5.2 Risk Assessment and Management Panels (RAMP)
The Risk Assessment and Management Panel (RAMP) program is a multi-agency coordinated response to family violence that increases the collective capacity and effectiveness of the service system to identify and respond to perpetrators, and to hold them responsible and accountable for their violence and abuse. RAMP is victim survivor and child-centred approach that focuses on ensuring that the perpetrator is held solely responsible and accountable for their abusive and violent behaviour.
RAMP is a key initiative to improve responses of serious threats to victim survivors of family violence. The primary aims of the RAMP program are to:
-
Increase the safety of victim survivors of family violence who are experiencing a serious threat.
-
Lessen serious threat posed by perpetrators and increase the accountability of perpetrators.
-
Increase agency accountability and strengthen the capacity of the service system to achieve the above two aims.
A RAMP is a formally convened meeting, held at a local area level, of key agencies and organisations that contribute to the safety of victim survivors (usually women) experiencing serious threat from family violence and where the normal service cannot mitigate the risk.
RAMPs provide a common approach for cases assessed as at highest risk and are convened regularly to:
-
Share relevant information about the threat posed by the perpetrator in order to undertake a comprehensive assessment that identifies the level of risk and impact of family violence on a victim survivor and their children.
-
To develop coordinated action plans across participating agencies to lessen or prevent serious threat posed by the perpetrator to a victim survivor’s life, health, safety or welfare.
9.5.3 RAMP structure
There are 18 RAMPs operating across Victoria. The RAMP structure includes two chairs, a coordinator, core members and associate members. Each RAMP is jointly chaired by a senior staff member of Victoria Police and a senior manager from a specialist family violence service.
RAMP members are essential to the effective operation of the RAMP and are required to attend all meetings.
Core members of RAMPs include one representative from each of the following:
- Victoria Police (co-chair plus a senior police member form Family Violence Investigation Unit).
- Specialist family violence service (coordinator, co-chair plus a representative senior family violence practitioner).
- Local Area Department of Health and Human Services Child Protection.
- Local Area Department of Health and Human Services Housing.
- Men’s family violence services (case management or Men’s Behaviour Change Program).
- Child FIRST/Family Support Agency/The Orange Door (Support and Safety Hub).
- Mental health.
- Drug and alcohol services.
- Community corrections.
In addition, an associate member can be invited to attend RAMP for a specific case. For example, Centrelink or a school principal. Special associate member status is given to all Aboriginal Community Controlled Organisations (ACCOs) to ensure that RAMP employs a culturally safe and appropriate decision-making process for all cases involving people that identify as Aboriginal.
Victim survivors and perpetrators do not attend RAMP meetings, as this has the potential to compromise the victim survivor’s safety. Individual cases are presented at RAMPs by an advocate, generally a case worker representing the interests of the victim survivor and their children under threat. This person may be the victim survivor’s case manager (for example, from a family violence service or a mental health service) or a representative of the referring organisation (for example, Victoria Police).
Where the adult or child victim survivor identifies as being Aboriginal or from a diverse cultural background, consideration must be given for attendance by an agency or organisation that is able to represent their cultural needs.
9.5.4 How to make a referral to a RAMP
Cases which are referred to a RAMP must involve a victim survivor of family violence (including any children who may also be victim survivors) experiencing a serious threat / serious risk of being killed or serious injury. A perpetrator can only be referred to a RAMP in the context of a ‘case’, where there is a serious threat/risk to a victim survivor of family violence. It is important to remember that:
-
Referral to a RAMP is not a first or sole response to serious threat.
-
Any agency, organisation or professional who identifies an adult and children at immediate risk of serious threat of harm from family violence should immediately notify Victoria Police and contact the local specialist family violence service based on the victim survivor’s current place of residence.
-
A RAMP referral does not substitute any agency’s usual functions or responsibilities.
-
Information sharing of relevant information may also occur prior to a RAMP to assess or manage serious threat. A RAMP referral is made when it is considered that the development of a coordinated multi-agency plan is required, in addition to the ‘normal’ service system response a victim survivor requires to reduce or remove the threat posed by the perpetrator and to support monitoring to keep the perpetrator in view.
Typically, the three major referrers to RAMP are:
- victim survivor specialist family violence services
- The Orange Door
- Victoria Police
Cases are identified as serious risk via a MARAM-based assessment and the Victoria Police family violence report (L17) respectively. However, any practitioner who identifies a victim survivor at serious risk from a serious threat of being killed or seriously injured can contact their local specialist family violence service to provide information to support a RAMP referral.
1. Adapted from Albuquerque, M., Basinskaite, D., Martins, M. M., Mira, R., Pautasso, E., Polzin, I., ... Wiemann, S. (2013). European manual for risk assessment. Göttingen, Germany: E-Maria Partnership
2. Adapted from Jane Wangmann, ‘Examining Integrated Models to Respond to Domestic Violence’ (Report Prepared for Sutherland Shire Domestic Violence Committee, 2006) 4.
3. Adapted from Ministry of Justice, 2017, Family Violence Risk Assessment and Management Framework, New Zealand Government, page 41.
Responsibility 10: Family Violence: Collaborate for ongoing risk assessment and risk management
Responsibility 10 chapter of the Family Violence Multi Agency Risk Assessment and Management Framework: Practice Guides.
Download and print the PDF or read the accessible version:
10. Family violence: collaborate for ongoing risk assessment and risk management
10.1 Overview
Due to the dynamic nature of family violence, family violence risk assessment and management is a continuous process. The aim of professionals, services and organisations working together is to understand family violence risk and undertake joint risk management strategies.
The safety of victim survivors (adults, children and young people) and visibility and accountability of perpetrators is the primary aim of family violence multi- agency collaborative practices.
Good practice in multi-agency responses involves:1
- A focus on victim survivor safety and perpetrator accountability.
- Inclusion of all family violence related services at all levels (service delivery, policy, problem solving).
- Shared missions, aims, values, and approaches to family violence and protocols.
- A collaborative approach to policy development and memoranda of understanding.
- Willingness to change organisational practice to meet the aims of the response and develop operating procedures to achieve this.
- Practices and protocols which ensure cultural safety, inclusivity and access and equity issues.
- Information sharing.
- Adequately trained and professional staff.
- Senior level commitment and coordination.
- Workable governance structure, with coordination, steering, troubleshooting and monitoring functions.
- Transparency, particularly in regard to outcomes, including criminal justice system outcomes, and evaluation processes.
- Commitment to continual self-auditing, enabled through data collection and monitoring processes.
- Regular and frequent coordinated case management meetings.
- Identification of service gaps (e.g. children’s counselling) and development of new services to address them.
10.2 System-level collaboration and development
Collaboration at an individual professional level must be supported by organisations’ policies and procedures, including agreements for working in collaborative, multi-agency processes.
Professionals and services should understand their role in responding to family violence and how their service/ organisation participates in and contributes to a broader network of services responding to family violence.
Services and organisations have a responsibility to work jointly to address family violence risk and undertake family violence risk assessment, risk management, planning and review.
Services should have the following2:
- Established strategies for working collaboratively with key partners within their local area to improve outcomes for victim survivors.
- Strong links with local youth services, multicultural services, Aboriginal and Torres Strait Islander services, services that specialise in working with people with disability, as well as LGBTIQ specialist services.
- Formal partnerships built on a mutual understanding of roles and responsibilities and the shared goal of increased safety of victim survivors and families.
- Established mechanisms that delineate referral processes and pathways.
- Services regularly meet to discuss how to best support victim survivors and appropriately share information to enable comprehensive risk assessment and consideration of matters relating to the safety and wellbeing of victim survivors.
- Regular participation in inter-agency and network meetings and are part of community networks and partnerships.
Further information on organisational responsibilities can be found in the Organisational Embedding Guide.
Having a range of professionals working collaboratively allows for interpretation and discussion. More informed decisions can then be made on appropriate family violence risk assessment and management responses.
Multi-agency collaboration is the key to building an integrated community response to family violence.
The functions of multi-agency collaboration include:3
- Improving communication between individuals and organisations.
- Improving each participant’s understanding of ‘the problem’ by exposing them to a variety of perspectives.
- Improving decision making on collective strategies and individual cases based on more complete information.
- Facilitating consistent and philosophically coherent policy development across services.
- Improving the accountability of each network participant to victim survivors.
- Facilitating evaluation of the collective response.
- Facilitating broader cultural change.
10.3 The role specialist family violence services
Specialist family violence services lead family violence system development. Their role includes strengthening the identification of family violence, referral pathways from multiple organisations and workforces, bringing professionals and services together, and promoting a shared understanding and commitment to family violence risk assessment and management.
Specialist family violence services may also:
- Identify gaps and barriers in the family violence service system.
- Support professionals and services to analyse their response to family violence from the perspective of ensuring victim survivor safety.
- Support services and organisations to make changes to practice or policy to align with the MARAM Framework.
1. Adapted from Australian Domestic & Family Violence Clearinghouse, 2008, Multi-Agency Responses to Domestic Violence — From Good Ideas to Good Practice., Newsletter No 33, page 4.
2. Adapted from Government of New South Wales, Good Practice Guidelines for the Domestic and Family Violence Sector in NSW.
3. Domestic Violence & Incest Resource Centre Victoria, 2004, Developing Integrated Responses to Family Violence in Victoria — Issues and Directions. Page 24.