Download and print the PDF or read the accessible version:
9. Contribute to coordinated risk management
9.1 Overview
This guide supports professionals to understand the role of coordinated risk management, and linkages to ongoing collaborative risk management (covered under Responsibility 10), as an integral part of family violence responses.
This guidance will enable you to identify the processes required for effective multi-agency collaboration and risk management.
Multi-agency collaboration supports a shared and consistent understanding of family violence risk and enables proactive and timely interventions. Collaboration should include keeping the perpetrator’s pattern of behaviour and whereabouts in view and actively monitoring risks posed by the perpetrator. This may be done through information sharing and engagement with the victim survivor.
Key capabilities
All professionals should have knowledge of Responsibilities 9 and 10, and be able to:
- Contribute to coordinated risk management as part of a multi-disciplinary and multi-agency approach. This includes proactively requesting and sharing relevant information to facilitate coordinated risk management (see also Responsibility 6).
- Have an ongoing role in collaboratively monitoring, assessing and managing risk over time including identifying any changes in the assessed level of risk. This includes ensuring risk management and safety plans are responsive to escalation of risk and changed circumstances.
- Participate in joint action planning, coordination of responses and collaborative action including enacting and monitoring safety plans.
Where engaged, specialist family violence practitioners will provide leadership of coordinated risk management, monitoring of risk and collaborative action planning.
9.2 Coordinated risk management and ongoing risk assessment in structure professional judgement
You should continue to use Structured Professional Judgement to inform your approach to determining seriousness of risk, including through coordinated and collaborative management and ongoing risk assessment. Each element of Structured Professional Judgement can be considered collaboratively with other professionals who contribute their knowledge and expertise to the assessment process. This includes considering sharing relevant information (when authorised to do so) under the Family Violence Information Sharing Scheme, the Child Information Sharing Scheme or other relevant legislation.
Figure 1: Model of Structured Professional Judgement
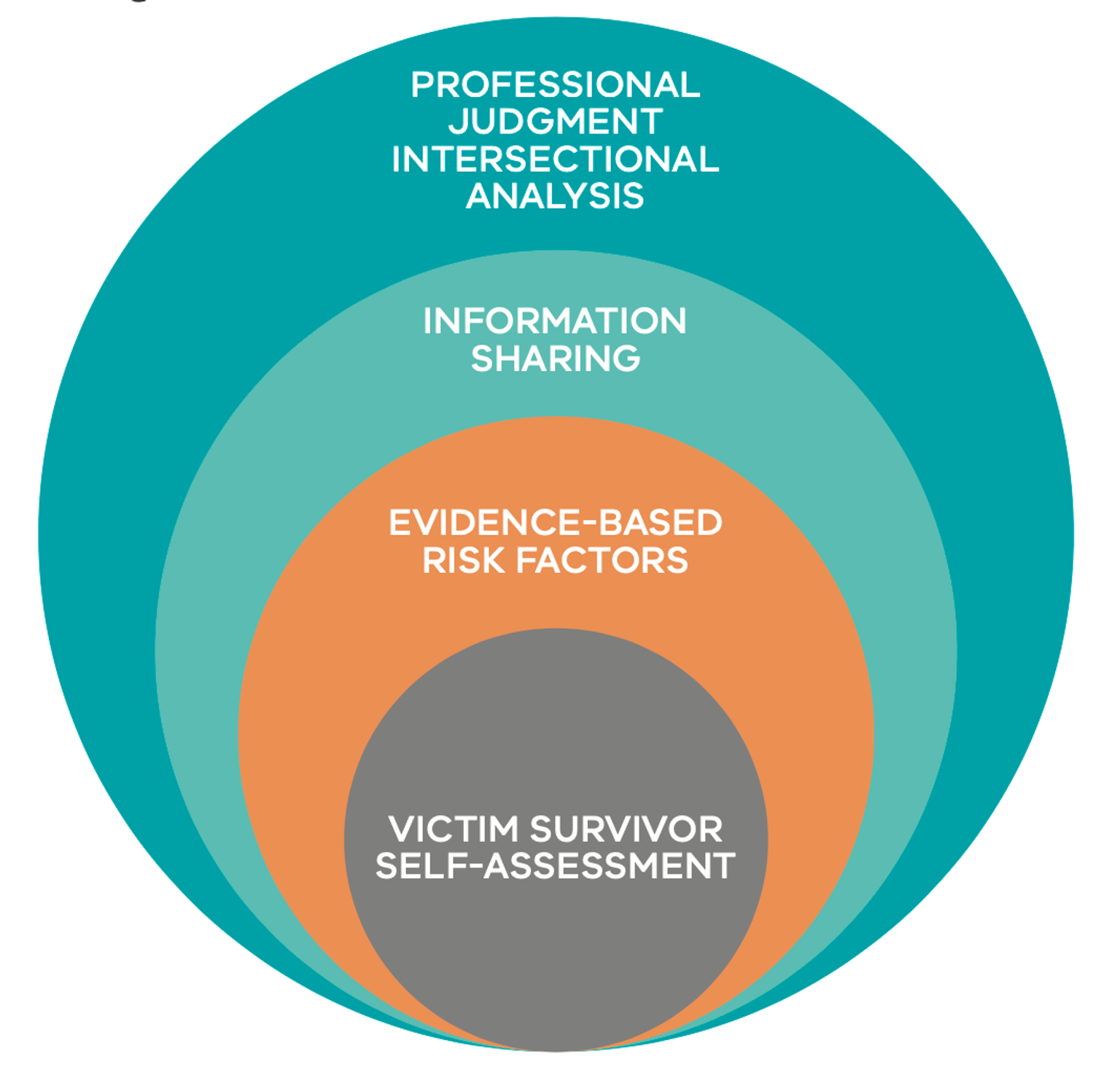
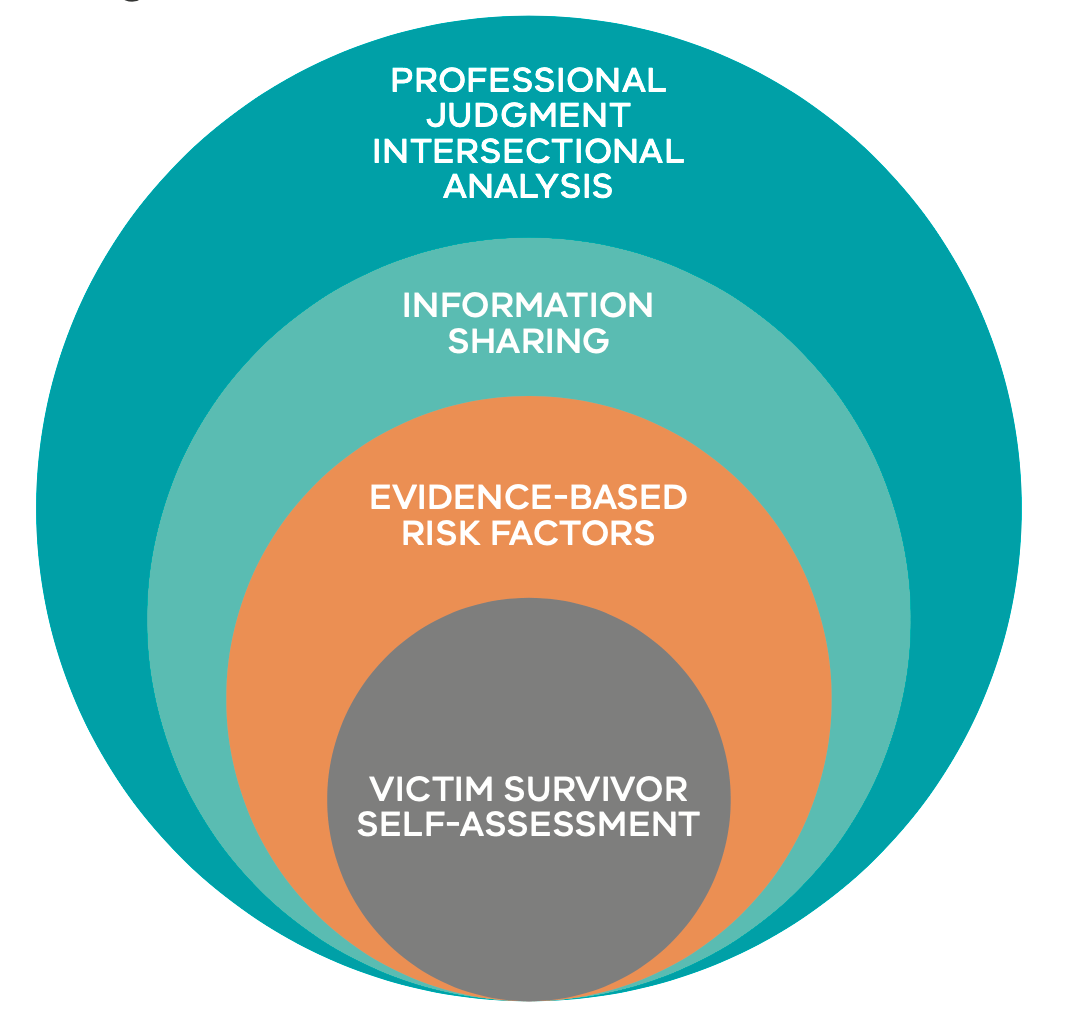{kind=link}
Review guidance in Responsibility 6 about sharing information with other services or professionals, including the relevant consent thresholds when sharing information about the perpetrator or the victim survivor. Identify key professionals and services who you may seek to engage in coordinated and collaborative risk assessment and management through consideration of the protective factors and the perpetrator circumstances. Consider using the genogram or ecomap exercises outlined in Responsibilities 7 and 8 to assist in this process.
You should consider the victim survivor’s experience and their views of the services and professionals you are engaging with or are likely to engage with. Consider what the victim survivor has discussed with you about any past or recent experiences of structural inequality, barriers or discrimination. This information should inform the approach and/or options you choose on the professionals or services you seek to engage with.
To respond to the dynamic nature of family violence, risk assessment should be integrated into the ongoing risk management process, including in coordinated processes. This is particularly relevant when considering guidance in Responsibility 10. Regularly check in with the victim survivor and seek or share information (as authorised) with organisations involved in risk assessment and management, such as the police, Corrections, and a range of community-based organisations.
9.2.1 Collaborating with a victim survivor
Reflect on person-centred practice, including across Responsibilities 3 and/ or 7 and in Section 9.3 of the Foundation Knowledge Guide.
You should inform the victim survivor that you are involved with a coordinated collaborative risk assessment and management process, when safe, reasonable and appropriate, including what services are involved. This will support a person-centred approach in your practice, as well as ensuring the victim survivor is empowered and supported to share their views.
It is critical that the victim survivor feels supported, informed and has agency of decision making regarding their options wherever possible, to support effective engagement and outcomes. Keep in mind the adult victim survivor’s self-assessment of their level of risk when determining seriousness/level of risk through Structured Professional Judgement.
You must explain the nature of ‘risk’ to the victim survivor, that it is dynamic, and can change quickly and over a short period of time. Inform the victim survivor if through your collaboration with other professionals or services you become aware of changes which may affect their level of risk.
Discuss with the victim survivor how and when the risk assessment will be reviewed. If risk has changed, review the safety plan with the victim survivor to support them to put it into action, if required.
Ask the victim survivor about any issues, concerns or scenarios where risk might escalate and seek consent to share information with other professionals about the possibility of risk escalating.
9.3 What is coordinated risk management?
Coordinated risk management is when multiple professionals and organisations act together to assess risk and plan to mitigate family violence risks for victim survivors (adults, children and young people). This includes maintaining visibility and a shared understanding of the perpetrator’s behaviours, tactics and whereabouts.
Risk assessment should be undertaken as part of any coordinated risk management approach. This involves collating and analysing information from various services or sources. Each coordination meeting should include sharing of relevant information to assess the level of risk, including information about the risk posed by the perpetrator, any specific threats or issues and the perpetrator’s circumstances.
The outcome of the risk assessment will inform the risk management strategies that are developed and actioned. Professionals involved will have a specific risk management role and actions to take. Depending on your role, this may range from information sharing only, to specific targeted actions to support a victim survivor’s safety and/or engaging or intervention with perpetrators.
The table below describes four key risk management components that are part of a coordinated response.1
Table 1: Key risk management components
|
Category |
Description and actions |
|---|---|
|
Monitoring of risk and safety |
Risk assessment is conducted continuously so that risk management and safety strategies can be adjusted over time to respond to changes in risk. Changes in escalation, frequency or presentations, as well as the circumstances of a victim survivor or perpetrator all impact the assessment of risk level. This monitoring should ideally be done by several services and professionals working together in a coordinated case management process. |
|
Facilitate engagement of support services |
Delivery of health and social services to empower and support stabilisation and recovery of victim survivors. This might include providing legal, employment, accommodation or educational opportunities and support, as well as responding to people’s broader health and wellbeing needs. Consider the domains of support outlined in the guidance on protective factors in Responsibility 3. |
|
Maintain perpetrator visibility and action interventions |
Supervision and monitoring of perpetrator’s behaviours through information sharing, coordinated risk management processes and appropriate behaviour change programs. This includes ensuring that perpetrators are aware of and comply with the conditions of intervention orders. Victim survivors’ safety is promoted by focusing attention on the behaviours of the perpetrator. |
|
Undertake safety planning |
This is the most important step in the risk management process. Safety planning aims to minimise the impact of violence, including where violence is continuing. It involves mobilising resources to actively protect against future violence, as well as reducing the severity of its impact by building resilience and supporting stabilisation. Safety planning can be performed by several professionals or services working together and should be led by or developed in partnership with the victim survivor. |
The continuum of coordination or collaboration approaches professionals and services may take is outlined below2. The approach will be determined by the circumstances and risks in each case.
Table 2: Levels of engagement in coordinated or collaborative practice
|
Levels of engagement |
|||||
|---|---|---|---|---|---|
|
Service / practice autonomy |
Collaborative practice |
Streamlined referrals |
Cooperation |
Coordination |
Integration |
|
With networking |
Formalised networking arrangements and organisational policy development |
Incident- based processes |
Including regular communication around clients and common goals |
Agreed plans and protocols |
Single system with sub- units and cross-unit accountability |
9.4 Contributing to collaborative risk management
Remember
Collaborative risk management assists professionals and services to maintain a focus and shared understanding on the actions and behaviours of a perpetrator that are causing risk.
Collaborative risk management practice can also support professionals and services to plan for the safety, stabilisation and recovery of a victim survivor.
Your role in liaising with other key services will depend on the professionals or services involved in the risk management functions. These services can be identified in reviewing an ecomap, protective factors or perpetrator’s circumstances. Further information is outlined in Section 9.2 above.
In coordinated approaches to collaborative risk management, professionals and services agree to:
-
Share and collectively analyse relevant information for ongoing risk assessment.
-
Contribute to developing risk management strategies and actions.
-
Report on the progress of specific agreed actions.
-
Notify any increases in risk using a timely system of alerts (red flags) if there is a recognised increase in the level of risk, or if a planned risk management strategy is not implemented or fails.
Specialist family violence practitioners have a lead role in collaborative risk management. These services routinely orchestrate ongoing clear communications between professionals or services providing support to the victim survivor, and to the perpetrator. This may include establishing communication protocols to facilitate information sharing and timely notification of changes in risk.
In a coordinated risk management approach, a professional or service should be nominated to lead coordination. In many cases this will be a specialist family violence service that is undertaking case management support. Some of the actions and responsibilities for this approach are outlined below.
Each professional or service should ensure they are authorised before sharing relevant information about victim survivors and perpetrators (see Responsibility 6) for risk management (protection) purposes. You should review your organisation’s policies to ensure you have authorisation to contribute to coordinated risk management, and that your actions can be resourced appropriately.
Table 3: Approach to coordinated risk management
|
Coordinated risk management processes |
Responsibility and actions |
|---|---|
|
Maintaining regular contact with the victim survivor. |
If a range of services are involved or providing support, identify who is the primary professional or service responsible for doing this. Ensure the victim survivor is informed of the outcomes of case coordination meetings and these are reflected in the safety plan. |
|
Using Structured Professional Judgement to analyse and determine the level of risk posed to the victim survivor from the perpetrator’s behaviour. |
Identify who will record and maintain documentation of coordinated risk assessment. |
| Receiving notification if a family violence incident occurs. | Message that it is a shared responsibility to notify other services if relevant to their role. |
| Ensuring other organisations update and share information when they consider that the level of risk has changed. | Message that it is a shared responsibility to notify other services if risk or circumstances have changed for a victim survivor or perpetrator. Notify if these changes may impact the risk management response or actions of other professionals or services, or the shared understanding of the level of risk. |
| Monitoring the completion of actions against a safety plan. |
Identify who will monitor and follow up to ensure agreed actions are completed. Identify who will review the safety plan to update, as required. |
| Obtaining confirmation from professionals or services when victim survivor needs have been met. | Identify who will monitor and follow up to ensure agreed actions are completed. |
|
Obtaining information from other sources about the perpetrator (whereabouts, activities, behaviours). |
Identify who will coordinate information requests if other sources of information are identified as relevant, and document requests in case management systems. |
| Maintaining a list of organisations and the type of information they hold (e.g. perpetrator whereabouts, activities, attitudes and behaviours) and expected reports to you. | Collectively review the victim survivor’s protective factors or ecomap, the perpetrator’s circumstances, or undertake the ecomap exercise for a perpetrator in Responsibility 8. |
| Establishing communication protocols with key organisations that can monitor perpetrator’s behaviour, risk and circumstances. |
Consider collectively if this is supported by existing protocols or whether new protocols should be established. Depending on the professionals or services involved, and the timeframe for the case coordination, this may be through existing ongoing protocols, or ad hoc and less formal protocols for a time limited period or an individual case. Consider if the perpetrator’s circumstances support identification of professionals or services who have access to relevant information (e.g. housing services, Centrelink, family services, drug and alcohol, and mental health services, men’s services). Schools can potentially provide critical information about changes for the child / young person and their family and should be included where appropriate. |
|
Receiving notification when designated safety plan actions are completed. |
Message that it is a shared responsibility to notify when actions are completed and identify who will update records and documentation to indicate that this has occurred. |
9.4.1 Document in your organisation’s record management system
It is important that you document the following information in your service or organisation’s record management system:
-
Services involved in the collaboration of risk management and safety planning.
-
Actions required of each service.
-
Additional or new information surfacing from collaboration.
-
When case coordination meetings are held.
-
The responsibility of ongoing risk assessment.
-
The victim survivor being informed of any updates.
9.5 COORDINATION OF RISK MANAGEMENT
9.5.1 Case coordination
Specialist family violence practitioners will often lead and conduct case coordination. Case coordination may include meetings to review risk and develop and organise risk management actions. In other instances, specialist family violence workers may participate in case coordination led by other professionals or services. These processes are important for building trust, clarifying roles and responsibilities, developing mutual understanding and knowledge of effective risk management strategies, developing creative action plans, and strengthening mutual accountability.
Case coordination draws on the collective wisdom of multiple professionals and services. It can include opinions and professional judgement, in addition to information which is shared between professionals and services. This collaborative process increases knowledge about the perpetrator’s whereabouts and level of risk they pose, facilitates more creative risk management strategies, and is responsive to changes in the level of risk.
Professionals taking part in a multi-agency coordinated approach to risk management should:3
-
Contribute knowledge, expertise and actions to develop a jointly developed risk management plan for victim survivors.
-
Try to reach consensus in decision making about risk and management responses.
-
Enable proactive outreach and risk management of perpetrators. For example, professionals and services should have a plan to reduce or remove risk and for specialist practitioners to engage with the perpetrator about their abusive behaviour, whilst keeping them connected and in view.
-
Assign service or professional responsibility for working directly with victim survivors on risk and safety, as well as other needs that may strengthen protective factors.
-
Focus on lessening the risk of further violence and providing ongoing support to victim survivors.
-
Ensure that meeting minutes are taken of case conferences and that safety plans are documented.
-
Record all follow-up actions such as timeframes, responsibility for tasks, monitoring and reviewing case, risk management and safety plans and give a copy to coordination team members, as relevant.
9.5.2 Risk Assessment and Management Panels (RAMP)
The Risk Assessment and Management Panel (RAMP) program is a multi-agency coordinated response to family violence that increases the collective capacity and effectiveness of the service system to identify and respond to perpetrators, and to hold them responsible and accountable for their violence and abuse. RAMP is victim survivor and child-centred approach that focuses on ensuring that the perpetrator is held solely responsible and accountable for their abusive and violent behaviour.
RAMP is a key initiative to improve responses of serious threats to victim survivors of family violence. The primary aims of the RAMP program are to:
-
Increase the safety of victim survivors of family violence who are experiencing a serious threat.
-
Lessen serious threat posed by perpetrators and increase the accountability of perpetrators.
-
Increase agency accountability and strengthen the capacity of the service system to achieve the above two aims.
A RAMP is a formally convened meeting, held at a local area level, of key agencies and organisations that contribute to the safety of victim survivors (usually women) experiencing serious threat from family violence and where the normal service cannot mitigate the risk.
RAMPs provide a common approach for cases assessed as at highest risk and are convened regularly to:
-
Share relevant information about the threat posed by the perpetrator in order to undertake a comprehensive assessment that identifies the level of risk and impact of family violence on a victim survivor and their children.
-
To develop coordinated action plans across participating agencies to lessen or prevent serious threat posed by the perpetrator to a victim survivor’s life, health, safety or welfare.
9.5.3 RAMP structure
There are 18 RAMPs operating across Victoria. The RAMP structure includes two chairs, a coordinator, core members and associate members. Each RAMP is jointly chaired by a senior staff member of Victoria Police and a senior manager from a specialist family violence service.
RAMP members are essential to the effective operation of the RAMP and are required to attend all meetings.
Core members of RAMPs include one representative from each of the following:
- Victoria Police (co-chair plus a senior police member form Family Violence Investigation Unit).
- Specialist family violence service (coordinator, co-chair plus a representative senior family violence practitioner).
- Local Area Department of Health and Human Services Child Protection.
- Local Area Department of Health and Human Services Housing.
- Men’s family violence services (case management or Men’s Behaviour Change Program).
- Child FIRST/Family Support Agency/The Orange Door (Support and Safety Hub).
- Mental health.
- Drug and alcohol services.
- Community corrections.
In addition, an associate member can be invited to attend RAMP for a specific case. For example, Centrelink or a school principal. Special associate member status is given to all Aboriginal Community Controlled Organisations (ACCOs) to ensure that RAMP employs a culturally safe and appropriate decision-making process for all cases involving people that identify as Aboriginal.
Victim survivors and perpetrators do not attend RAMP meetings, as this has the potential to compromise the victim survivor’s safety. Individual cases are presented at RAMPs by an advocate, generally a case worker representing the interests of the victim survivor and their children under threat. This person may be the victim survivor’s case manager (for example, from a family violence service or a mental health service) or a representative of the referring organisation (for example, Victoria Police).
Where the adult or child victim survivor identifies as being Aboriginal or from a diverse cultural background, consideration must be given for attendance by an agency or organisation that is able to represent their cultural needs.
9.5.4 How to make a referral to a RAMP
Cases which are referred to a RAMP must involve a victim survivor of family violence (including any children who may also be victim survivors) experiencing a serious threat / serious risk of being killed or serious injury. A perpetrator can only be referred to a RAMP in the context of a ‘case’, where there is a serious threat/risk to a victim survivor of family violence. It is important to remember that:
-
Referral to a RAMP is not a first or sole response to serious threat.
-
Any agency, organisation or professional who identifies an adult and children at immediate risk of serious threat of harm from family violence should immediately notify Victoria Police and contact the local specialist family violence service based on the victim survivor’s current place of residence.
-
A RAMP referral does not substitute any agency’s usual functions or responsibilities.
-
Information sharing of relevant information may also occur prior to a RAMP to assess or manage serious threat. A RAMP referral is made when it is considered that the development of a coordinated multi-agency plan is required, in addition to the ‘normal’ service system response a victim survivor requires to reduce or remove the threat posed by the perpetrator and to support monitoring to keep the perpetrator in view.
Typically, the three major referrers to RAMP are:
- victim survivor specialist family violence services
- The Orange Door
- Victoria Police
Cases are identified as serious risk via a MARAM-based assessment and the Victoria Police family violence report (L17) respectively. However, any practitioner who identifies a victim survivor at serious risk from a serious threat of being killed or seriously injured can contact their local specialist family violence service to provide information to support a RAMP referral.
1. Adapted from Albuquerque, M., Basinskaite, D., Martins, M. M., Mira, R., Pautasso, E., Polzin, I., ... Wiemann, S. (2013). European manual for risk assessment. Göttingen, Germany: E-Maria Partnership
2. Adapted from Jane Wangmann, ‘Examining Integrated Models to Respond to Domestic Violence’ (Report Prepared for Sutherland Shire Domestic Violence Committee, 2006) 4.
3. Adapted from Ministry of Justice, 2017, Family Violence Risk Assessment and Management Framework, New Zealand Government, page 41.
Updated