Strategic priority 2: Facilitate consistent and collaborative practice
Framework organisations must collaborate to keep victim survivors safe and hold perpetrators in view. This includes sharing information to better understand and act on family violence risk. Information sharing helps practitioners make better practice decisions and provide the right support to people experiencing family violence.
Collaboration highlights from 2024-25
|
Collaboration case study: mental health and alcohol and other drugs Mental health and alcohol and other drugs (AOD) services across Victoria nominated specialist family violence advisers (SFVAs) to represent their member agencies on Risk Assessment and Management Panels (RAMPs). This was made possible through collaboration between DFFH, SFVA statewide coordinators, the Centre for Mental Health Learning, the Victorian Alcohol and Drug Association (VAADA), the SFVA leadership group, and the Department of Health. This work involved:
This initiative supported RAMPS to draw on SFVA expertise in high-risk cases. |
Collaboration by the numbers
Practitioners need access to timely and relevant information to assess and manage risk and plan for victim survivor safety.
Table 1: Collaboration and information sharing
| In 2024–25, there were: | The aim was to: |
| 105,242 MARAM risk assessments conducted using MARAM tools available on the platforms TRAM and SHIP | Identify and assess the level of risk experienced by victim survivors. This includes their risk of experiencing further family violence |
| 32,352 safety plans made using MARAM tools available on the platforms TRAM and SHIP | Enhance the safety of people experiencing family violence. Practitioners tailor plans to victim survivors’ needs and circumstances. This includes setting out practical steps they can take to protect themselves and children |
| 5,422 CIP comprehensive reports delivered | Provide consolidated risk-relevant information actions. This supports risk assessment and management |
| 4,678 CIP brief reports delivered | Provide practitioners with a subset of critical risk-relevant information for immediate decision making |
| 84,677 instances of information sharing under FVISS and CISS by centralised information sharing teams within government | Provide Information Sharing Entities with information to assess family violence risk and support safety planning |
Data source: Department of Families Fairness and Housing.
Note: Above figures reflect data captured through specific reporting platforms such as Client Records Management (CRM), TRAM and SHIP. They do not represent all information sharing, risk assessments and safety plans completed across the system.
MARAM Annual Survey: collaboration insights
Most frontline workers (92%) who responded to the survey were confident or very confident to collaborate with other practitioners across the service system.
However, results show there is more we need to do to support organisations to optimise their collaborative work in managing risk.
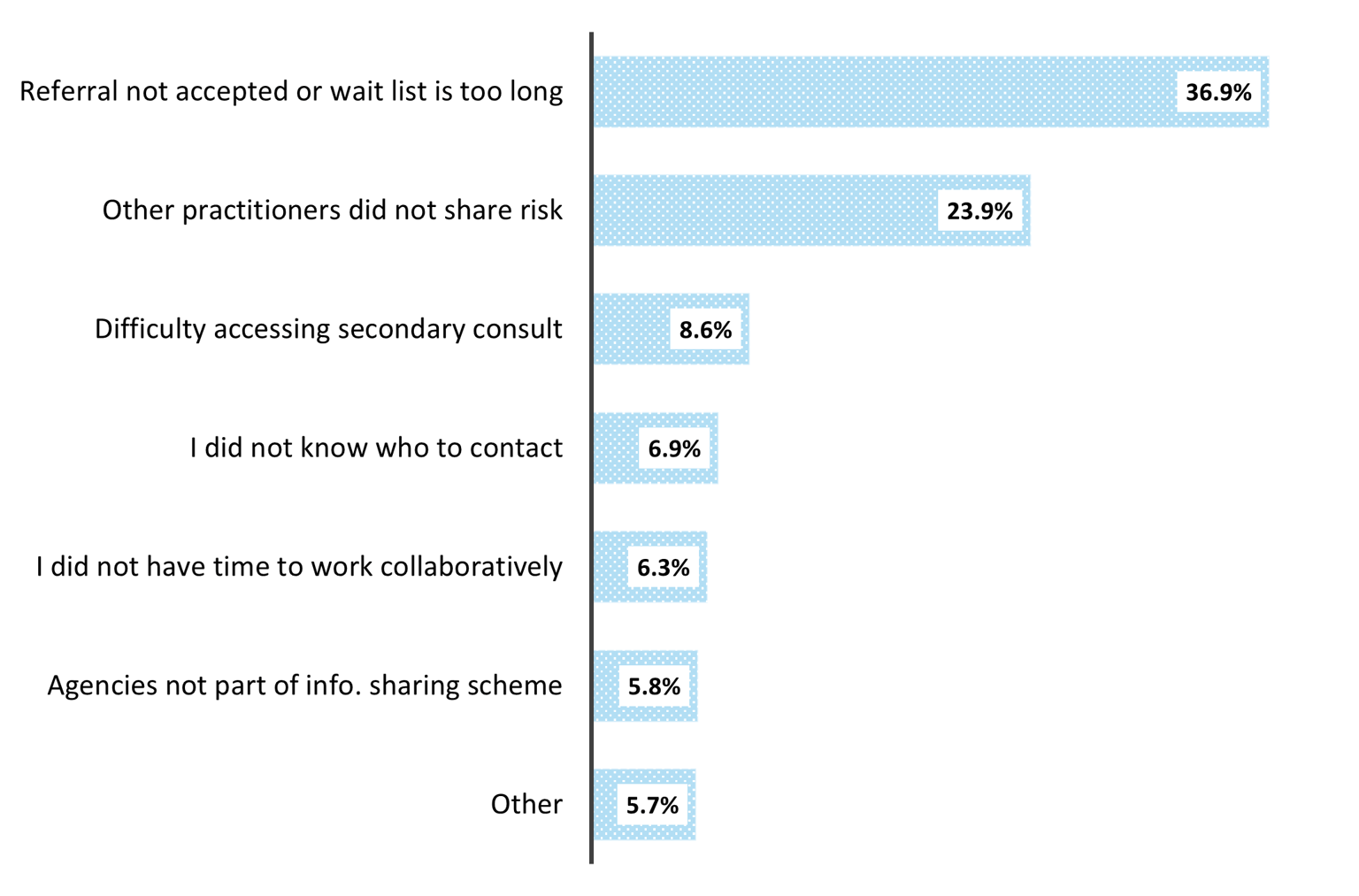
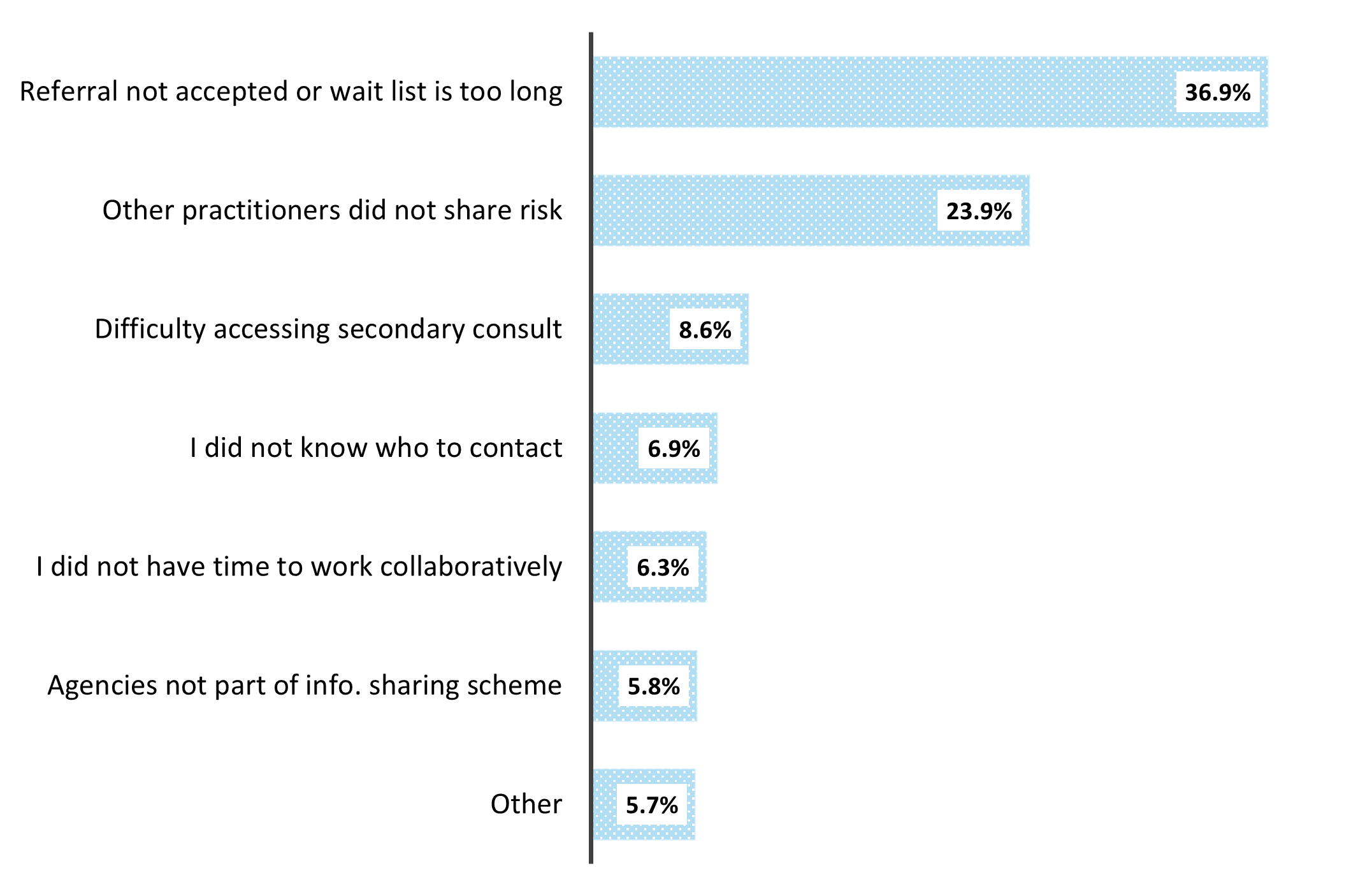
More than a third of participants stated that long waiting lists and referrals being rejected are barriers to collaboration with other agencies. Figure 2 sets this out.
Figure 2: Barriers to collaboration
{kind=link}
Survey results show that most frontline workers are aware of FVISS and how it applies to their work (91%). They continue to use it to support their clients:
- consistent with 2023–24, 26% of participants shared information under FVISS more than once a week, with 29% sharing at least once week to once a month
- more than half of participants said they proactively shared information for either every client (16%) or most clients (36%) where family violence is identified
- 57% of participants said they always or often use risk-relevant information from other organisations to support clients.
However, almost one-third (30.7%) of participants said they rarely request or share information under FVISS. In addition, 14% said they had never used the scheme to share information. This was more pronounced in universal services. For example, in the health sector, almost a quarter of participants had never shared under FVISS. For comparison, just 10% in the human services sector had never shared under FVISS.
The biggest barrier to sharing information was delays in receiving information under the schemes (24%), with response times likely to be impacted by the growing demand for information requests and current resourcing to support this function. A lack of cross-sector understanding was also highlighted as a barrier (17%).
Case study: Collaborative information sharing practice Tracey is a case worker in a therapeutic program supporting adult victim survivors. She was allocated Maria, a mother of 2 children, Ava and Oscar. Maria had recently ended her relationship with Anthony and there was an active exclusionary Intervention Order in place protecting her and the children. Recognising the need to tailor her therapeutic approach in line with the family’s lived experiences, Tracey identified that understanding the children’s history with Child Protection would be important in shaping her work. With Maria’s support, Tracey submitted a request to obtain a summary of past involvement relating to Ava and Oscar and information about Anthony, the children’s biological father. Upon review, the team identified that Anthony had two other children from a previous relationship. He also had an extensive history of using family violence towards partners and children and had previously participated in a Men’s Behaviour Change Program (MBCP). This information was shared with Tracey to inform her family violence risk assessment and support a holistic understanding of the family’s circumstances. Tracey also contacted the MBCP, who confirmed that Anthony remained engaged with the program. This created an opportunity for collaborative case coordination, ensuring services were aligned in their approach to safety and accountability. Drawing on the shared information, Tracey worked with Maria, Ava and Oscar to develop a strengths-based safety and support plan, incorporating both immediate safety strategies and longer-term therapeutic interventions to promote recovery and wellbeing. Note: Names have been changed. |
Collaboration plans for 2025–26
- In the Health portfolio, the Royal Women’s Hospital will develop the Trauma and Violence Informed Workplace project. The project will be evaluated by the University of Melbourne, to be scalable after 18 months to all public health services. Safer Care Victoria will support the Department of Health to develop new service and funding models for Gamblers Help services. This will ensure future community health organisations are ready to align with MARAM and information sharing reforms.
- The Corrections and Justice Services portfolio will work with Technology Solutions to enhance their IT family violence solution that was implemented in April 2025. This comprehensive platform is used for recording and storing FV information, tracking MARAM processes and uploading of risk assessments and other documentation. Once fully implemented across both Community Correctional Services and Corrections Victoria, the system will work as a mechanism for internal information sharing.
Updated