To what extent is The Orange Door visible, accessible and safe (including culturally safe) at each site?
Physical location and physical accessibility
The Support and Safety Hubs: statewide concept envisaged that The Orange Door would be accessible through an area-based access network that includes a primary physical community-based site as well as outreach or mobile Hub practitioners who can engage with people where they feel comfortable.[1] The Orange Door was intended to initially operate from 9am to 5pm Monday to Friday (with the intention of including extended hours – although this is not part of initial establishment at this stage). The physical sites are designed to have a reception area where members of the public can make enquiries. Perpetrators are not to be encouraged to come to The Orange Door as their first contact with the service system, and Men’s Behaviour Change programs are not delivered at The Orange Door (physical) site.[2]
The locations of The Orange Door have been chosen for their visibility and proximity to public transport and other community services/institutions. Table 4 provides a summary of the features of The Orange Door locations.
Table 4: Physical features of The Orange Door physical locations
| DHHS area (primary location) |
Location and visibility |
Public transport accessibility |
Proximity to other services |
|
Barwon (Geelong) |
Prominently located on a main street retail shopping strip |
Approximately 10 minutes’ walk from Geelong V/Line station (servicing a single train line) and closer to multiple bus lines |
Located nearby other community services. The Geelong Magistrates’ Court is around 10 minutes’ walk away |
|
Bayside Peninsula (Frankston) |
Prominently located on a main street retail shopping strip |
Approximately 10 minutes’ walk from Frankston station (servicing a single train line) and closer to multiple bus lines |
Colocated with other community services. The Frankston Magistrates’ Court is located around 10 minutes’ walk away |
|
North Eastern Melbourne (Heidelberg) |
Shopfront within a small suburban shopping mall |
Approximately 10 minutes’ walk from Heidelberg station (servicing a single train line) and closer to multiple bus lines |
Located nearby other community services. The Heidelberg Magistrates’ Court is around five minutes’ walk away |
|
Mallee (Mildura) |
Shopfront on a secondary street one back from the main street |
Approximately five minutes’ walk from a bus stop servicing parts of Mildura and surrounding towns, and 10 minutes’ walk from the intercity bus station |
Located across the road from other community services. The Mildura Magistrates’ Court is around five minutes’ walk away |
The Orange Door primary locations appear to be situated in relatively visible and accessible areas, with access to public transport. Evidence from fieldwork indicates concerns that it may be difficult for some clients to access the locations from public transport if they did not live nearby a train line. Despite the limited number of clients interviewed for the evaluation, a number of clients stated that physical accessibility was often challenging, even for those with a car. For example, client feedback indicated that they were not able to find disability parking near one physical site of The Orange Door.
However, it was accepted that the locations chosen were the most acceptable locations within the DHHS area, and that increasing accessibility would require greater outreach or opening of formal access points. The opening of access points is planned and will come online in terms of the planned roll out.
Other community services are located near all of The Orange Door locations, however certain areas (The Orange Door in Mallee, Bayside Peninsula Area and the staff based at Colac) appear to have stronger connections with and between nearby organisations based on their proximity. Moreover, evidence from fieldwork indicates that it was not uncommon for clients to access The Orange Door straight from the nearby courts, and this was particularly the case in NEMA.
The Orange Door buildings themselves have all been fitted out similarly, with a consistent ‘look and feel’ for the reception and client areas. This involves a large open wooden desk at the reception area, lockable rooms for interviews and lounge areas (in all locations, this is situated behind a sliding door that can be electronically locked). Opinions differed on the appropriateness of the reception and client area:
One client interviewed compared it to sitting in their lounge room and commented that their children were given things to do and eat.
Some staff expressed concern that the reception area was not able to be easily secured in case of a disturbance or aggressive person. Some of the CSOs – who sit behind the reception desk – reported they felt exposed by the open desk, and indicated that clients sometimes did not appear to know where to stand and needed to come to their side of the desk watching them input their details on their computer[3]. Furthermore, in Bayside Peninsula, the electronic sliding doors used to separate the reception area from the foyer and the client lounge area from the reception area were not able to be closed quickly to stop someone getting through.
'Families I know would be intimidated coming into a building like this, the fear of them taking their children away, whether they’re going to be treated with respect. The physical space isn’t safe to be able to deal with trauma, people are having to wear sunglasses inside.' – Practitioner interview
There has been a small number of situations where physical security issues have been raised and subsequently improved at The Orange Door. For example, we understand there were security concerns relating to CCTV screens inside interview rooms where perpetrators can be interviewed and that the screens have now been turned off in response to these initial concerns.
A separate office section for practitioners and FSV staff is accessible from the client area through locked door. Most staff view the office spaces as broadly suitable and that it was ‘their home’. It is a positive finding that some staff are reporting a sense of belonging to the space so early in the roll out of The Orange Door. Localised concerns around hot desk arrangements, comfort factors (e.g. blinds) and site specific safety issues were raised during fieldwork and are to be expected in the very early stages of fit-out of a new premise.
Access options
Apart from physical access to The Orange Door, the service model specified a number of options to access its services. The model outlines how the Service System Navigator plays a role in developing access options within the local context of the area.
Telephone and email access
Each of The Orange Door areas has implemented its telephone (toll-free number provided by FSV) and email access slightly differently. These two access options have been established and are operational in each of the four locations. The primary concern regarding these options has been how to manage demand. One example of this is that in BPA, practitioners reported that clients had told them that phone calls that were not answered rung out – that is, there was no voicemail system or other overflow mechanism such as a central call centre to capture them.
Outreach
Practitioners are expected to undertake outreach with clients and families in settings where they feel most comfortable. The extent of outreach undertaken by practitioners at this point in time differed based on their primary specialty of practice:
- Child and family wellbeing practitioners are experienced in undertaking home visits as part of their previous practice in Child FIRST, Child Protection or other family services. They reported that they still preferred to undertake home visits as part of the assessment and planning stage where possible, although time constraints meant that this was not always possible.
- Family violence-focused practitioners reported reluctance about home visits due to risk of violence from the perpetrator.
- Home visits were a regular part of Aboriginal practitioners’ work. They reported that they would often accompany other workers and that ‘showing their face’ often led to increased engagement from the family.
- Community-based Child Protection practitioners also undertake a large number of home visits. Primarily this was to ensure the families understood the possibility of formal engagement by Child Protection were concerns not addressed.
- There was some evidence of emerging practice in one area of police accompanying practitioners on home visits to try and engage families earlier.
Practitioners reported being unsure if the way in which outreach and home visits were occurring at this early stage of implementation were appropriate and in line with the intended The Orange Door model. Further definition (and/or reconfirmation) of the outreach role will be required once The Orange Door is through the initial stages of establishment to ensure the outreach access option is developed.
Alternative physical access options, including out posted workers
The concept envisaged that a limited number of The Orange Door practitioners will operate as out-posted workers from their employing organisations with the capacity to deliver the full Orange Door foundational service offering.[4] While this has not yet been formally established as intended in the model, alternative access points have already emerged.
- Swan Hill: 2.5 FTE The Orange Door practitioners were working in Swan Hill at the time of the evaluation fieldwork. During the morning screening meeting held in Mildura, those cases that enter The Orange Door from Swan Hill or surrounding areas are assigned to the practitioners in Swan Hill. The physical location is situated within the offices of the Mallee Domestic Violence Service (MDVS).
- Colac: The physical location is within Colac Area Health, which is an integrated health service that provides medical and allied health services as well as community services. The existing service model means that there are well-established working relationships between practitioners at The Orange Door and other colocated services such as family violence case management services, family counselling, paediatricians, mental health, drug and alcohol services.
- As the service is located within a broader integrated service model, The Orange Door has been able to engage with external services in Colac Area Health to promote the services of The Orange Door, and build the capacity of more mainstream services to identify family violence and refer to The Orange Door.
- The close proximity of these services within the one physical site makes it easier for informal information sharing such as following up on a referral. Practitioners in Colac are more easily able to seek information from other services such as medical health records and homelessness as they are all located on site.
- An alternative pathway for L17 reports involving an Aboriginal Affected Family Member (AFM), where L17s originating from Mildura and Robinvale are sent directly to Meminar (an Aboriginal service), while also being visible to The Orange Door staff. This is based on the Koori police family violence protocol, which was in place prior to The Orange Door.[5]
At the time of the evaluation fieldwork, BPA and NEMA only operate at their primary locations. There is evidence that alternative access points are evolving based on local needs as envisaged in The Orange Door concept.
Service System Navigator
The Service System Navigator (SSN) role (employed by FSV) is currently the key networking element in The Orange Door, designed to:
- establish and maintain practice interface agreements with key services in the area, as well as partnering with the local service sector to identify opportunities to address local service gaps
- resolve system and navigation access issues and work with the governance structure to effect change
- monitor progress of service engagement, connections and service capacity and provide advice to internal and external stakeholders regarding service interfaces
Evidence from the evaluation identified that the role is not currently functioning as intended in these early stages.
- Many practitioners reported having little if any interaction with the SSN (some did not know which person was in the role at their area of The Orange Door) and were not clear what the value of this role was. This is in many ways to be expected during these early months where the focus of The Orange Door is on initiating service delivery, operationalising the model and ensuring basic business processes were in place.
- Other practitioners stated that it was useful for the SSN to be in place before The Orange Door commenced operations, but that until the client pathways had been clearly defined by FSV through the SSN in each area, it was difficult for the practitioners to establish connections.
- Some SSNs appeared to lead the operationalisation of integrated practice in the absence of other practical clarification. This was not a responsibility identified as part of the SSN role and may be specific to the early implementation phase and start–up demands.
- There was concern about whether the SSN role had appropriate authority to create the partnerships on behalf of The Orange Door, particularly because outside stakeholders and community sectors had no reference to what the SSN role was (at that point in time). While there are position descriptions that define these roles, at an operational level at this early stage of implementation, it is unclear to the workforce if the SSN and Hub Manager have the same authority or decision making level within The Orange Door (despite being at the same VPS grade levels).
- In the service model, the SSN forms part of a feedback loop with services and advice to practitioners on the service system. There was no evidence during fieldwork of this feedback loop occurring at this early stage of implementation. Partially, this is as the ‘review and monitoring’ stage of the service model has not been implemented (see Section 4.1.1), however, this is may also be due to the SSN’s inability to have an understanding of demand of at this early stage of operations.
Safe and inclusive environment
Cultural safety and accessibility for clients and workforce
The concept paper specifies that The Orange Door will:
- Support the choice and self-determination of Aboriginal people by recognising their needs and working closely with Aboriginal services, including Aboriginal Controlled Community Organisations (ACCOs) where present.
- Actively tailor their services to the needs of multicultural communities in their local area, including access to interpreter services and employing workers from multicultural communities.
- Have the capacity to recognise and meet the specific needs of people with disabilities, people from LGBTIQ communities, older people experiencing violence and adolescents who use violence in the home.
The Orange Door has made a commitment to inclusive practice for Aboriginal communities. This has included the establishment of an Aboriginal Practice Leader role. The feedback from practitioners has been very positive about the role of the Aboriginal Practice Leaders. There is not data available at this point in time to determine whether the current FTE resourcing for Aboriginal Practice Leads in each area is sufficient to meet demand, or how cultural safety practice is being embedded through their work to The Orange Door workforce. Practitioners are clear when they should be engaging with the Aboriginal Practice Leader for Aboriginal clients and are grateful for the guidance and support:
'We try to identify Aboriginal clients very quickly, but then I will go on to ask what mob they’re from… Indigenous workers will have fantastic engagement skills and that’s important because people are very fearful in that community because of what happened historically.' – Aboriginal Practice Lead interview
'The work around Aboriginal clients is amazing – everyone is consulting [practitioner name] on Aboriginal clients, and now [the Aboriginal service] is saying we can’t cope with our demand, we’ve never had so many.'
'I went on a [home] visit with a non-Indigenous worker and she [the client] didn’t open the door to her but as soon as I showed my face, she opened the door.'[6] – Practitioner interview
There is also evidence that practitioners at The Orange Door are using the Aboriginal Practice Leaders to support their practice.
In terms of Aboriginal inclusive practice within The Orange Door, there are still fundamental differences in Aboriginal practice that have not been resolved and cannot be resolved through cultural awareness programs alone. For example, the language and approach to engaging with perpetrators is very different between mainstream and the varied approaches in Aboriginal practice, which may not even use the term perpetrator or the concepts of ‘holding to account’:
'For non-Aboriginal people, they name the things they do, whereas we have always done practice without naming it.' – Practitioner interview
'Working with the whole family – it’s an Aboriginal approach, an Aboriginal AFM will always ask for help from the partner.' – Practitioner interview
While cultural safety programs can cover content such as the impact of colonisation, disadvantage and trans-generational trauma, there is room for improvement to build the skills and capacity of non-Aboriginal practitioners to engage with Aboriginal clients. One of the key mechanisms to build this capacity and resolve differences in Aboriginal practice with other service’s practice is to embed Aboriginal voices and engagement from the outset of service design and delivery. FSV has the foundations for this in the development of a range of guidance and policy documents including Everybody Matters: inclusion and equity statement and the toolkit and resources being developed through the Intersectionality Capacity building project.
Consideration of cultural safety includes not only working with clients but the safety of the Aboriginal workforce within The Orange Door. The feedback from the Aboriginal workforce in The Orange Door is mixed.
'All the Indigenous people here migrate together, sometimes we don’t feel safe in this space, to be you… The presence of more diverse people would make us feel safer.'
'As an Aboriginal woman, I feel FSV and the Manager here are very respectful to Aboriginal culture, from the heart, not just in a tokenistic way.' – Aboriginal practitioner interview
Box 3: Quantitative data on Aboriginal people accessing The Orange Door
The Orange Door appears to be receiving a relatively consistent number of cases involving Aboriginal people as shown in Figure 10. Across all The Orange Door areas, 7.3 per cent of clients are recorded as Aboriginal.
Figure 10: Number of clients identified as Aboriginal and/or Torres Strait Islander by The Orange Door area, July – December 2018
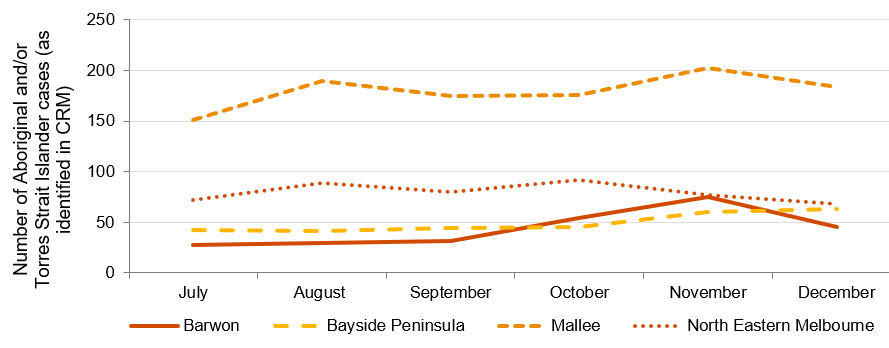
Source: PwC analysis of CRM data provided by FSV. Note that The Orange Door commenced in NEMA in July 2018. There is a large proportion of clients where Aboriginal status is not recorded (‘blank’) so the actual number may be higher.
Based on the available data and evidence from fieldwork, it appears that Aboriginal and/or Torres Strait Islander clients are using The Orange Door; however they may be under-recorded in the CRM.
Cultural safety and accessibility for clients with diverse needs
Evaluation of the accessibility of The Orange Door by clients from the diverse cohorts identified by the RCFV is limited at this point in time. This is because there is currently inadequate data on clients with diverse needs recorded on the CRM and because of the small number of client interviews conducted for the evaluation. It is important that The Orange Door can meet the specific and intersecting needs of clients with a disability, older people (particularly those experiencing family violence in the form of elder abuse), LGBTIQ clients, children and young people (either as victim survivors of family violence, perpetrators of family violence and/or those subject to child wellbeing concerns) are responded to by The Orange Door. As mentioned above, FSV has the foundations for this in the development of a range of guidance and policy documents including Everybody Matters: Inclusion and Equity Statement and the toolkit and resources being developed through the Intersectionality Capacity building project.
There was limited evaluation data available on the cultural safety and accessibility of The Orange Door for clients with diverse needs at this stage. The data that was available was generated through qualitative interviewing of The Orange Door workforce and through stakeholder interviews with peak organisations. This data indicates that attempts are being made by The Orange Door to tailor responses to clients with diverse needs. Examples include assigning practitioners to clients of a similar cultural background, or referring clients to services that are known to have culturally tailored programs. However further investigation is required to make evaluative judgements on the accessibility and cultural safety of The Orange Door for these clients. It is important to acknowledge that the findings from this evaluation are that we have insufficient data to evaluate how culturally safe and accessible The Orange Door is at this point in time – this does not mean that The Orange Door is not providing accessible and safe services, rather that we have insufficient evidence to make an evaluative judgement.
Box 4: Availability of quantitative data on clients with other diverse needs
At this point in time, quantitative data relating to clients with other diverse needs, such as the elderly and LGBTIQ, are not recorded in the CRM sufficient to enable analysis. It is possible to record date of birth (DOB), gender and sexuality factors in the CRM, but DOB cannot be reported on yet and recording of LGBTIQ status is too low to report on at this stage.
Since October 2018, data fields showing primary spoken language, country of birth and whether an interpreter was required have been reported on; however, virtually all records are blank for these fields. For example, of the 16,714 cases created in the CRM between October and December 2018, 98 per cent of the ‘primary spoken language’ fields, and 99 per cent of the ‘interpreter required’ fields are blank. These statistics, particularly the former, do not correspond to evaluation evidence from fieldwork that indicates The Orange Door is servicing clients from multicultural backgrounds.
The Orange Door has recruited practitioners from diverse backgrounds and language skills, noting that language is only one aspect of inclusion. Inclusive practice is still dependent on the practitioner’s knowledge of the different dynamics of family violence in cultures and practice:
'We have clients from diverse backgrounds who are matched to workers that suit that background where possible. We have Mandarin, Farsi-speaking workers, Aboriginal and Maori workers – that said, the experience of diverse clients depends on the skills of the practitioner.' – Practitioner interview
The Orange Door also regularly uses interpreters to support service delivery for clients who do not speak English. However the use of translators and interpreters can be problematic when translating terms such as ‘family violence’, and in insuring trust in the fidelity of the translation particularly in small communities where confidentiality may also be an important consideration. This is a well known challenge in this space and was reflected by FSV, stakeholders and practitioners during interviews.
'Regularly using a translator, maybe once a month (phone interpreter can be clunky and booking them can be a challenge), in-person ones are often from their [the client’s] community so there may be a conflict. Most clients are quite reluctant because they think it’ll be someone in their community.' – Practitioner interview
Community awareness of the role of The Orange Door
The Orange Door is considered physically visible in terms of street frontage, branding and information materials. However, in terms of the role of The Orange Door, at this early stage of implementation, there was evidence of only emerging awareness of The Orange Door by the broader community.
Information about referrals being made to The Orange Door indicates that there is some awareness of the role of The Orange Door, at least by services who have in the past referred to Child FIRST or family violence services (ie L17s or referrals from professionals). Over time, awareness of the role of The Orange Door would be expected to increase amongst other universal services (eg health professionals, schools).
The role of The Orange Door as an intake and assessment service only is not well understood, even by referring agencies (at this point in time). Practitioners reported referrals being received for a range of issues that were not directly related to child wellbeing or family violence issues. For examples, housing or homelessness problems in the absence of family violence or respite issues for families with a child with disability[7]. It is unclear if this lack of awareness of the role is time sensitive (and only evidenced in this early stage of implementation) or if this lack of clarity over the role will persist well beyond the first year of operations.
In terms of the general community awareness, there is evidence that clients also self-refer for a range of difficulties unrelated to family violence or child wellbeing issues. This would indicate a lack of awareness of the role of The Orange Door. However, it may also indicate a lack of appropriate or accessible social support systems in the area and a desire by people having difficulties to try any service that appears to provide assistance to people. Awareness in the potential client groups for The Orange Door requires validation through direct client feedback before conclusions can be drawn on the awareness of the role of The Orange Door.
There has been some feedback that there is even less awareness of The Orange Door in diverse communities:
'Never heard of an Aboriginal service referring people onto The Orange Door. Aboriginal services aren’t really aware of who we are and what we do.' – Aboriginal practitioner
This would be an area for further validation and exploration in future evaluations. It is reasonable to expect in the early stages of implementation that awareness of the service would not have reached all client sub-groups.
Key finding 27:
The Orange Door areas have been established in locations that are visible and accessible for most clients and in close proximity to community service providers and public transport. There are some challenges for some clients to access some of the physical locations (e.g. not on major transport route for some locations in the catchment)
Key finding 28:
The maturity of The Orange Door has meant that some access options, in particular outreach and publicly identifiable access points, have not been operationalised at the time of this evaluation and will be established in line with the planned roll out
Key finding 29:
The physical space at The Orange Door appears to be broadly functional and fit for purpose and FSV has undertaken significant work on the facilities. However, some safety concerns remain and have been identified to FSV during the course of this evaluation
Key finding 30:
The role of the Service System Navigator has not been sufficiently defined and understood by The Orange Door workforce to enable development of service system pathways and connections at the early stage of implementation. The focus of the role will shift from operations to the service system once operational issues are resolved
Key finding 31:
Access via phone could be improved during business hours with the implementation of a message bank that would operate when all lines are busy or the call is not answered. It is understood that this is part of a broader program of IT and infrastructure upgrades planned by FSV
Key finding 32:
Data limitations prevent us making evaluative judgements on whether The Orange Door is accessible and responsive to the needs of clients with diverse needs. Further investigation is required
Key finding 33:
The physical locations and branding of The Orange Door support community awareness of the role of The Orange Door. There is evidence of emerging understanding of the role as an intake and assessment service (notably by those organisations who had previously referred to family violence or Child First services).
To what extent has The Orange Door ensured clients receive information and options that respond to their needs and enable informed choices?
As discussed in Section 4.3.2, The Orange Door is designed to provide clients with information to enable client agency and choice. This information is intended to help people to understand their risk, prioritise needs and understand options for support.[8]
Evidence from fieldwork indicates that practitioners are not aware of guidance about how much information should be shared with clients in which circumstances. At this early stage, this has caused them to err on the side of providing less information rather than more information. The extent of provision of information to clients throughout their journey through The Orange Door is outlined in Table 5 below.
Table 5: Information provided to clients
| The Orange Door function | Information provided |
Description |
|
Access
Screening, identification and triage
|
Limited[9] |
With the exception of self-referrals and L17s, clients are typically not aware that they will be or have been referred to The Orange Door until a practitioner contacts them (as intended by the service model). This can minimise frustration that may arise due to lags from referral to first contact, however, it may also lead to further escalation of risk if clients perceive that nothing is happening in relation to their needs.[10] Feedback from client interviews indicates that they received minimal information about The Orange Door when first referred to the service. Clients reported that they were not always clear on what The Orange Door did or how the service was relevant to their situation. |
| Assessment and planning | Dependent on case type |
The extent of information provided to clients is based on:
|
|
Connection to services Service response |
Requires further data |
Based on evidence from fieldwork, the information provided to clients when they are allocated or referred to services primarily relates to what the service will involve. As discussed in Section 4.2.2, in some cases, clients may remain in contact and receive support from The Orange Door practitioners following their connection with services. Over half of cases are closed without access to support from The Orange Door or connection to external services (see Section 4.2.1). It is not clear what information clients receive in these circumstances. |
|
Review and monitoring |
Limited |
Evidence from fieldwork indicates that there was no systematic flow of information to/from clients following connection to services. On an ad hoc basis, clients appeared to contact The Orange Door practitioner, however, this did not appear to occur frequently. |
Further analysis on client choices and information sharing can be found in Sections 4.3.2, 7.1 and 7.2. Additional data on the experiences and views of clients will be required to make further conclusions.
Key finding 34:
While sharing of information about clients and service within The Orange Door appears to be occurring, there appears to be limited information is shared with clients of The Orange Door at this point in time. However further data is needed to validate the frequency, amount and type of information shared, and if clients perceive that information provided meets their needs
How is The Orange Door working to keep perpetrators in view to keep women and children safe?
Information sharing informs risk assessments and risk planning
The Orange Door collects and analyses information about clients from a range of sources. These include: clients themselves; police; CIP; professionals and other referrers; home agency databases; and CRM. This information is used by practitioners to assess the risk of family violence, assess child safety, wellbeing and development concerns and to keep perpetrators in view. This not only involves collecting information from external sources, but also multidisciplinary collaboration to provide rapid responses to perpetrators’ use of violence.[11]
A key component of keeping perpetrators in view is through access to critical information which allows workers to assess the risk posed by a perpetrator of family violence. A number of reforms help facilitate this, and help to enable an integrated approach, including:
- The Family Violence Information Sharing Scheme (the scheme) was created under Part 5A of the Family Violence Protection Act 2008. The scheme enables information to be shared between selected government agencies and funded organisations (including The Orange Door), prescribed as ‘information sharing entities’ or ‘risk assessment entities’ in order to assess or manage family violence risk. Consent does not need to be given by perpetrators for their information to be shared by information sharing entities, or consent of alleged perpetrators if shared by risk assessment entities.[12]
- Under Part 5B of the Family Violence Protection Act 2008, workers in The Orange Door are able to collect, use and disclose confidential information with other workers where relevant to delivering The Orange Door services, “in a way that gives precedence to safety and wellbeing over privacy.”[13]
The evaluation found a lack of understanding about what ‘keeping perpetrators in view’ actually means in the context of The Orange Door service environment. This is likely to be a point in time issue reflecting the emerging perpetrator service practice, variation in practice across The Orange Door areas at this point in time, a lack of a definition of ‘keeping perpetrators in view’ in foundational documents, and the innovation of the integrated model and how perpetrator services could be integrated in a way to keep women, children and others experiencing family violence, safe. As such, we have examined mechanisms that go to the sharing of information about perpetrators behaviour that can be used to assess risk, stay in contact with perpetrators and engage them in interventions to change their behaviour as part of the evaluation.
Information sharing informs risk assessments and risk planning
The three key ways that information about perpetrators is shared in practice are the use of CIP, history checks on CRM and employing agencies’ databases and multidisciplinary practice.
Central Information Point
The development of the CIP is in response to the recommendations of the RCFV. CIP was established to provide frontline workers with timely access to critical information for the assessment and management of family violence. The CIP allows representatives from Court Services Victoria, Victoria Police, Corrections and DHHS to consolidate critical information about perpetrators of family violence into a single report within hours[14] to enable assessment on the risk posed by a perpetrator of family violence.
To request a CIP, practitioners in The Orange Door typically need to get approval from a team leader or practice lead. There appears to be some inconsistencies in the extent to which CIP requests need to be justified, with some leaders “waving them through” while others “will grill [practitioners]”. Evidence from evaluation fieldwork indicates that some practitioners believe that there is a cap of five CIP requests per day for each area, however, the CIP team is understood to be prepared for a greater number of requests. Practitioners reported a lack of clarity on when and how a decision should/could be made to initiate a CIP request. CIP reports are generally made in the assessment and planning stage, but also in some cases during screening, identification and triage.
'When you have that history [from CIP] it changes your perspective and you can safety plan more vigilantly.' – Practitioner interview
There has been strong evidence from practitioners at each The Orange Door during the evaluation that the CIP has been effective for improving risk assessment and outcomes for clients, particularly those who were previously unknown to The Orange Door. Practitioners reported that having access to information from across the service system has facilitated more accurate assessment and planning for clients, based on having a more fulsome picture of the current situation and history.
Box 5: Use of CIP in The Orange Door
In the first half of 2018-19, the four areas of The Orange Door areas together recorded an average of just under 10 CIP requests per business day.[15] Figure 11 shows the CIP requests created per month for each area in that period.
Figure 11: Number of CIP reports created (as recorded on the CRM) by The Orange Door area, July – December 2018
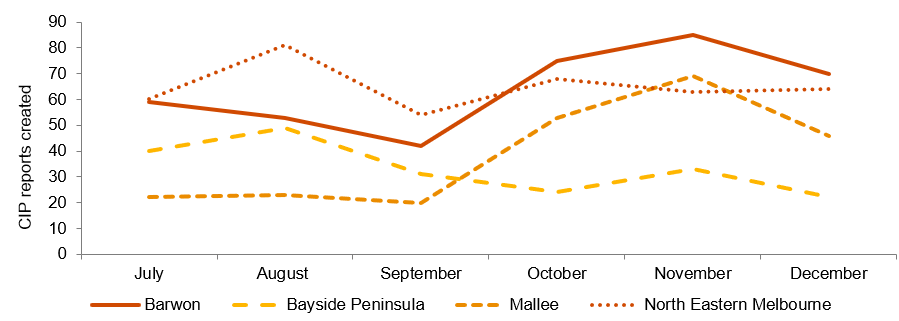
Source: PwC analysis of CRM data provided by FSV. Note that The Orange Door commenced in NEMA in July 2018.
There appear to be some inconsistencies in how CIP is used in each area. Practitioners acknowledged that the CIP is specifically for family violence cases, but cited child wellbeing cases where it would have been useful to inform risk and needs assessments. Some practitioners stated that they had used CIP when the case only peripherally related to family violence (which is consistent and allowed within the legislation). One other inconsistency that practitioners referred to was whether information gained from a CIP request could be shared with affected parties, eg to inform safety planning. The legislation does allow for sharing of perpetrator information with the victim survivor to assist in managing their safety, however practitioners reported variation in their understanding of if this was allowed, and if and when they shared information. The evaluation found that while CIP is considered a positive tool for The Orange Door and there is FSV guidance material regarding the use of CIP, there is a need for greater operational clarity and consistency over when, how and how often CIP requests could be made to assist practitioners at the operational level.
Case study of CIP use
A CIP request was made when a practitioner was concerned about the risk a perpetrator posed to a client. The client has disclosed that there was a history of family violence for her and also a previous partner of the perpetrator. The CIP report indicated an extensive history of family violence perpetrated by the man with numerous women dating back a decade. Importantly, this information indicated a number of instances when the perpetrator offended at the location a woman had parked her car while away from home. This information immediately changed the safety planning the practitioner did with The Orange Door client with a much stronger focus on safety while travelling to and from work and other known locations (shops, child care, etc.). –real example reported by practitioners
CRM
CRM is expected to be used by practitioners to capture, store and record all case information. It also integrates with a number of systems, including the L17 portal, CIP and the TRAM, and in future, others will be built in.[16]
Over time, CRM will build up a considerable amount of client and case data that can be used to inform risk assessments. While CRM’s recent introduction means that historical information currently held is limited, practitioners provided some examples where searches for clients or related family members across CRM had yielded additional information that would have been otherwise unknown. As it is rolled out across all DHHS areas and through progressive upgrades delivered and planned by FSV, CRM will enable quicker and more automated information sharing. This should speed up searches of perpetrators’ historical cases, meaning that CIP can be deployed only on more critical cases.
Multidisciplinary practice
Multidisciplinary practice is a fundamental aspect of The Orange Door. There is evidence that The Orange Door workforce is collaborating on assessment and planning supported by physical colocation and personal working relationships. The collaboration is inconsistent and not yet embedded within practice, especially when working with perpetrators. In particular:
- For some family violence-focused practitioners (who sometimes call themselves ‘women’s workers’), there is an ideological barrier to sharing information with anyone who is perceived to be ‘helping the male perpetrator’. This appeared to stem from their perceived priority to help the victim survivor above anything else, and viewpoint that providing information to a ‘men’s worker’ may increase risk to their client.[17] Some practitioners working with perpetrators reported that they would prefer not to know about the victim survivor’s circumstances in case they inadvertently disclosed details to the perpetrator when speaking to them.
- Some practitioners do not yet clearly understand or are aware of the FSV Support and Safety Hubs: Perpetrator practice guidance (April, 2018) on when and how information should be shared between victim survivor and perpetrator focused practitioners[18]. This means that practitioners are generally taking a risk-averse approach to sharing information at this point in time.[19]
- Multidisciplinary practice was most evidently displayed by the Aboriginal practitioners at The Orange Door, who provided support to both the victim survivor and perpetrator in most cases.[20] According to Aboriginal practice leads and specialist family violence practice leads, this is because the tradition of providing support to Aboriginal families tends to be community-led, involving those outside the family to assist the victim survivors and perpetrators. As such, the integration of perpetrator services with victim survivor services is aligned with existing practice.
- Perpetrator interventions beyond Men’s Behaviour Change (MBC) programs are not yet matured. During fieldwork, MBC programs were the only intervention allocated to non-Aboriginal clients that practitioners reported. The wrap-around nature of Aboriginal services means that perpetrators are provided support from the same service that are supporting victim-survivors, and that support involves cultural connection and individual counselling rather than just behaviour change groups.
Insights gained from client interviews for this evaluation regarding the role of The Orange Door in keeping perpetrators in view were limited. One participant expressed gratitude that The Orange Door had reached out to their partner as they were keen for their partner to receive support and assistance. This was viewed by the client as a sign that The Orange Door was non-discriminatory.
As engagement with perpetrators and/or data that demonstrates the numbers of perpetrators engaged through The Orange Door is currently limited (also see Sections 4.1.1), further investigation into how information is shared to keep perpetrators in view is required before making firm evaluation judgements on whether The Orange Door is contributing to keeping perpetrators in view.
Use of information to inform service responses for perpetrators in The Orange Door
Keeping perpetrators in view also means providing them with opportunities to change their behaviour by connecting with services that assist in holding them accountable for their actions. This involves assessing perpetrators’ preparedness for change and connecting them to services to stop or reduce their use of violence and improve their parenting.[21]
Service responses for perpetrators is determined by the information collected as part of the assessment and planning stage function of The Orange Door. Thus, the success and limitations of that stage assist and constrain information sharing in the later ‘connection to services’ stage of The Orange Door service delivery. CRM data on the connection to services function is currently limited and appear to be inconsistently recorded. Despite the data limitations, qualitative data collected as part of the evaluation indicate that there are concerns about information sharing specific to that function:
Contact with men is limited. Practitioners working with perpetrators stated that they tried to call three times over three days and if they were not successful in getting in touch, they closed the case. In general, practitioners did not attempt to use contact methods other than phone. If they could not contact the perpetrator, assessing their preparedness for change is difficult, and connecting them with a service mostly impossible.[22]
[We] don’t actually get on to many clients; there’s only a few [over their time at The Orange Door] that I’ve actually had real conversations with” – Practitioner interview
- One perpetrator focused practitioner often collaborates closely with a family violence-focused practitioner and reported that the information collected through CIP and other sources is useful to inform safety planning even if they are unable to get in contact with the perpetrator.[23]
- Some practitioners reported their concerns that there is no senior practitioner with whom to consult specific to their practice of working with perpetrators of family violence. Ironically, this has the potential to improve information sharing through multidisciplinary practice if these practitioners consult with the advanced family violence practice lead, however, this does not always occur as yet. While this is not the intent of the role, there is a perception in the workforce that the advanced family violence practice lead specialises in victim survivor practice.
- CRM does not currently record the outcome or output of the service response beyond The Orange Door. Moreover, data recording of allocations of core services to clients and referrals to non-core services on the CRM is currently poor. This means that it is difficult for practitioners to track the use of service responses by perpetrators and the success of these interventions.[24]
Further research on service responses, involving higher quality CRM data, will be required to provide insights into whether service responses for perpetrators are tailored based on shared information.
Key finding 35:
There is an evolving understanding about what it means at an operational level for The Orange Door to ‘keep perpetrators in view
Key finding 36:
CIP has been effective for improving risk assessment and outcomes for clients, particularly those who were previously unknown to The Orange Door. Operational clarity is needed for the workforce as to when, how and how often CIP request can be made
Key finding 37:
The CRM has the potential to be a source of client and case data that can inform risk assessment, however data recording is not yet adequate to effectively support this function
Key finding 38:
The Orange Door workforce is collaborating on assessment and planning supported by physical colocation and personal working relationships. The collaboration is inconsistent and not yet embedded within practice, especially when working with perpetrators. Collaboration on assessment and planning is most evidently displayed by Aboriginal practitioners and aligns with their community-led approach to service provision
Key finding 38:
CRM data on connection to services are limited. As such, the evaluation was unable to determine if service responses for perpetrators are tailored based on shared information
Key finding 39:
Support to perpetrators by The Orange Door is limited as it is dependent on their voluntary engagement with the service. Many do not respond to attempts by The Orange Door to contact them. This was anticipated and is reflected in the guidance documents for The Orange Door
[1] FSV, ‘Support and Safety Hubs: Statewide Concept’, July 2017.
[2] FSV, ‘Support and Safety Hubs: Frequently Asked Questions – Public Version’, May 2018.
[3] It is possible that this increased transparency between The Orange Door and the client to ensure accuracy and comprehensiveness of information. However, during this evaluation, this was considered by practitioners not to be appropriate.
[4] FSV, Support and Safety Hub Statewide Concept’, July 2017.
[5] Qualitative evaluation data from fieldwork
[6]
[7] Please note, it is recognized that respite for children with disability may also be a child wellbeing concern and as such, fall within the scope of The Orange Door services.
[8] FSV, ‘Support and Safety Hubs: Concept paper’, July 2017.
[9] There are however a range of written information pamphlets etc. that have been prepared, tailored to client groups and available at The Orange Door.
[10] Qualitative evaluation evidence from fieldwork
[11] FSV, ‘Support and Safety Hubs: Service Specifications’, April 2018.
[12] FSV, ‘Support and Safety Hubs: Frequently Asked Questions’, 30 May 2018.
[13] Family Violence Protection Act 2008: Part 5B – Information sharing relating to Support and Safety Hubs: 184
[14] State Government of Victoria, ‘The Central Information Point’, 2018.
[15] PwC analysis using CRM data provided by FSV.
[16] FSV, ‘Support and Safety Hubs: Service Model’, April 2018.
[17] Qualitative evaluation evidence from fieldwork
[18] FSV Support and Safety Hubs: Perpetrator practice guidance, April 2018
[19] Qualitative evaluation evidence from fieldwork
[20] Qualitative evaluation evidence from fieldwork
[21] FSV, Support and Safety Hubs: Service Specifications’, April 2018.
[22] Qualitative evaluation evidence from fieldwork
[23] Qualitative evaluation evidence from fieldwork
[24] Qualitative evaluation evidence from fieldwork
Updated